Article Text

Abstract
BACKGROUND Animal studies have shown that the neuromuscular structures on the luminal side of the colonic circular muscle coordinate circular muscle activity. These structures have been identified by electron microscopy in the normal human colon, but have never been thoroughly studied in patients with acquired intestinal hypoganglionosis.
AIMS To perform histological, immunocytochemical, and electron microscopic examinations of the colon of a patient with acquired intestinal hypoganglionosis presenting as megacolon.
PATIENT A 32 year old man with a one year history of constipation and abdominal distention, a massively dilated ascending and transverse colon, and a normal calibre rectum and descending and sigmoid colon. He had a high titre of circulating serum anti-neuronal nuclear antibodies.
METHODS Histology, immunocytochemistry (for neurofilaments, neurone specific enolase, synaptophysin, glial fibrillar acidic protein, S100 protein, and smooth muscle α-actin), and electron microscopic examinations on the resected colon.
RESULTS The number of ganglion cells and nerve trunks was decreased throughout the colon. Disruption of the neural network and a loss of interstitial cells of Cajal were observed on the luminal side of the circular muscle; in their place, the non-dilated colon contained a hypertrophic fibromuscular layer.
CONCLUSIONS Striking architectural alterations occurred at the site regarded as the source of the coordination of colonic circular muscle activity in an adult patient with acquired intestinal hypoganglionosis presenting as megacolon.
- megacolon
- intestine
- hypoganglionosis
- pseudo-obstruction
- interstitial cells of Cajal
Abbreviations used in this paper
- ICCs
- interstitial cells of Cajal
- ANNA-1
- anti-neuronal nuclear antibodies
Statistics from Altmetric.com
Acquired intestinal aganglionosis is a rare condition that may present with intestinal pseudo-obstruction and colonic dilatation.1 In the normal human colon, electron microscopy has disclosed a particular organisation of the structures on the luminal side of the circular muscle, where two to eight rows of smooth muscle cells with unusual morphology have been identified; close to these cells, a fibrous layer containing a network of neural elements and interstitial cells of Cajal (ICCs) has been described.2 Animal studies have shown that this region generates slow waves3 and coordinates their progression along the circular muscle,4 but the architectural organisation of these structures has not yet been thoroughly investigated in patients with acquired intestinal hypoganglionosis. We performed histological, immunocytochemical, and electron microscopic examinations of the colon of an adult patient with acquired intestinal hypoganglionosis presenting as megacolon.
Case report
A 32 year old white man was referred to our unit in January 1996 with a one year history of constipation and abdominal distention. At the time of the onset of the symptoms, he was admitted to another hospital where a barium enema and computed tomography of the abdomen disclosed a massively dilated ascending and transverse colon, with a normal calibre rectum and descending and sigmoid colon. No obstructing lesion was identified at colonoscopy.
At the time of our physical examination, the patient was 171 cm tall, weighed 58 kg, and had a distended abdomen. The results of a neurological examination were normal, and there was nothing to suggest an autonomic neuropathy. Routine laboratory investigations showed nothing worthy of note, but a plain abdominal radiograph disclosed considerable dilatation of the ascending and transverse colon; the rectum was empty. The results of barium follow through radiography of the small intestine were normal. Anorectal and oesophageal manometry were performed as previously described5: the resting pressure of the anal sphincter was normal (56 mm Hg), but there was no rectoanal inhibitory reflex. Oesophageal peristalsis was replaced by low amplitude multiple peaked simultaneous contractions (the mean distal oesophageal amplitude was 35 mm Hg). The resting pressure of the lower oesophageal sphincter was 25 mm Hg, and the sphincter relaxed normally after swallows. An intrinsic neuropathy not limited to the colon and rectum was suspected and the patient was treated with a low fibre diet, prokinetics, oral laxatives, and enemas. Three months later, he underwent colectomy with ileostomy for an impacted colon.
After surgery, the patient gained 6 kg but all of the small intestine became dilated despite the absence of any mechanical obstruction. Episodes of pseudo-obstruction occurred and total parenteral nutrition was started. Anti-neuronal nuclear antibodies (ANNA-1) were measured in the serum by indirect immunofluorescence on cryostatic sections of mouse brain and immunoblots on human Purkinje cell homogenates1 ,6; the latter showed a high titre of ANNA-1 (1/6400). No evidence of neoplasia was observed during the 40 months of follow up.
Methods
The colon was examined immediately after surgery, with seven pieces of tissue being cut from the caecocolonic junction, the ascending, cranial, and caudal transverse, the cranial and caudal descending, and the sigmoid colon. Full thickness longitudinal and transverse samples for light microscopy were taken from each piece of tissue, fixed in buffered formalin overnight, dehydrated, and embedded in paraffin. Serial 4 μm thick sections were cut, with the first and last being stained with haematoxylin and eosin, and the others being preserved for immunocytochemistry. The control tissues were surgical specimens obtained from ten men with a mean age of 50 years (range 45–60) who underwent colectomy for colonic cancer; these patients had no other colonic disease and the samples were taken at least 10 cm from the neoplastic area.
The neural and glial structures were immunostained with monoclonal antibodies or anti- sera raised against neurofilaments (2F11, IgG1, kappa; Dako, Glostrup, Denmark), γ-γ neurone specific enolase (BBS/NC/VIH14, IgG1, kappa; Dako), synaptophysin (SY38, IgG1, kappa; Dako), glial fibrillary acidic protein, and S100 protein (Dako); the muscular structures were immunostained with a monoclonal antibody raised against smooth muscle α-actin (1A4, IgG2a, kappa; Dako). T lymphocytes were marked by specific anti-CD3 antiserum (Dako), and B lymphocytes by an anti-CD20 monoclonal antibody (L26; IgG 2a, kappa; Dako). Immunoreactivity was detected using the standard immunoperoxidase/diaminobenzidine method and assessed on a numerical scale (0 = absent, 1 = focal, 2 = multifocal, 3 = diffuse).
c-kit immunoreactivity was also tentatively assessed using the c-kit Ab-1 antibody (Oncogene Research Products, Calbiochem, Milan, Italy) as described by Hagger et al 7; c-kit immunoreactivity was virtually absent in the patient but, under our experimental conditions, was also very weak and irregular in the controls. The results were therefore judged to be non-specific and were disregarded, also given the limitations of c-kit immunoreactivity in detecting ICCs.8
The samples for electron microscopy were taken from sites adjacent to those of the samples obtained for light microscopy, and processed to obtain both transverse and longitudinal sections as previously described.2 Semithin sections were stained with a toluidine blue solution and photographed under a light microscope; ultrathin sections of the selected areas were stained, and further examined and photographed under a JEOL 1010 electron microscope.
Results
The ascending, transverse, and descending sigmoid colon (measured while both ends of the specimen were still clamped) were respectively 12, 17, and 6 cm wide. Haematoxylin and eosin staining disclosed no more than two ganglion cells per cm in both the myenteric and submucous plexuses throughout the colon (the mean values in the controls were 25 (15–35) and 35 (7–63) cells per cm respectively). A scanty lymphocyte infiltrate consisting mainly of CD3 positive T lymphocytes was observed in association with the remaining neural structures in only one of the sections. The reduced number of ganglion cells throughout the colon was confirmed by immunocytochemistry (table 1) and electron microscopy. Most of the remaining nerve endings had a large diameter, and contained few synaptic vesicles but abnormally abundant tubules of smooth endoplasmic reticulum and neurofilaments. There were very few glial and Schwann cells in the muscular layers and submucosa (table 1).
Immunoreactivity of neural, glial, and muscular structures in the patient and in 10 controls (mean values in parentheses)
The mean thickness of the circular muscle layer was 820 (400–1500) μm in the dilated and 1460 (800–1800) μm in the non-dilated colon; the longitudinal muscle layer was 300 (200–500) μm and 820 (400–1600) μm thick. The thickness of the control circular and longitudinal muscles was 690 (400–1000) μm and 362 (200–600) μm. Cells resembling fibroblasts and myofibroblasts were observed in the circular muscle layer. Immunostaining for smooth muscle α-actin was diffuse in both the circular and longitudinal muscle layers (table 1), but less intense in the patient than in the controls.
Immunocytochemistry (table 1) and electron microscopy showed the absence of nerve structures and ICCs on the luminal side of the circular muscle throughout the colon. A thick fibrous layer with haphazardly organised elastic and collagen fibres, interspersed with cells that were mainly parallel to the major axis of the gut, was observed only in the non-dilated colon (fig 1A); this layer also contained smooth muscle α-actin immunoreactive cells (fig 1B; table1), some of which were myofibroblasts, and smooth muscle cells (fig1C). All of them had an extended rough endoplasmic reticulum and a large Golgi apparatus, and were interconnected by the simple apposition of their plasma membranes or by specialisations similar to those of the smooth muscle cells of the inner portion of the circular muscle. Macrophages were common, but none of them showed phagocytic activation; no degenerating cells were ever observed.

Hypertrophic fibromuscular layer of the non-dilated descending colon. (A) Muscularis propria and submucosa. Semithin section stained with toluidine blue. S, serosa; LL, longitudinal muscle layer; CL, circular muscle layer; SM, submucosa. A thick fibromuscular layer (asterisk) is located on the luminal side of the circular muscle (original magnification × 70). Calibration bar 140 μm. (B) Smooth muscle α-actin immunoreactivity in the fibromuscular layer showing that some of the cells (arrows) are smooth muscle cells (original magnification × 500). Calibration bar 6.5 μm. (C) Some of the cells of the fibromuscular layer had the features of myofibroblasts (asterisks), and others the features of smooth muscle cells (MC): note the extended rough endoplasmic reticulum and large Golgi apparatus in the cells identified as myofibroblasts, and the well developed contractile apparatus in those identified as smooth muscle cells (original magnification × 6500). Calibration bar 1.5 μm.
ICCs were present in the region between the circular and longitudinal muscle layers and located near the residual nerve elements of the myenteric plexus (fig 2A,B); they had few organelles, and were closely associated with elastic and collagen fibres (fig2C).

{kind=link}
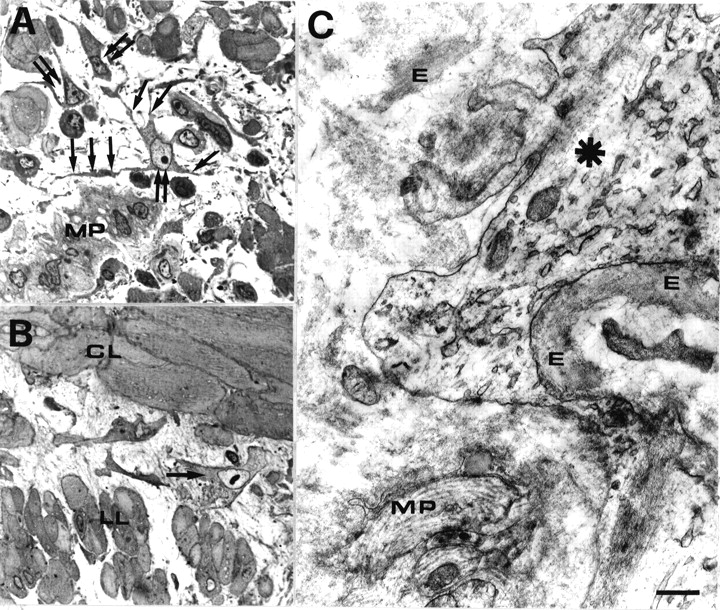{kind=link}
Interstitial cells of Cajal (ICCs) in the myenteric plexus region. (A) Dilated (right transverse) colon. Semithin section stained with toluidine blue. Three ICCs (double arrows) with several branches (arrows) are located near myenteric plexus elements (MP) (original magnification × 750). Calibration bar 13 μm. (B) Non-dilated (descending) colon. Semithin section stained with toluidine blue. One ramified ICC (arrow) with clear cytoplasm is located between the circular (CL) and longitudinal (LL) muscle layers (original magnification × 750). Calibration bar 13 μm. (C) Non-dilated descending colon. Electron microscopy showed that the ICC cytoplasm (asterisk) appeared to be poor in mitochondria, filaments, and caveolae. E, elastic fibres; MP, myenteric plexus elements (original magnification × 25 000). Calibration bar 0.4 μm.
Discussion
This paper describes an adult patient with acquired intestinal hypoganglionosis presenting as megacolon. Megacolon in adults is a rare condition associated with various clinical disorders, such as idiopathic megacolon, Hirschsprung’s disease, and intestinal pseudo-obstruction.9 In most cases of idiopathic megacolon, enteric innervation is normal10; in patients with Hirschsprung’s disease, there are no ganglion cells, and the nerve fibres are hypertrophic in the narrowed segment of the colon. Generalised myopathy or neuropathy may be associated with megacolon in patients presenting with intestinal pseudo-obstruction.9In our patient, the onset of the disease in adult life, the extension of the hypoganglionosis to the dilated segment of the colon, the absence of nerve trunk hypertrophy and the presence of circulating ANNA-1 support the diagnosis of acquired intestinal hypoganglionosis. Moreover, the abnormally large number of neurofilaments and smooth endoplasmic reticulum tubules in the remaining neural structures suggested a previous degenerative injury of the enteric nervous system.11 As previously described in patients with aganglionosis,1 the inflammatory infiltrate around the residual neural structures of the enteric nervous system mainly consisted of T lymphocytes, supporting the hypothesis that a T cell mediated response may precede the ANNA-1 response in the process leading to enteric nerve destruction.1
The circular and longitudinal muscle layers were thickened, particularly in the non-dilated colon, and electron microscopy disclosed features suggesting both muscular hypertrophy and hyperplasia. Similar findings have been previously reported in the lower oesophageal sphincter of patients with achalasia,12suggesting that denervation may stimulate a hypertrophic muscle response.
The neural network on the luminal side of the circular muscle was disrupted and devoid of ICCs throughout the colon, whereas a few ICCs were still present near the residual neural structures of the myenteric plexus. It has been proposed that ICCs may be pacemakers of gut motility and also act as intermediaries of the neural control of gut muscular activity.13 A lack of ICCs has been reported in the aganglionic segment of children with Hirschsprung’s disease,14 but our study is the first to describe the absence of ICCs in an adult patient with intestinal hypoganglionosis, and suggests that disruption of the ICC network may be a common feature of both congenital and acquired hypoganglionosis.
A thick fibromuscular layer was found on the luminal side of the circular muscle in the non-dilated colon. Ultrastructural examination identified the cell types of this layer as common fibroblasts in some cases and as partially or completely differentiated smooth muscle cells in most others. Torihashi et al 15 have shown that the development and maintenance of the specific ICC phenotype depends on c-kit signalling and that neurones release the natural ligand for c-kit. 15It can therefore be postulated that, in the absence of the neuronal c-kit signalling pathway, the pre-existing ICCs in our patient were transformed into smooth muscle cells, and the fibromuscular layer may represent structural remodelling in response to the disorganisation of the neural structures. Why the fibromuscular layer was present only in the descending and sigmoid non-dilated colon despite the more widespread neural impairment is difficult to explain, but it is reminiscent of the functional division of the colon into a cranial portion (the major site of storage) and a caudal portion (which acts mainly as a conduit). This division is associated with striking differences in smooth muscle anatomical organisation2 and mechanical properties, and muscle responsiveness to neuro-humoral agents and intracellular signalling pathways.
Acknowledgments
We are grateful to Dr E Contessini-Avesani who operated on the patient, Dr A di Troia and Dr E Nobile-Orazio for the determination of circulating anti-neuronal nuclear antibodies, and the Associazione Amici della Gastroenterologia del Padiglione Granelli and the University of Florence (grant ex quota 60%) for financial support.
Abbreviations used in this paper
- ICCs
- interstitial cells of Cajal
- ANNA-1
- anti-neuronal nuclear antibodies