Article Text

Abstract
BACKGROUND There is a lack of suitable models for testing of therapeutic procedures for gastro-oesophageal reflux disease. Endoscopic sewing methods might allow the development of a new less invasive surgical approach to treatment of gastrointestinal disorders.
AIMS To develop an animal model of gastro-oesophageal reflux for testing the efficacy of a new antireflux procedure, endoscopic gastroplasty, performed at flexible endoscopy without laparotomy or laparoscopy.
METHODS At endoscopy a pH sensitive radiotelemetry capsule was sewn to the oesophageal wall, 5 cm above the lower oesophageal sphincter, in six large white pigs. Ambulant pH recordings (48–96 hours; total 447 hours) were obtained. The median distal oesophageal pH was 6.8 (range 6.4–7.3); pH was less than 4 for 9.3% of the time. After one week, endoscopic gastroplasty was performed by placing sutures below the gastro-oesophageal junction, forming a neo-oesophagus of 1–2 cm in length. Postoperative manometry and pH recordings (24–96 hours; total 344 hours) were carried out.
RESULTS Following gastroplasty, the median sphincter pressure increased significantly from 3 to 6 mm Hg and in length from 3 to 3.75 cm. The median time pH was less than 4 decreased significantly from 9.3% to 0.2%.
CONCLUSIONS These are the first long term measurements of oesophageal pH in ambulant pigs. The finding of spontaneous reflux suggested a model for studying treatments of reflux. Endoscopic gastroplasty increased sphincter pressure and length and decreased acid reflux.
- gastro-oesophageal reflux
- endoscopic gastroplasty
- manometry
Abbreviations
- GOR
- gastro-oesophageal reflux
- GORD
- gastro-oesophageal reflux disease
- LOS
- lower oesophageal sphincter
Statistics from Altmetric.com
A variety of models have been proposed for studying gastro-oesophageal reflux (GOR) but all have certain drawbacks. Surgical models, in which the lower oesophageal sphincter (LOS) is excised or incised, tend to disrupt the oesophageal sphincter anatomy in an unphysiological manner. Pharmacological models can only be used in short term experiments. Long term ambulant measurement of distal oesophageal acid exposure with continuous pH monitoring (the current gold standard investigation for gastro-oesophageal reflux disease (GORD)) is also difficult to achieve in animal studies.
The application of sewing methods at flexible endoscopy1has allowed the introduction of new less invasive approaches to the treatment of reflux, including endoscopic gastroplasty, with demonstrable improvement in manometric LOS function in animal studies.2 It would thus be desirable to evaluate the potential efficacy of endoscopic gastroplasty by testing its ability to reduce distal oesophageal acid exposure in a reflux model.
The primary aim of this study was to develop a long term, in vivo, animal model of GOR which is ambulant and allows repeat measurements of distal oesophageal acid exposure by long term pH monitoring. Another aim was to test the efficacy of endoscopic gastroplasty in reducing distal oesophageal acid exposure in this model.
Materials and methods
MATERIALS
Endoscopic sewing machine
An endoscopic sewing machine, which can be used to place sutures at flexible endoscopy, was used in this study.2 It can be mounted on any flexible endoscope with a biopsy channel of 2.8 mm or greater. The essential components of the machine are the suction cavity and a hollow needle holding the suture material. A suture can be placed through the full thickness of the gastrointestinal tissue with the endoscopic sewing machine.3
Knot tying
A knot pusher, backloaded through the biopsy channel, was used to tie knots at flexible endoscopy. The individual half hitches were tied extracorporeally, outside the mouth and pushed down with the knot pusher while maintaining view with the endoscope.4Four half hitches were used to tie a secure knot by this method.
Cutting methods and suture materials
A flexible thread cutting device was used to cut the sutures.5 The cutting device was passed via the biopsy channel and the sutures backloaded through the side holes of the device. Cephald traction on the cutter cuts the sutures close to the knot.
3/0 nylon suture material was used in this study. Nylon was chosen because the antireflux procedures required a non-absorbable suture material to hold the tissues together for a long period and the monofilament structure reduced surface friction, thus facilitating suturing and knotting techniques.
Overtubes
An oro-oesophageal overtube (Keymed, Southend, UK) was used to facilitate the multiple intubations that were necessary to place sutures and tie knots.
pH sensitive radiotelemetry capsule
The body of the radiotelemetry capsule (Type 7006, Remote Control Systems Ltd, Amersham, Bucks, UK; fig 1) is made from a glass cylinder measuring 25 mm long and 7.6 mm in diameter. The pH sensitive glass tip is fused on to the end of the glass cylinder, which contains a single thick film semiconducting chip, a power source, and a transmitting aerial. The disposable reference cap is attached to the body of the radiotelemetry capsule and houses the components of a reference cell: an Ag/AgCl disc, a reservoir of saturated NaCl, and a cotton thread link that limits the diffusion of NaCl around the capsule. The power source is a 1.35V mercury battery (RM212) which lasts approximately 2000 hours. The pH sensitive radiotelemetry capsule transmits at a frequency which corresponds to changes in the pH of its surroundings. The frequency response is linear over the range of pH 1 to pH 10. Prior to implantation, the radiotelemetry capsule was calibrated with buffers of pH 1.0 and pH 7.0 at 37°C.
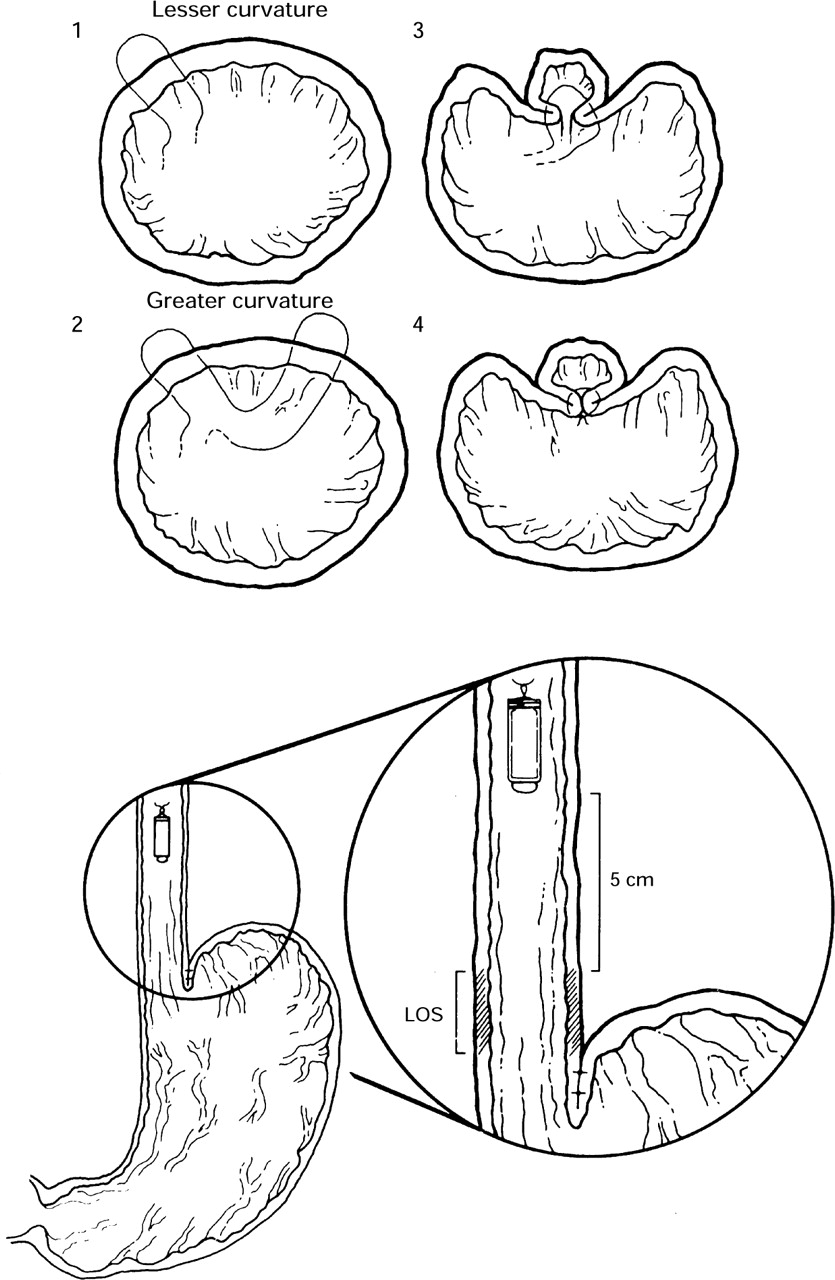
Endoscopic gastroplasty. Diagram indicates transverse and longitudinal section through the oesophagus and stomach to indicate the placement of stitches and site of implantation of radiotelemetry capsule. Two stitches are placed immediately below the cardio-oesophageal junction; the tissue is pulled together and tied with four half hitches. A separate pair of stitches is placed 1 cm below the first. There are several possible mechanisms by which endoscopic gastroplasty might improve reflux: it creates a neo-oesophagus out of gastric tissue, thus increasing the exposure of the lower oesophageal sphincter (LOS) to positive intra-abdominal pressure; it may increase lower oesophageal sphincter pressure by placing a tuck in the muscle layer at the lower end of the sphincter; it may make the angle of this more acute; by decreasing the potential for relaxation of the gastric sling fibres distension induced lower oesophageal sphincter relaxation may be reduced.
Animal studies
Female pigs of Large White breed were studied. They weighed between 20 and 30 kg (median weight 24 kg) and were between 10 and 12 weeks old. The experimental design was approved by the Home Office (Project Licence number: PPL 70/03491) and adhered toGuiding Principles in the Care and Use of Animals.
METHODS
Anaesthesia
Pigs were anaesthetised with halothane, intubated, and anaesthesia maintained with a mixture of halothane, nitrous oxide, and oxygen. Continuous monitoring of vital signs and rectal temperature were performed during the anaesthesia.
Station pull through manometry—measurement of LOS pressure and length
Oesophageal manometry was performed using a triple lumen PVC catheter continuously perfused with water at a rate of 0.5 ml/min using a pneumohydraulic pump.6 The manometry catheter was passed through the mouth into the stomach and then withdrawn at 0.5 cm increments. The pressure measurements at each station were recorded by means of a penchart recorder, the data obtained by electrically isolated pressure transducers connected to the manometry catheter. The pressure traces were analysed to determine the LOS pressure, length, and position. These measurements were made before and immediately after the endoscopic gastroplasty in the anaesthetised animal. Each measurement was repeated twice.
Continuous ambulatory pH measurement
The endoscopic sewing machine was used to attach a pH sensitive radiotelemetry capsule to the oesophageal wall, 5 cm above the manometrically defined LOS. Two stitches were placed in the oesophageal wall and then the sutures were passed through the loop in the reference electrode of the radiotelemetry capsule. The radiotelemetry capsule was run down over the thread to the desired position in the oesophagus and each of the two threads was tied securely to the oesophageal wall with four half hitches. We were careful to arrange the attachment of the capsule so that the sensor at the distal end of the capsule when fully extended from its attachment was 5 cm above the upper border of the lower oesophageal sphincter measured at manometry.
A jacket containing the aerial belt and the recorder was placed around the pig’s torso. After recovering from the anaesthesia, the pig was allowed to walk freely in its pen while wearing the jacket. Continuous 48 hour recordings of distal oesophageal pH were obtained in an ambulant setting in this manner. After 48 hours the recorder was removed from the jacket and the data downloaded into a computer. The recorder was then replaced into the jacket and further 48 hour recordings were obtained. No anaesthesia or sedation was required to change the recorder. At the end of the study, the radiotelemetry capsules were recovered and checked for postcalibration drift.
Operation—endoscopic gastroplasty
Endoscopic gastroplasty was performed using the endoscopic sewing machine by placing sutures below the gastro-oesophageal junction2 (fig 1). To facilitate the procedure, an oro-oesophageal overtube was placed in the oesophagus at the beginning of the procedure. The endoscopic sewing machine was then advanced just below the gastro-oesophageal junction; a fold of tissue was sucked into the suction cavity and a transmural stitch was placed. The suture was then reloaded on to the machine and a second stitch placed at the same level, but opposite to the previous stitch. The suture ends were then tied to create a gastric tube. By placing further sutures just below the first knot a neo-oesophagus was created.
Histopathology
Biopsy specimens of the distal oesophagus were obtained at flexible endoscopy for histological analysis.
Recovery and feeding
Oral feeding began once the animal had fully recovered from anaesthesia, which was usually within 60 minutes of reversal.
EXPERIMENTAL DESIGN
Preoperative assessment and preparation
Following anaesthesia, endoscopy was performed to assess the distal oesophagus and gastro-oesophageal junction. A manometry tube was then passed per orally into the stomach and station pull through manometry was performed. After defining the position of the LOS manometrically, the radiotelemetry capsule was implanted into the distal oesophageal wall, 5 cm above the LOS. After recovery, 48–96 hour continuous recordings of distal oesophageal pH were obtained using a digital data logger with an inbuilt telemetry receiver (Medilog 1000, Oakfield Instruments, Oxon, UK).
Protocol alteration on finding spontaneous acid reflux
The preoperative distal oesophageal pH profile was not expected to show pathological levels of reflux—that is, to lie within the normal physiological range for man (pH less than 4 for less than 4% of the time). The initial experimental protocol was then to perform a sphincter (LOS) damaging operation in order to produce pathological reflux and to confirm this by long term, ambulant distal oesophageal pH measurement. Cardioplasty had been chosen as the reflux producing operation. Unexpectedly, the baseline pH profile of all six animals showed values that would be considered pathological in man (table 1). Cardioplasty was therefore not performed, and all animals underwent an antireflux procedure—endoscopic gastroplasty.
The preoperative pH profile of all six animals used in this study
Perioperative procedures and measurements
A week following implantation and prior to performing endoscopic gastroplasty, the radiotelemetry capsules were checked for position at endoscopy and then retrieved by cutting the thread using endoscopic suture cutting forceps (Olympus FS-1K, Keymed, Southend, UK). The endoscopic gastroplasty was then performed. The radiotelemetry capsules were checked for drift, recalibrated, and reattached to the oesophageal wall following endoscopic gastroplasty. The place of attachment was determined by remeasurement of LOS position. The pH capsules were removed and reimplanted after the gastroplasty for three reasons: the capsule might have interfered with the endoluminal suturing; the calibration could be rechecked; and the capsule could be resited at the correct position, 5 cm above the manometrically determined LOS position as these were rapidly growing animals.
Evaluation of antireflux procedure
One week after the endoscopic gastroplasty, endoscopy was performed to confirm the presence of the radiotelemetry capsule and intact sutures. Radiotelemetry capsules were retrieved and tested again for calibration drift. Preoperative LOS parameters and distal oesophageal acid exposure were compared with similar parameters following endoscopic gastroplasty in order to assess the efficacy of the procedure.
STATISTICAL ANALYSIS
The non-parametric Wilcoxon matched pair test was used to analyse the effect of endoscopic gastroplasty on LOS sphincter function and distal oesophageal acid exposure (Statistica for Windows 4.1, Statsoft Inc., 1993). A p value of less than 0.05 was considered significant.
Results
PREOPERATIVE PREPARATION AND EVALUATION
Endoscopic assessment
At preliminary endoscopy, none of the animals showed evidence of oesophagitis or ectasia of the Z line. The porcine cardia features a gastric pouch adjacent to the cardio-oesophageal junction but there was no endoscopic evidence of hiatus hernia. No microscopic evidence of oesophagitis was found in endoscopic biopsy specimens of distal oesophageal mucosa. The radiotelemetry capsules were attached to the oesophageal wall on all six occasions using a double stitch technique and secured with four half hitches per stitch. On one occasion the radiotelemetry capsule became detached at eight hours; this was recognised by the appearance of a gastric pH profile on the recorder (pH less than 2.0 for 90% of the time). The radiotelemetry capsule was retrieved from the stomach at endoscopy and sewn back into the oesophagus.
Manometric measurements
The preoperative station pull through manometry revealed a median sphincter pressure of 3 mm Hg (range 2.3–6 mm Hg). The median LOS length was 3 cm (range 2–3.5 cm). There was no manometric evidence of hiatus hernia.
Measurements of distal oesophageal acid exposure
A total of 447 hours of preoperative recordings was obtained. The median length of continuous recording was 64.5 hours (range 46–140 hours). The recordings were carried out over one week in four animals and over two weeks in the other two animals to check that there was no major alteration in distal oesophageal acid exposure with time in these animals. The median baseline pH was 6.8 (range 6.4–7.3). Each 24–48 hour recording was repeated on two occasions with a 24 hour gap. The median number of reflux episodes over a 24 hour period was 19 (range 8–32) and the longest reflux episode was 70 minutes in duration. The median percentage time pH less than 4 was 9.3% (range 6–11.1%), suggesting that the porcine distal oesophageal acid exposures were at levels that would be considered abnormal in man (table 1).
OPERATION—ENDOSCOPIC GASTROPLASTY
Endoscopic gastroplasty was carried out in all six animals. Four to six stitches were placed in pairs just below the cardio-oesophageal junction. All pairs of stitches were secured with four half hitches tied extracorporeally and pushed through the oesophagus with a knot pusher. The median duration of the procedure was 30 minutes (range 20–40). A retroflexed view of the cardia confirmed that the intended anatomical alteration had been achieved.
POSTOPERATIVE EVALUATION
Endoscopic assessment
Endoscopy performed at one week following endoscopic gastroplasty showed that all the stitches and knots were intact. The pleated anatomical arrangement created by gastroplasty was evident at endoscopy one week after the operation. The stitches and knots holding the radiotelemetry capsule in the oesophagus were identified. In some animals a red nodule with a superficial erosion could be seen at the stitch site. There was no endoscopic evidence of perforation or stigmata of recent bleeding at any of the stitch sites. All radiotelemetry capsules were successfully retrieved at the end of the experiment by cutting the stitch in the oesophagus and pulling the capsule out using retrieval forceps. The radiotelemetry capsules were immediately tested for calibration drift but none was found.
Manometric measurements
Following endoscopic gastroplasty, there was a significant increase in median LOS pressure from 3 (range 2.3–6) to 6 (range 4.5–16) mm Hg (p<0.05). The individual measurements of LOS pressure before and after endoscopic gastroplasty were: 2.3 to 16, 2.8 to 4.8, 5.5 to 6, 6 to 14.5, 3 to 4.5, 2.5 to 5.3. The median LOS length also significantly increased from 3 (range 2–3.5) to 3.75 (range 3–5) cm (p<0.05). The individual measurements of LOS length before and after endoscopic gastroplasty were: 3 to 4, 2 to 3, 3.5 to 4, 3 to 3, 3 to 3.5, 3 to 5.
Measurement of distal oesophageal acid exposure
A total of 344 hours of postoperative recordings was obtained. The median duration of the recording was 48 hours (range 24–96 hours). Following endoscopic gastroplasty, the median percentage time at which pH was less than 4 decreased significantly from 9.3% to 0.2% (range 0–2.9%, p<0.05; fig 2). The number of reflux episodes also decreased from a median of 19 to 2 (p<0.05). Figure 2 shows an example 48 hour pH tracing before and after endoscopic gastroplasty in an animal.

{kind=link}
{kind=link}
Preoperative and postoperative distal oesophageal acid exposure. Endoscopic gastroplasty significantly decreased acid reflux (p<0.05). The top trace shows preoperative 48 hour pH profile and the bottom trace shows postoperative 48 hour pH profile of the distal oesophagus.
COMPLICATIONS AND TECHNICAL DIFFICULTIES
During this study there was no damage to the recording equipment, but the aerial belt had become displaced in one animal and had to be repositioned. Attempts were made to measure the yield pressure of the LOS but the consequent gastric dilatation impaired respiration sufficiently for us to abandon this measurement. Recovery after surgery was immediate; the pigs were eating within an hour of reversal of anaesthesia. All the animals ate normally and gained weight in the week following the operation. There were no deaths or complications such as perforation, bleeding, peritonitis mediastinitis, or pneumonia following either the insertion of radiotelemetry capsules or endoscopic gastroplasty. No intraperitoneal or mediastinal adhesions were seen at postmortem examination.
Discussion
This study is the first to show that pigs reflux acid into the distal oesophagus in amounts that are equivalent to pathological reflux in man.7 Our method has allowed for the first time, documentation of the ambulatory pH measurement of the distal oesophagus in pigs for 24 hours or more. This methodology has permitted us to evaluate a new antireflux procedure by its ability to reduce 24 hour oesophageal pH exposure in a model that does not require prior surgical mutilation of the LOS or other surgical procedures such as gastrostomy.
Several models of GOR or oesophagitis have been reported in the past 90 years.8 Surgical destruction of LOS by cardiomyomectomy (excision of LOS) with9 ,10 or without11 ,12forming a hiatus hernia, by cardiomyotomy,9 ,13 ,14 by cardioplasty in which a full thickness longitudinal incision is made through the sphincter and the defect repaired with transverse closure,9 ,15-18 or by hydrostatic balloon inflation,10 have all been used to create pathological reflux in animal models. Other surgical models include the creation of a hiatus hernia with or without vagotomy19-22 and the formation of a gastrostomy.23 The placement of a gastric fistula8 or gastrostomy13 ,18 has also been used to increase intragastric pressure in order to produce reflux experimentally.
Reflux has also been experimentally induced by pharmacological means in animal models with continuous infusion of atropine24 and intravenous pentagastrin.12 A simple model of oesophagitis, produced by the instillation of chemicals including hydrochloric acid and bile,25-28 which have been implicated in the pathogenesis of reflux oesophagitis29has been used in some studies.
Some investigators have used oesophagitis as an indicator of reflux,9-12 15-19 while others measured distal oesophageal pH with or without abdominal compression (Tuttle test).23 ,24 LOS pressure measurements,2 ,16yield pressure,2 ,13 ,30 or the volume of coloured intragastric fluid that produced endoscopically identifiable GOR13 ,18 have also been used as indirect measurements or indicators of reflux. Some studies used radiology to observe reflux10 ,16 and to delineate the angle of His which was used as a measure of the sphincter competence.13
Although some investigators have measured oesophageal acid exposure in the short term, while under anaesthesia in pigs23 and dogs,24 it has proved difficult to perform long term studies of acid reflux, especially in a conscious ambulant animal model. Samelson and colleagues12 and Patrikios and colleagues31 were able to obtain measurements of distal oesophageal acid exposure up to four hours through a surgically created cervical oesophagostomy in conscious dogs. Gillenet al managed to measure intraoesophageal pH in unanaesthetised dogs up to four hours using pH catheters.17 The use of radiotelemetry capsules sewn to the oesophageal wall has for the first time allowed long term, repeatable measurements of 24 hour acid exposure or longer in conscious, ambulant animals.32 ,33
The observation that apparently healthy pigs had acid reflux at values which would be pathological in man came as a surprise. It thus allowed us to use the pig as a model of GOR without requiring any prior surgical disruption of the LOS, as had been originally planned. The significance of this level of reflux in the pig is uncertain and is probably physiologically normal for this animal as there was no endoscopic or histological evidence of oesophagitis. Studies by Patrikios and colleagues31 and Samelson and colleagues12 in mongrel dogs indicated that the mean distal oesophageal acid exposure (percentage time pH was less than 4) in these animals was 0.6% and 3.1%, respectively, over a period of four hours. In support of our observations of reflux in pigs is a study by Heig et al using pH catheters under anaesthesia which reported that piglets have short episodes of spontaneous GOR.23 There are no other published studies of ambulatory 24 hour pH monitoring in animal models by groups other than our own. Our studies in beagle dogs have revealed that the normal 24 hour pH profile of distal oesophageal acid exposure (median percentage time pH less than 4–2.1)32 ,33 is similar to that seen in healthy humans.34
The anatomy of the pig cardio-oesophageal junction is different to that seen in dog and man in two respects. There is a subdiaphragmatic diverticulum in the pig’s fundus and the squamocolumnar mucosal junction features prominent nodular papillae. Our manometric measurements suggest that the median LOS pressure in pigs (3 mm Hg) and in beagle dogs (4.6 mm Hg)2 is lower than that reported in healthy human volunteers (14.9 mm Hg).35 The manometric measurements in dog and pig were made under anaesthesia but there are few comparable manometric measurements under anaesthesia in patients. One study by Hill in 200 patients compared intraoperative manometric measurements, before and after median arcuate posterior gastropexy carried out under anaesthesia with preoperative and postoperative measurements performed without anaesthesia; good correlation was shown between these measurements (5.5 versus 5.0 and 21.8 versus 19.0 mm Hg, preoperative versus intraoperative before repair and pullout versus postoperative).36 Another study by Jamieson and Myers in 34 patients undergoing fundoplication gave similar results when comparing preoperative measurements performed before and during anaesthesia (12 versus 12 mm Hg).37 The pig, unlike man, is never upright which may make reflux more likely to occur. It is probable that this level of reflux is normal for the pig and that the mucosal defence mechanisms are superior, thus decreasing the likelihood of oesophagitis.
The demonstration of acid reflux at this level seems to be a real phenomenon. The anaesthesia did not cause the reflux as it was consistently present up to two weeks after insertion of the radiotelemetry capsule in ambulant animals. Furthermore, the postoperative improvement of the pH could not be explained by the growth of the pigs. In two animals the operation was postponed for a week to check for spontaneous improvement in distal acid exposure, but no improvement was observed. It is possible but unlikely that the radiotelemetric capsule might serve as an irritant or bolus; this might induce subtle lower oesophageal sphincter relaxations which were then corrected by endoscopic gastroplasty. Against this are the following observations. We have sewn radiotelemetry capsules in canine oesophagus under the same conditions. These dogs did not have reflux on 24 hour pH studies on any occasion.32 ,33 We recorded some reflux episodes during the anaesthetic period but at endoscopy never observed any tendency for the radiotelemetry capsules to prolapse into the stomach corresponding to the observed reflux episodes. Manometric and pH measurements showed that the improvement occurred immediately after endoscopic gastroplasty and did not change during the observation period.
The continuous transmission of pH from the oesophagus for a period of up to a week represents the longest continuous recording of distal oesophageal pH achieved to date. Radiotelemetry capsules can provide much longer continuous transmission of pH data. The longest continuous transmission of pH data from a radiotelemetry capsule sewn with an endoscopic sewing machine to the human stomach lasted 159 days.38
The animal model described in this study has certain advantages. Prior surgery is not required to induce reflux. The methods used in the study in preparation of the model are non-invasive and therefore less likely to cause pain. Long term measurements allow studies of the effect of surgery on pH rather than indirect pressure measurements. The animals are conscious, ambulant and not restrained. Possible disadvantages of the model include the occasional detachment of the radiotelemetry capsule from the oesophagus and displacement of the aerial belt.
The results in this study show that endoscopic gastroplasty significantly reduced distal oesophageal acid exposure in the short term. There was also reduction in the number of reflux episodes following the procedure. Sphincter pressure and length were shown to be significantly increased after the operation. Long term studies are required to assess the effectiveness, safety, and longevity of endoscopic gastroplasty. Preliminary studies in man suggest that symptomatic improvement, as well as alteration in pH and pressure, can be achieved with endoscopic gastroplasty.39
Acknowledgments
Patents on endoscopic sewing machines, knot tying, and thread cutting devices are held by our group. This work was supported by a Science and Engineering Research Council grant (GR IG 11675) and the Wellcome Trust (No. 042997/2/94/A). Some of this data was presented at the British Society of Gastroenterology and was published in abstract form (Kadirkamanathan SS, Yazaki E, Hepworth CC, et al. Reflux control at flexible endoscopy using endoluminal suturing in an “in-vivo” model. Gut1995;37:A52).
Abbreviations
- GOR
- gastro-oesophageal reflux
- GORD
- gastro-oesophageal reflux disease
- LOS
- lower oesophageal sphincter