Article Text

Abstract
BACKGROUND/AIMS Intestinal metaplasia (IM) is a common finding at the oesophagogastric junction, but the aetiopathogenesis of the different IM subtypes—that is, incomplete IM (specialised columnar epithelium, SCE) and complete IM— and their associations with gastro-oesophageal reflux disease and Helicobacter pylori gastritis are unclear.
METHODS 1058 consecutive dyspeptic patients undergoing gastroscopy were enrolled. The gastric, oesophagogastric junctional, and oesophageal biopsy specimens obtained were stained with haematoxylin and eosin, alcian blue (pH 2.5)-periodic acid Schiff, and modified Giemsa.
RESULTS Complete junctional IM was detected in 196 (19%) of the 1058 subjects, and in 134 (13%) was the sole IM subtype. Incomplete junctional IM (SCE) was detected in 101 (10%) subjects, of whom 62 (61%) also had the complete IM subtype. Of patients with normal gastric histology (n = 426), 6% had complete IM and 7% junctional SCE. The prevalence of both types of IM increased with age in patients with either normal gastric histology or chronic gastritis (n = 611). Epithelial dysplasia was not detected in any patients with junctional IM. In multivariate analysis, independent risk factors for incomplete junctional IM were age (odds ratio (OR) 1.3 per decade, 95% confidence interval (CI) 1.2 to 1.6), endoscopic erosive oesophagitis (OR 1.9, 95% CI 1.1 to 3.2), and chronic cardia inflammation (OR 2.9, 95% CI 1.3 to 6.2), but not gastric H pylori infection (OR 1.0, 95% CI 0.6 to 1.7). In univariate analysis, junctional incomplete IM was not associated with cardia H pylori infection. Independent risk factors for “pure” complete junctional IM (n = 134) were age (OR 1.2 per decade, 95% CI 1.0 to 1.4), antral predominant non-atrophic gastritis (OR 2.6, 95% CI 1.3 to 5.2), antral predominant atrophic gastritis (OR 2.1, 95% CI 1.1 to 5.2), and multifocal atrophic gastritis (OR 7.1, 95% CI 2.5 to 19.8). In univariate analysis, junctional complete IM was strongly associated with chronic cardia inflammation and cardia H pylori infection (p<0.001).
CONCLUSIONS Both complete and incomplete junctional IM are independent acquired lesions that increase in prevalence with age. Although IM subtypes often occur simultaneously, they show remarkable differences in their associations with gastritis and erosive oesophagitis: junctional complete IM is a manifestation of multifocal atrophic gastritis, while the incomplete form (SCE) may result from carditis and gastro-oesophageal reflux disease. The frequency of dysplasia in intestinal metaplasia at the oesophagogastric junction appears to be low.
- intestinal metaplasia
- oesophagogastric junction
- oesophagitis
- gastritis
- gastro-oesophageal reflux disease
- Helicobacter pylori
Abbreviations used in this paper
- IM
- intestinal metaplasia
- SCE
- specialised columnar epithelium
Statistics from Altmetric.com
- intestinal metaplasia
- oesophagogastric junction
- oesophagitis
- gastritis
- gastro-oesophageal reflux disease
- Helicobacter pylori
Intestinal metaplasia (IM) is commonly detected in random biopsy specimens taken immediately distal to the normally located squamocolumnar junction.1-6 IM at the oesophagogastric junction is a topic of great interest, because it may aetiopathogenetically be linked to the adenocarcinoma at this location.7 The incidence of this carcinoma has increased at a rate exceeding that of any other cancer.8 Whether IM at the oesophagogastric junction is a consequence of gastro-oesophageal reflux disease or a manifestation of multifocal gastritis caused byHelicobacter pylori is unclear.
IM is histopathologically divided into three subgroups based on the mucin content of the columnar-type and goblet cells.9 ,10In the complete form of IM (type I), the columnar cells are absorptive and contain neutral mucins, whereas in the incomplete forms of IM, they are at least partly secretory and contain acidic sialomucins (type II) or sulphomucins (type III).10 ,11 IM types II and III are commonly referred to as incomplete IM or specialised columnar epithelium (SCE) and are easily recognised with simple histochemical stains such as alcian blue (pH 2.5)-periodic acid Schiff.12 SCE is the histological hallmark of Barrett’s oesophagus.12
This study set out to examine the prevalences and demographics of complete IM and SCE at the oesophagogastric junction in a large consecutive series of dyspeptic patients sent for open access gastroscopy. We wanted to evaluate the associations between these IM subtypes and gastritis, H pylori infection, and endoscopic and histological signs of gastro-oesophageal reflux disease, as well as the extent to which junctional complete IM and SCE are similar or dissimilar in these associations.
Methods
PATIENTS
The study population totalled 1698 consecutive dyspeptic patients sent for gastroscopy over a four month period. The patients with classical Barrett’s oesophagus—that is, SCE detected above the oesophagogastric junction (n = 28)—were excluded. Patients for whom no adequate gastric antral, corpus, and oesophagogastric junctional biopsy specimens were available were also excluded, leaving a final study population of 1058 patients.
ENDOSCOPY
Two biopsy specimens were obtained from the gastric antrum 2 cm or more from the pylorus, and two others from the large curve of the gastric body, the oesophagogastric junction, and the distal oesophagus 2 cm or more above the junction (eight samples in all).
The oesophagogastric junctional biopsy specimens were obtained by first identifying the junction between the oesophagus and stomach at the level of the proximal end of the gastric folds.13 ,14 The normal squamocolumnar mucosal junction, or Z line, is coincident with the aforementioned junction.14 In this report, junctional IM denotes the IM detected in biopsy specimens obtained immediately distal to normal appearing Z line. Junctional biopsy specimens were obtained under direct vision with the gastroscope in antegrade position. If gastric type mucosa extended circumferentially or as tongues above the oesophagogastric junction, biopsy specimens were taken separately from this mucosa to detect Barrett’s oesophagus. Subjects with Barrett’s oesophagus or incomplete IM detected in the oesophagus were excluded from the present analysis.
Subjects with endoscopic oesophagitis grades II-IV by Savary-Miller classification15 were classified as having erosive oesophagitis.
HISTOLOGY
Formalin fixed biopsy samples were embedded in paraffin wax, and tissue sections stained with haematoxylin-eosin, alcian blue (pH 2.5)-periodic acid Schiff, and modified Giemsa. The presence of gastritis, activity of gastritis, gastric gland atrophy, IM, andH pylori infection were classified according to the Sydney System.16 Chronic gastritis subtypes were classified as follows: 1, normal gastric histology; 2, antral predominant gastritis (inflammation or inflammatory activity more severe in the gastric antrum than in the corpus, but no gastric gland atrophy); 3, antral predominant atrophic gastritis (gastric gland atrophy detected in the antrum but not the corpus); 4, corpus predominant gastritis (gastric gland atrophy detected only in the corpus or non-atrophic gastritis with more severe inflammation or inflammatory activity in the corpus); 5, multifocal atrophic gastritis (gastritis with atrophy detected in both the antrum and corpus).
The presence of complete and/or incomplete IM, chronic inflammation, and H pylori infection in the cardia was evaluated in junctional biopsy specimens. Only cases showing typical mucus secreting glandular gastric cardia epithelium17 were included in this study. Chronic cardia inflammation was defined as infiltration of the lamina propria by lymphocytes and plasma cells.18 Complete IM was defined as the presence of goblet cells without acidic alcian blue (pH 2.5)-periodic acid Schiff positive material in columnar-type cells.19 Incomplete IM or SCE was defined as the presence of goblet cells, with acidic mucins in goblet and adjacent columnar-appearing cells.19 ,20 Figure1 shows examples of complete and incomplete forms of metaplasia. Dysplasia, when present and definite, was graded as low grade or high grade.12 The study population was divided into three groups according to the histological findings at the oesophagogastric junction: group 1, patients with only complete type junctional IM; group 2, patients with SCE or incomplete junctional IM (61% of them also had complete IM); group 3, control subjects without either type of IM.

Complete intestinal metaplasia (IM) is characterised by goblet cells stained red or blue by alcian blue (pH 2.5)-periodic acid Schiff stain and by the presence of absorptive non-goblet cells (A). Incomplete IM or specialised columnar epithelium is differentiated from the complete IM subtype by the presence of goblet cells intermixed with mucin-secreting columnar-appearing non-goblet cells staining red and blue by the alcian blue (pH 2.5)-periodic acid Schiff stain (B).
Microscopic oesophagitis was defined as papillae extending into the upper third of the oesophageal mucosa with or without the infiltration of inflammatory cells.8
STATISTICAL ANALYSIS
χ2 and Mann-Whitney U tests were used to compare groups, and p<0.05 was considered as significant. Multiple logistic regression analysis was used to assess the relations between complete or incomplete IM and factors with a significant difference in prevalence in univariate analysis when the two groups were compared with the control group without these lesions. Odds ratios (OR) with their 95% confidence intervals (95% CI) are reported for independent risk factors for the complete and incomplete IM forms.
ETHICS
This study was approved by the ethics committee of Jyväskylä Central Hospital.
Results
The study population consisted of 1058 patients (mean age 57.3 years, 95% CI 56.3 to 58.3 and male to female ratio 1:1.5), of whom 134 (13%) had complete IM and 39 (4%) incomplete IM (SCE) as the sole type of IM at the oesophagogastric junction. The mean age of the “pure” complete IM group was 65.0 (95% CI 62.5 to 67.4) years and that of the “pure” incomplete IM group 62.9 (95% CI 58.5 to 67.3) years. A total of 62 patients harboured both types of IM simultaneously, giving overall prevalence for complete IM of 19% (n = 196), and for incomplete IM or SCE of 10% (n = 101). Henceforth patients with complete IM denotes the patients with this type of IM only (n = 134), whereas the incomplete IM or SCE group refers to patients with SCE only plus those with complete IM as well as SCE (n = 101).
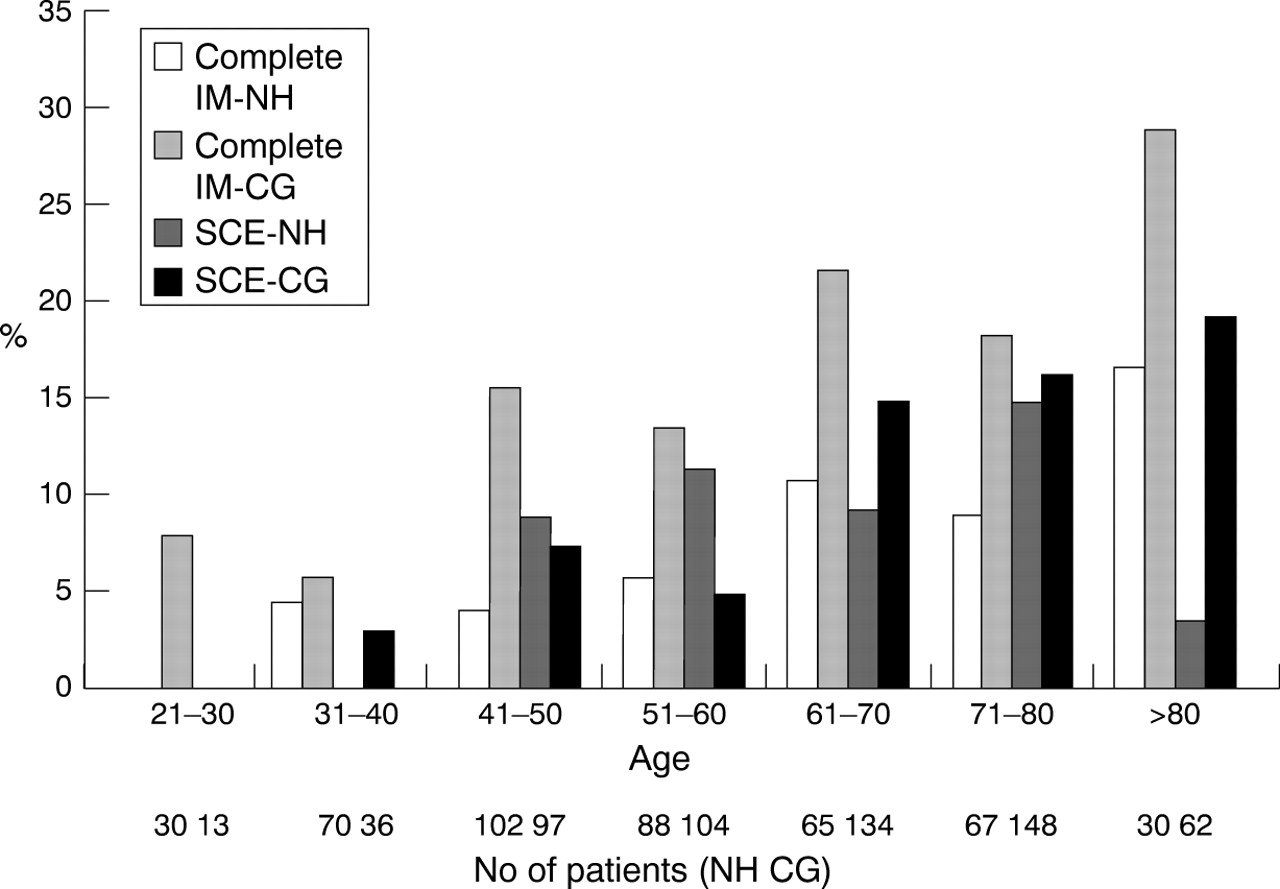
The patients with complete or incomplete IM were older than those without either lesion (table 1, both patients with chronic gastritis and normal stomach included). In subjects with normal stomach, the mean age of the non-IM-non-SCE group was 50.8 (95% CI 48.4 to 53.2) years, that of the junctional complete IM group 62.4 (95% CI 56.3 to 68.5) years, (p = 0.001), and that of the junctional SCE group 54.0 (95% CI 46.3 to 61.7) years (p = 0.003). The difference in mean age between the complete IM and SCE group was insignificant (p = 0.1). Both types of junctional IM correlated with age in patients with normal gastric histology or with chronic gastritis (fig 2). The sex ratios of patients with either type of junctional IM were not significantly different from that of the control group. In patients with multifocal atrophic gastritis, complete junctional IM was significantly more common than incomplete junctional IM (table 2). On the other hand, in patients with histologically normal stomach, junctional incomplete IM was more common than complete IM, although the difference did not reach statistical significance (table 2). Junctional epithelial dysplasia was not observed in any patient with complete or incomplete junctional IM.
Demographic, endoscopic, and histological characteristics of patients with junctional complete or incomplete intestinal metaplasia (IM) compared with those of the control group without these lesions

{kind=link}
{kind=link}
Prevalences of junctional complete and incomplete (specialised columnar epithelium, SCE) intestinal metaplasia (IM) in different age groups. NH, normal gastric histology (n = 426); CG, chronic gastritis (n = 632). The correlation of age with both IM types was significant in the CG (p<0.001 for complete IM and incomplete IM) and NH (p = 0.001 for complete IM and p = 0.002 for incomplete IM) group.
The prevalences of oesophagogastric junctional complete and incomplete intestinal metaplasia (IM) in different types of gastritis
Reflux symptoms, smoking habits, or the use of non-steroidal anti-inflammatory drugs did not correlate with the presence of either type of IM (table 1). Hiatal hernia or histological oesophagitis did not predict the presence of junctional IM of either type.
Multivariate analysis showed that age, antral predominant non-atrophic gastritis, antral predominant atrophic, and multifocal atrophic gastritis were independent risk factors for “pure” complete junctional IM (table 3). Independent risk factors for junctional SCE were age, endoscopic erosive oesophagitis, and chronic cardia inflammation (“carditis”) (table 3).
Results of multivariate analyses to determine the independent risk factors for junctional complete and incomplete intestinal metaplasia
Discussion
This study showed complete and incomplete IM to be common findings at the oesophagogastric junction in a consecutive series of dyspeptic patients: almost a quarter of our study population had either or both forms of the lesion. Previously reported prevalence rates varied from 5.3 to 36%.2-4 ,6 ,21 ,22 The width of this range may be due to patient selection or to different methods of biopsy sampling or staining for histology. Haematoxylin-eosin stain yields lower IM rates than the simultaneous application of alcian blue(pH 2.5)-periodic acid Schiff, which also enables differentiation between complete and incomplete IM.6 ,19 ,20 ,23
The prevalence of junctional complete IM and SCE at the oesophagogastric junction increased with age, and both IM subtypes were also found in patients without concomitant gastritis, indicating that junctional IM and SCE are acquired local lesions. Complete IM and SCE seemed to occur in men and women at similar frequencies, contrasting with Barrett’s oesophagus and oesophagogastric junctional adenocarcinomas which are strongly male predominant diseases.12 ,24 ,25
An important finding was that, in multivariate analysis, endoscopic erosive oesophagitis, but not H pyloriinfection or antral predominant gastritis, was an independent risk factor for junctional SCE. In contrast, complete junctional IM was associated with gastritis, and particularly with multifocal atrophic gastritis, but not with endoscopic erosive oesophagitis. These observations suggest that at least some subjects with junctional SCE suffer this lesion as a consequence of gastro-oesophageal reflux disease, while complete junctional IM is a manifestation of multifocal atrophic gastritis and H pylori infection. However, in patients with normal stomach, complete junctional IM may result from gastro-oesophageal reflux disease, because this IM subtype was detected in 6% of this subgroup.
In the stomach, IM represents a sequence of progressive lesions from complete (type I or “small bowel type IM”) to incomplete (types II and III or “colonic type IM”) IM.26 ,27 This may also be the case with IM at the oesophagogastric junction. However, this hypothesis was not supported by the finding that junctional complete IM and SCE were detected at a similar age in subjects with normal gastric histology. Proper and correct analysis of the background factors for junctional IM subtypes is difficult because obviously there are varying degrees of overlap with regard to the pathogenic factors for junctional complete IM and SCE.
The present findings suggest important clinical and practical conclusions on junctional SCE: the presence of SCE at the oesophagogastric junction in subjects with a normal stomach—that is, histologically normal antral and gastric corpus mucosa—may predict gastro-oesophageal reflux disease with high certainty. This could also apply to junctional SCE patients with chronic gastritis. The presence of complete junctional IM may not indicate reflux, but is a manifestation of multifocal atrophic gastritis. These conclusions are concordant with an earlier study indicating that junctional SCE is related to gastro-oesophageal reflux disease detected by 24 hour oesophageal pH monitoring.28
In this study, none of the patients with junctional IM showed dysplasia, which accords with an earlier report.5Dysplasia is quite a common finding at Barrett’s epithelium and precedes the appearance of adenocarcinoma.12 This may also be the case in the adenocarcinomas of the oesophagogastric junction, which are on the increase in many western countries.24 ,25 ,29 The low rate of dysplasias in junctional IM suggests that neither junctional SCE nor complete IM are as high risk carcinoma precursor lesions as Barrett’s oesophagus is for oesophageal adenocarcinoma. On the other hand, junctional complete IM and SCE are common lesions, and the absence of dysplasia in a limited number of patients does not exclude the possibility that junctional SCE or complete IM could progress to dysplasia and carcinoma in some patients.
In conclusion, this study indicates that complete and incomplete IM at the oesophagogastric junction are common acquired lesions. They may not be directly related to Barrett’s oesophagus or junctional adenocarcinomas because of the differences in their basic demographics. It seems that incomplete junctional IM (SCE) and complete IM are dissimilar lesions in terms of their pathogenesis: the former seems to be a consequence of gastro-oesophageal reflux disease and the latter a manifestation of multifocal atrophic gastritis.
Acknowledgments
In addition to the authors, the following doctors are members of The Central Finland Endoscopy Study Group: Liisa Ahlskog-Muraja, Teuvo Antikainen, Sirpa Antila, Jorma Anttinen, Matti Hallikas, Kari-Pekka Hämäläinen, Heikki Janhonen, Matti Kairaluoma, Kerkko Karjalainen, Pekka Kauranen, Matti Kolu, Heikki Korhonen, Jari Korhonen, Ritva Koskela, Raimo Krees, Ilkka Kunnamo, Vesa Kärjä, Päivi Laaksonen, Matti Laukkanen, Reino Liisanantti, Marja Lohman, Timo Mäntynen, Kyösti Nuorva, Antero Palmu, Ulla Palmu, Matti Pellinen, Pertti Särkkä, Harri Selänne, Tuula Tervo, Marianne Udd, Jukka Viinikka.
Abbreviations used in this paper
- IM
- intestinal metaplasia
- SCE
- specialised columnar epithelium