Article Text

Abstract
BACKGROUND The renin-angiotensin system may be implicated in the subtle sodium handling abnormality in preascitic cirrhosis.
AIMS To assess the role of angiotensin II in sodium homoeostasis in preascitic cirrhosis, using losartan, its receptor antagonist.
PATIENTS Nine male, preascitic cirrhotic patients, and six age matched, healthy male controls.
METHODS A dose response study using 2.5, 5, 7.5, and 10 mg of losartan was performed on a daily 200 mmol sodium intake, followed by repeat studies with the optimal dose, 7.5 mg of losartan, to determine its effects on systemic and renal haemodynamics, renal sodium handling, and neurohumoral factors.
RESULTS Preascitic cirrhotic patients had significantly reduced baseline urinary sodium excretion compared with controls (154 (8) versus 191 (12) mmol/day, p<0.05), associated with significantly reduced systemic angiotensin II levels (6.0 (1.7) versus 39.5 (10.0) pmol/l, p=0.002). Losartan 7.5 mg normalised renal sodium handling in the preascitic cirrhotic patients (202 (12) mmol/day, p=0.05 versus baseline), without any change in systemic or renal haemodynamics, but with significantly increased systemic angiotensin II levels (7.8 (2.3) pmol/l, p=0.05 versus baseline). Losartan had no effect on renal sodium handling in controls.
CONCLUSIONS In preascitic cirrhotic patients, the subtle renal sodium retention, paradoxically associated with low systemic neurohumoral factor levels, is improved with low dose losartan, suggesting the involvement of angiotensin II via its direct action on the renal tubule.
- sodium retention
- preascitic cirrhosis
- renin-angiotensin-aldosterone system
- angiotensin II receptor antagonist
- renal haemodynamics
Statistics from Altmetric.com
- sodium retention
- preascitic cirrhosis
- renin-angiotensin-aldosterone system
- angiotensin II receptor antagonist
- renal haemodynamics
Abnormal sodium homoeostasis is a common complication of liver cirrhosis. A subtle sodium handling abnormality is found in the preascitic stage of cirrhosis,1 2 characterised by sodium balance while on a 100 mmol sodium per day diet,1 but positive sodium balance while on a 200 mmol sodium per day diet.2 This sodium handling abnormality becomes more severe as the patient's liver disease progresses until ascites finally develops. The presence of ascites and its complications, such as spontaneous bacterial peritonitis and hepatorenal syndrome, represent major indications for liver transplantation. Attention has therefore focused on elucidating the pathophysiology of this abnormal sodium handling and ascites formation, in order to attain better prognostic indicators and improved, less expensive therapeutic measures.
The sodium handling abnormality in preascitic cirrhotic patients has been shown to be due to sodium retention in the upright posture3 associated with increased serum levels of aldosterone.3 These observations suggest that the renin-angiotensin-aldosterone system (RAAS) may play a crucial pathogenetic role in the abnormal renal sodium handling in preascitic cirrhosis. The fact that abnormal sodium handling in cirrhosis has been localised predominantly to the proximal nephron,4 a site of angiotensin II action, supports this contention. The recent report, in preascitic cirrhotic patients, of a significant increase in intrarenal angiotensin II production with the application of lower body negative pressure which simulates an upright posture, associated with renal sodium retention,5 further strengthens the early role of the RAAS in the pathophysiology of abnormal sodium handling in cirrhosis. This sodium retention decreases on resumption of the supine posture, at the expense of the development of a hyperdynamic circulation.6 The associated suppression of systemic plasma renin activity (PRA), angiotensin II, and aldosterone concentrations to low normal levels indirectly indicates that the volume expansion consequent on sodium retention is still present in the supine posture. That is, the supine posture alone is insufficient to correct the sodium retention and volume expansion in cirrhosis.
Angiotensin II is a key regulator of sodium and fluid homoeostasis. Angiotensin II exerts its effects through binding to angiotensin II receptors. Specific intrarenal receptors of angiotensin II have been localised to the glomeruli, renal tubules, and renal vasculature.7-10 The development of specific competitive angiotensin II receptor antagonists has provided a tool with which the effects of angiotensin II can be studied.11 12 These angiotensin II receptor antagonists, unlike angiotensin converting enzyme (ACE) inhibitors, do not affect bradykinin metabolism, and are therefore less vasodepressive,13 making them a more attractive probe to assess angiotensin II action.
The aim of this study was to use losartan, an angiotensin II receptor antagonist, as a probe to assess the role of angiotensin II in the regulation of renal sodium handling and the mechanisms involved in preascitic cirrhosis, thus improving our understanding of the pathophysiology of ascites formation.
Materials and methods
Ethics approval for the study was granted by the Ethics Committee of The Toronto Hospital. All control subjects and cirrhotic patients gave informed consent for the study.
PATIENTS
Nine male, ascites free, biopsy proved cirrhotic patients, aged 57 (4) years (range 36–72), were recruited from the Liver Clinics of The Toronto Hospital. The aetiology of cirrhosis was either alcoholic (n=7), viral hepatitis C (n=1), or poststeatohepatitis (n=1). They were well compensated cirrhotic patients who had no history of ascites or diuretic use. Pugh score was 5.2 (0.2). Serum albumin was 35 (2) g/l, serum bilirubin 15 (2) μmol/l, and prothrombin time 11.4 (1.1) seconds. None of the patients had a history of ascites and absence of ascites was confirmed by ultrasound before enrolment. These patients were therefore termed preascitic cirrhotic patients. All patients were stable and had abstained from alcohol for at least six months prior to entry. Patients with intrinsic renal or cardiovascular disease on history and physical examination or with abnormal urinalysis, chestx ray, or electrocardiograph were excluded from the study, as were patients who had had an episode of gastrointestinal bleeding within the previous three months. Six age matched healthy male volunteers, aged 49 (4) years (range 36–62) and recruited through advertisement, served as controls. They were normotensive and non-obese, on no medication, and had been abstinent from alcohol for at least one month. None of the control subjects had evidence of liver or renal disease on history, physical examination, and urinalysis.
STUDY DESIGN
This strict metabolic study was conducted in the Clinical Investigation Unit of the Toronto Hospital. Both study groups had a run in period of one week during which time they were maintained on a 22 mmol sodium, 1 litre fluid per day diet to ensure that all study subjects started off the study at the same baseline sodium status.2 A 24 hour urine collection to measure urinary sodium excretion was obtained at the end of the first week in order to ensure compliance with the sodium washout. The study then began with the subjects placed on a 200 mmol sodium, 1.5 litre fluid per day diet for one week, as preascitic cirrhotic patients have been shown to reach a steady state of subtle sodium retention after being on a 200 mmol per day sodium intake for at least four days.2 Twenty four hour urine collections were made for the last three days of this week as an estimate of sodium handling. Daily weights were recorded throughout the study period.
Normal healthy individuals have been shown to block the vasoconstrictive response of angiotensin II with 10 mg of losartan14 and a natriuretic response was shown after 100 mg of losartan.15 However, an optimal dose of losartan for both vasodilatory and natriuretic effects in cirrhotic patients is not known. Therefore, a dose response study was first conducted with control subjects and cirrhotic patients receiving single sequential doses of 2.5, 5, 7.5, and 10 mg losartan at 8 00 am on different days, two days apart. The day the patient received 2.5 mg losartan was taken as day 1 of the study. On the day of medication, the patient was monitored with hourly blood pressure measurements for 12 hours, together with a 24 hour urine collection to determine urinary sodium excretion. The maximal hypotensive effect of losartan was expected to be approximately four to six hours after drug administration, although the pharmacological effect could last up to 24 hours.14Any patient who experienced a fall in mean arterial blood pressure of more than 10 mm Hg with a particular dose of losartan did not receive further doses of losartan and was observed for a further 24 hours from the time of maximal fall in mean blood pressure. The optimal dose of losartan was defined as the dose that produced improved sodium excretion (>20%) with minimal reduction in mean arterial pressure (<10 mm Hg)
After completion of the dose response study and with a rest period of two days, with control subjects and preascitic cirrhotic patients continuing with their sodium intake of 200 mmol and 1.5 litre fluid per day, in order to maintain the sodium retaining state, baseline haemodynamic and renal studies were performed. In the evening at 10 00 pm prior to the baseline studies, or day 9 of the study, all study subjects received lithium carbonate 300 mg orally for measurement of lithium clearance, used as a measure of proximal tubular reabsorption of sodium.16 Assessments of baseline renal function, systemic haemodynamics, and neurohumoral factors were performed on day 10. Shortly after 8 00 am, an intravenous catheter was inserted. After two hours of bedrest in the supine position, blood was collected from all study subjects via an indwelling catheter without a tourniquet for measurement of serum electrolytes, plasma renin activity (PRA), plasma angiotensin II, and aldosterone levels. Measurements of inulin clearance, an index of glomerular filtration rate (GFR), p-aminohippurate clearance, an index of renal plasma flow (RPF), lithium clearance, and urinary sodium excretion were made for two periods of one hour each, with patients voiding while supine. Mean arterial pressure (MAP) and heart rates were assessed hourly during the renal study. In the afternoon at 2 00 pm, after fasting for at least six hours, all study subjects were transferred to the Nuclear Cardiology Department for measurements of central blood volume and systemic haemodynamics using radionuclide angiography. An additional 24 hour urine collection was made for estimation of urinary sodium excretion on the same day.
After a further period of seven days, while maintained on the 200 mmol sodium, 1.5 litre fluid per day diet, the haemodynamic and renal studies were repeated using the optimal dose of losartan. Study subjects received 300 mg lithium at 10 00 pm on the evening prior to the repeat studies. On the following morning at 6 00 am, all subjects received the optimal dose of losartan as assessed in the dose response study. Subsequently, measurements of renal and systemic haemodynamics, sodium excretion (both during the two hour renal study period and over 24 hours), central blood volume, and neurohumoral factors were repeated in exactly the same manner as the baseline measurements.
PROCEDURES
Inulin, p-aminohippurate, and lithium clearances
The techniques of inulin,p-aminohippurate, and lithium clearances have been reported previously.17 The average of the two collections for both the baseline and losartan studies represented the parameters measured during that particular study period.
Central blood volume measurements
Detailed description of the technique of central blood volume measurements using radionuclide angiography has been described previously.18 Briefly, red blood cells were labelled using technetium-99m pertechnetate. The cardiac volumes were measured based on regional activity corrected for attenuation and analysed using a semiautomated software. Quality assurance studies in our Nuclear Cardiology Laboratory have established the standard error of the estimate of ventricular volume calculation to be less than 5 ml.19
ANALYTICAL TECHNIQUES AND ASSAYS
Standard analytical methods were used to measure serum and urinary electrolytes and lithium. Blood samples for PRA, plasma angiotensin II, and aldosterone determinations were collected on ice with tubes for angiotensin II containing EDTA and aprotinin. Plasma was separated by refrigerated centrifugation and stored at −70°C until assay. Plasma renin activity was estimated by the radioimmunoassay of angiotensin I generated from plasma after one hour incubation at pH 5.5 and at 37°C in conditions inhibiting the further conversion of angiotensin I (Rianen assay system Angiotensin I [125I] kit, Dupont Company, Wilmington, Delaware, USA). Samples that yielded values of less than 0.1 ng/l/s were then reassayed and incubated for three hours. Plasma angiotensin II was measured by radioimmunoassay (Radioimmunoassay for Angiotensin II kit (human), Peninsula Laboratories, Belmont, California, USA). Plasma aldosterone was assayed using a radioimmunoassay technique with a commercial kit (Coat-A-Count Aldosterone kit, Diagnostic Products Corporation, Los Angeles, California, USA). Inulin concentrations in plasma and urine were measured by a modified technique of Walser et al,20 andp-aminohippurate, by a spectrophotometric method of Brun.21
CALCULATIONS
Inulin and p-aminohippurate clearances were corrected for body surface area and expressed per 1.73 m2. Renal vascular resistance (RVR) for each clearance period = MAP + renal blood flow; renal blood flow = RPF/(1 − packed cell volume). Proximal tubular reabsorption of sodium was calculated using lithium clearance and GFR, whereas the distal tubular reabsorption of sodium was calculated from inulin clearance, serum sodium concentrations, urinary sodium concentrations, and urinary volume.22
The end diastolic, end systolic, and central blood volumes were directly measured during radionuclide angiography. Stroke volume, cardiac output, and systemic vascular resistance (SVR) were then calculated from standard formulae.18 All volume measurements can be affected by body size and were therefore corrected for body surface area using the subject's height and weight. Likewise, the cardiac output was corrected for body surface area to yield the cardiac index.
STATISTICAL ANALYSIS
All results were expressed as mean (SEM). Differences between the means of the baseline and postdose observations during the dose response study for each variable in each group were determined by one way analysis of variance (ANOVA). For independent variables, paired and unpaired Student's t tests were used to analyse two means of each variable. Differences were considered significant if the null hypothesis could be rejected at the 0.05 probability level.
Results
DOSE RESPONSE STUDY
The mean 24 hour urinary sodium excretion in the preascitic cirrhotic patients for the three days prior to the dose response study was 147 (7) mmol/day, confirming that they were in a state of sodium retention. With the initial dose of 2.5 mg of losartan, there was an immediate natriuresis in the preascitic cirrhotic patients. However, this did not achieve statistical significance (table 1). With increasing doses of losartan, the natriuresis observed in the cirrhotic patients was maintained. The 7.5 mg dose, in contrast to 10 mg, did not result in a significant fall in the MAP (table 1) during the 12 hour observation period; it was therefore chosen as the optimal dose of losartan in this study. The fall in MAP with 10 mg of losartan was transient, observed three hours after losartan administration in the cirrhotic patients only; MAP gradually returned to baseline during the next 24 hours. The control subjects did not show any significant change in either urinary sodium excretion, MAP, or heart rate during the dose response study (table 1).
Haemodynamic and sodium excretion response following increasing single oral doses of losartan during the dose response study
RESPONSE TO 7.5 mg LOSARTAN
Sodium homoeostasis
Baseline studies were conducted on day 10, when all parameters had returned to levels similar to those prior to the dose response study. Urinary sodium excretion, both measured over a 24 hour period and during the two hour renal study period, was significantly lower in the preascitic cirrhotic patients compared with controls (154 (8) mmol/day versus 191 (12) mmol/day over the 24 hour collection period, p<0.05, table 2; and 0.16 (0.03) mmol/min versus 0.36 (0.05) mmol/min during the two hour renal study period, p<0.01, fig 1). The significantly reduced renal sodium excretion in the cirrhotic patients was due to an increase in the tubular reabsorption of sodium proximal to the distal tubule (73.64 (1.80)% versus 60.30 (4.95)% in controls, p=0.02, fig1). This resulted in a significant decrease in the fractional excretion of sodium in the cirrhotic patients (1.26 (0.23)% versus 1.91 (0.15)% in the controls, p=0.05).
Renal sodium handling, systemic and renal haemodynamics, and central blood volume before and after 7.5 mg losartan

(A) Urinary sodium excretion, (B) proximal tubular reabsorption of sodium, and (C) fractional excretion of sodium before and after 7.5 mg losartan in the cirrhotic patients and controls.
With 7.5 mg of losartan, renal sodium handling was normalised in the cirrhotic patients. Both the 24 hour urinary sodium excretion (202 (12) mmol/day, p=0.05 versus baseline) and the two hour urinary sodium excretion during the renal study period (0.27 (0.04) mmol/min, p=0.01 versus baseline) increased significantly (fig 1). This was associated with a weight loss of 0.32 (0.06) kg over the 24 hour period. The improved renal sodium handling in the cirrhotic patients was due to a significant decrease in the tubular reabsorption of sodium proximal to the distal tubule in the cirrhotic patients (p=0.05, fig 1), leading to an improved distal delivery of sodium. The distal tubular reabsorption of sodium, however, was not affected by losartan, therefore resulting in a significant increase in the fractional excretion of sodium (1.68 (0.25)%, p=0.05 versus baseline, fig 1). No change in sodium handling following losartan was observed in the control subjects.
Systemic haemodynamics and central blood volume
At baseline, the mean MAP measured during the two hour renal study period was lower in the cirrhotic patients compared with controls, but the difference was not statistically significant (table 2). Following 7.5 mg of losartan, there were no significant changes in the mean MAP, heart rate, SVR, and cardiac index in both the control subjects and cirrhotic patients (table 2). Central blood volume and cardiac volumes also did not change significantly with 7.5 mg of losartan in both groups (table 2).
Renal haemodynamics
Baseline GFR, RPF, and RVR were not significantly different between the two groups (table 2). Losartan 7.5 mg did not affect renal haemodynamics in either the control subjects or the cirrhotic patients (table 2).
Neurohumoral factors
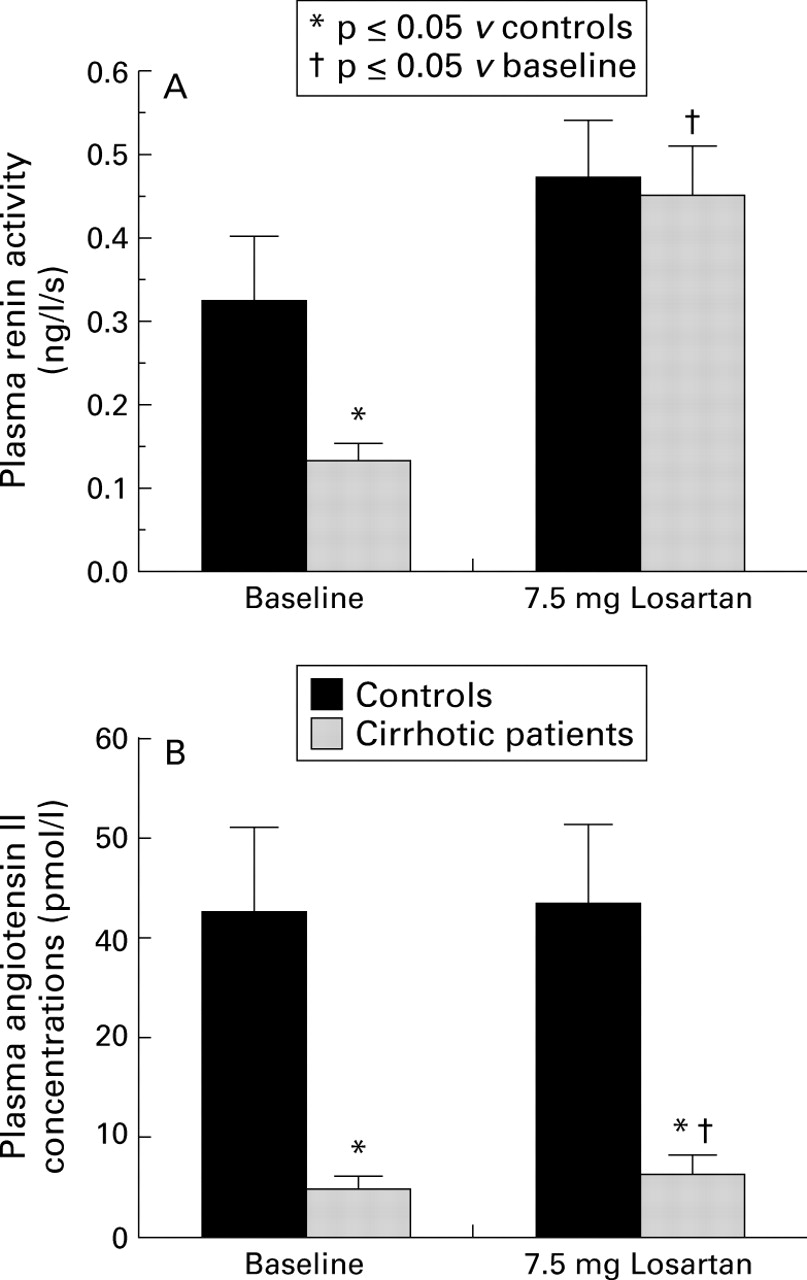
Baseline systemic angiotensin II levels, measured in the supine posture, were significantly lower in the preascitic cirrhotic patients compared with controls (6 (2) pmol/l versus 40 (10) pmol/l in controls, p<0.01). With 7.5 mg losartan, supine systemic levels of angiotensin II increased significantly in cirrhotic patients (8 (2) pmol/l, p<0.05 versus baseline) but not in controls (fig 2). Systemic angiotensin II levels in cirrhotic patients, however, remained consistently lower than those in controls (fig 2). The baseline supine PRA was also significantly lower in cirrhotic patients (0.13 (0.02) ng/l/s) compared with controls (0.32 (0.08) ng/l/s, p<0.05, fig 2). With 7.5 mg losartan, there was a significant increase in PRA in preascitic cirrhotic patients (0.45 (0.06) ng/l/s versus 0.13 (0.0) 2 ng/l/s at baseline, p=0.05, fig 2). The change in PRA in control subjects (0.47 (0.07) ng/l/s), however, was minimal (fig 2). Likewise, supine baseline plasma aldosterone levels were lower in preascitic cirrhotic patients compared with controls (95 (15) pmol/l versus 136 (30) pmol/l in controls, p>0.05) and did not change with losartan (100 (11) pmol/l in cirrhotic patients and 112 (17) pmol/l in controls) in both groups.

{kind=link}
{kind=link}
(A) Plasma renin activity, (B) plasma angiotensin II levels, before and after 7.5 mg losartan in cirrhotic patients and controls.
Discussion
The results of this preliminary study confirm previous findings that preascitic cirrhotic patients have subtle sodium retention when placed on a 200 mmol sodium as opposed to a 100 mmol sodium per day intake,1 2 23 manifested as a reduced urinary sodium excretion, associated with suppression of systemic RAAS in the supine posture. The acute use of a low dose angiotensin II receptor antagonist resulted in normalisation of this subtle sodium handling abnormality in preascitic cirrhotic patients, despite unchanged renal and systemic haemodynamics.
A 200 mmol sodium per day diet was chosen for this study for several reasons. Preascitic cirrhotic patients have previously been shown to come into a steady state of subtle sodium retention after four days of this sodium intake,2 and therefore the study would not require a long run in period. Secondly, this level of sodium intake, although higher than that contained in the usual “no added salt diet of 100–130 mmol sodium per day” that the patients were accustomed to, was similar to their usual diet with a few additional high salt items and therefore easily manageable. Thirdly, this level of sodium retention was sufficient to assess the natriuretic effect of losartan.
This subtle sodium handling abnormality in preascitic cirrhosis has been shown to result in intravascular volume expansion.24 25 The supine posture is the means whereby some of this excess volume can be eliminated,26 as may have occurred in the present study, since the central blood volume in the cirrhotic patients was not significantly increased. Therefore, this study was performed in the supine posture to examine what additional mechanisms are involved in the pathophysiology of sodium retention in preascitic cirrhosis.
The proximal renal tubule has previously been identified as an important site of renal sodium retention in cirrhosis.4 27 The two most likely candidates for increased proximal tubular reabsorption of sodium in preascitic cirrhotic patients are: (1) an increase in renal sympathetic nervous system (SNS) activity, since a subtle increase in systemic SNS activity, unmasked by a high sodium diet, has been observed in preascitic cirrhosis28; (2) alternatively, an increase in intrarenal production of angiotensin II,5 possibly mediated by portal hypertension.29
Recent work from our laboratory showed that, in preascitic cirrhosis, the application of lower body negative pressure at −20 mm Hg for 30 minutes, which simulates an upright posture, led to a significant increase in renal angiotensin II production, together with unchanged renal SNS activity, as measured by renal noradrenaline spillover technique.5 This indicates that activation of the intrarenal RAAS may be the first of a series of events involved in the abnormality in sodium homoeostasis in preascitic cirrhosis. All components of the RAAS are present within the kidney, thereby allowing significant amounts of angiotensin II to be formed intrarenally.30 31 The logical extension of this observation is to manipulate the RAAS to assess the resultant changes in renal sodium excretion. Recent characterisation of angiotensin II receptors in various tissues with the subsequent development of angiotensin II receptor antagonists, has provided an exciting investigational tool to assess angiotensin II function. The prototype, losartan, being less vasodepressive than ACE inhibitors,13has consistently been shown to be well tolerated with minimal side effects,32-34 thus making it a very attractive probe for the study of angiotensin II effects on sodium handling in cirrhosis.
The effects of losartan on systemic and renal haemodynamics, and neurohumoral factors has been extensively evaluated in healthy normal volunteers14 35-37 and in patients with systemic hypertension38 or congestive cardiac failure.39 While the effects of losartan last for up to 24 hours, a clear dose dependent relation exists between losartan and the observed effects.14 Therefore, in order to produce as pure an angiotensin II action as possible without the confounding effect of systemic hypotension, a low dose of losartan was required. Our dose response study indicated that a dose of 7.5 mg of losartan was the optimal dose that produced a natriuresis without any systemic hypotension in the cirrhotic patients.
The improved renal sodium excretion with the acute administration of low dose losartan, in preascitic cirrhosis, was due to a decrease in the tubular reabsorption of sodium proximal to the distal tubule. In the absence of any change in GFR or RPF, this would suggest that angiotensin II had a direct sodium retaining effect on the renal tubule. Indeed, sodium retention has been shown to be independent of changes in renal haemodynamics following angiotensin II infusion.40 41 Furthermore, the proximal renal tubule has been shown to contain a large number of angiotensin II receptors,42 43 which are much more sensitive to angiotensin II than receptors of the renal efferent arterioles and zona glomerulosa of the adrenal gland.44 The fact that 7.5 mg of losartan had no effects in the controls but improved sodium excretion in the preascitic cirrhotic patients would suggest that there must have been activation of their intrarenal as opposed to the systemic RAAS, since systemic levels were actually lower in the cirrhotic patients. Alternatively, the preascitic cirrhotic patients were more sensitive than the controls to the direct sodium retaining effect of angiotensin II on the renal tubule. Finally, the use of losartan may have reduced portal pressure,45 which has been shown to be involved in the pathogenesis of sodium retention in cirrhosis.17 However, this remains speculative, as portal pressure was not measured in this study, and the dose we used was substantially smaller than the portal pressure lowering dose reported.45
The increase in urinary sodium excretion following the acute administration of a low dose of losartan was not accompanied by any change in the central blood volume or cardiac volumes. This may at first seem surprising since the negative sodium balance would be expected to be accompanied by a negative volume balance. This may be due to the fact that the volume change after a single low dose of losartan was insufficient to alter the central blood volume. Alternatively, the change in volume may not have occurred in the central compartment, but rather in another circulatory bed such as the splanchnic circulation.
The fact that the sodium retaining effects of angiotensin II can be dissociated from its haemodynamic effects has provided important insights into the pathogenesis of sodium retention in cirrhosis. An increased tubular reabsorption of sodium may represent the first abnormality in the sodium homoeostasis in these patients. As the cirrhotic disease progresses, abnormalities in the circulation may then contribute to further sodium retention in these patients.
The neurohormones at baseline were lower in the preascitic cirrhotic patients, significantly so with systemic angiotensin II levels. This is consistent with the finding of subtle renal sodium retention, suggesting intravascular volume expansion. Following the acute administration of 7.5 mg losartan, angiotensin II receptor blockade leading to activation of the RAAS through removal of the negative feedback mechanism, should have caused an increase in PRA in both groups. However, PRA only increased significantly in the cirrhotic patients but not in the controls. The most likely explanation is that in the cirrhotic patients, additional mechanisms such as an increased sensitivity of the renal baroreceptor mechanism stimulate renal renin release.46 47 The angiotensin II thus formed must have been produced intrarenally, possibly at a tissue level, and then metabolised intrarenally, as the systemic levels of angiotensin II remained low following losartan compared with the controls and consequently, the plasma aldosterone levels remained unchanged.
The ability of a single low dose of losartan to effect a natriuresis without any deleterious systemic hypotensive effects certainly establishes its clinical advantage over ACE inhibitors. Further studies still need to be performed to determine whether the long term administration of low dose losartan can maintain the natriuretic response in preascitic cirrhotic patients. If positive, this may normalise their volume status and prevent or delay the development of the hyperdynamic circulation. Similar studies also need to be performed to assess the effects of losartan in ascitic patients.
In summary, the use of a single low dose of the angiotensin II receptor antagonist, losartan, in preascitic cirrhotic patients improved renal sodium handling and normalised the subtle sodium handling abnormality in these patients unmasked by a 200 mmol sodium diet. This occurred without any significant change in systemic or renal haemodynamics, suggesting a direct renal tubular effect of losartan in inducing a natriuresis. This study therefore supports the pivotal role of the RAAS in the control of sodium homoeostasis in preascitic cirrhosis.
Acknowledgments
Dr Nigel Girgrah is the recipient of the Resident Research Grant from The Physicians Services Inc. of Ontario, Canada. Dr Jane Collier is the recipient of the Schering's Hepatology Fellowship from Schering Canada Inc. Dr Florence Wong is the recipient of the Fellowship from The Medical Research Council of Canada. The study was supported by a Research Grant from the Kidney Foundation of Ontario, Canada. Special thanks are extended to Yasmin Allidina of the Nuclear Cardiology Department for the patient hours of image analysis and data entry. The authors also wish to thank Sue Chong, dietetic assistant, and the nursing staff of the Clinical Investigation Unit at Toronto Hospital for their expert assistance and generous support.
References
Footnotes
- Abbreviations used in this paper:
- ACE
- angiotensin converting enzyme
- GFR
- glomerular filtration rate
- MAP
- mean arterial pressure
- PRA
- plasma renin activity
- RAAS
- renin-angiotensin-aldosterone system
- RPF
- renal plasma flow
- RVR
- renal vascular resistance
- SNS
- sympathetic nervous system
- SVR
- systemic vascular resistance