Article Text

Abstract
BACKGROUND Ingestion of a meal stimulates colonic motility. It is unclear whether the nutrient composition of a meal affects colonic motor response.
AIMS To investigate and compare the effects of a predominantly fat or carbohydrate meal on colonic motility.
METHODS In 18 healthy subjects, ambulatory colonic manometry was performed by placing a six sensor, solid state probe from the mid-transverse colon to the rectum. In a randomised, crossover design, 10 and 27 hours after probe placement, subjects received 4.18 MJ meals containing 60% calories from fat or carbohydrate sources. Preprandial and postprandial pressure activity and motor patterns were evaluated.
RESULTS Both meals induced phasic activity with a greater area under the curve (p<0.03) in the first postprandial hour, compared with the control period. Fat induced motor activity persisted longer (p<0.05) than that of the carbohydrate meal, but the onset of motor response was slower (p<0.001). Although both meals induced more (p<0.001) propagating pressure waves, only the fat meal induced more (p<0.05) simultaneous and retrograde waves. After both meals, 50% of subjects exhibited high amplitude (more than 103 mm Hg), prolonged duration (more than 13 seconds) propagating waves. Both meals induced greater activity (p<0.05) in the transverse/descending colon than in the rectosigmoid colon.
CONCLUSIONS Carbohydrate meals induce colonic motor response, but the effects are short lived when compared with fat meals. The prolonged, segmental, and retrograde phasic activity induced by the fat meal may delay colon transit. Thus meal composition influences colonic motor response.
- fat
- carbohydrate
- meals
- colon motility
- gastrocolonic response.
Statistics from Altmetric.com
Meal induced motor activity of the colon is often described as the gastrocolic reflex.1 However, this is not a specific colonic reflex because meals stimulate motor activity throughout the gut, including the colon.2 3 Hence, this physiological event is more aptly described as the colonic motor response to a meal.4-9 Although well documented,7-16 several aspects of this response remain unclear.
Humans consume a variety of meals whose energy and nutrient composition is variable. It has been shown that a 4.18 MJ meal but not a 1.46 MJ meal stimulates colonic motor activity.15 This suggests that the energy content of a meal may influence the colonic motor response. Similarly, the fibre content of a meal has also been shown to influence colonic transit.17 But whether the fat or carbohydrate composition of a meal affects the colonic motor response is unclear. Wright and colleagues16 showed that a 2.5 MJ fat meal (olive oil) enhanced colonic spike activity but a 2.5 MJ carbohydrate meal (glucose) did not induce spike activity—that is, carbohydrates do not produce a colonic motor response. Although they are nutrient solutions, however, olive oil and glucose are not typical meals. Furthermore, they differ significantly in their osmolality, pH, and other characteristics, which can affect upper gastrointestinal motor activity18-21 and consequently colonic motility.2
It is currently recommended that a healthy diet should contain at least 55% of energy from a carbohydrate source.22 The effects of such a meal on colonic motor activity have not been investigated. If a carbohydrate meal does not induce a colonic motor response,16 then this may have implications for the dietary management of patients with colonic disorders such as constipation.
In the canine colon, an early (within 60 minutes) and a late (2–6 hours) colonic motor response have been described.6 An early, immediate, and late colonic response has also been suggested.5 It is not known, however, whether the human colon exhibits a similar pattern. Some studies have suggested that the postprandial response lasts for one hour,9 14 15 but one study indicated that it lasts for several hours.8 These discrepancies may be due to the short duration of recording,9 14 15 23 colon cleansing,23 or lower fidelity recording systems.11 13 23 Recent studies have also shown that meals increase colonic tone,12 24 25 but there is only sparse information regarding colonic motor patterns.
The aim of our study, therefore, was to perform prolonged recordings of postprandial colonic motility in healthy humans, under ambulatory conditions, in order to characterise and compare the effects of a high fat or high carbohydrate meal.
Methods
SUBJECTS
Nineteen healthy volunteers (10 men, nine women, aged 23–55 years) were recruited through a hospital advertisement. All subjects gave written informed consent, and the human subjects review committee of the College of Medicine approved the study protocol. No subject had any previous history of gastrointestinal symptoms, lactose intolerance, or abdominal surgery, and none was taking medication. They all had a normal physical examination and were within 20% of ideal body weight.
EXPERIMENTAL DESIGN
Subjects were admitted to the Clinical Research Center at 7 00 am and received a tap water enema. At 7 30 am, a flexible 6.5 mm diameter silastic probe with six strain gauge microtransducers (Gaeltec Limited, Isle of Skye, UK), was placed in the colon, with the help of a colonoscope. The technique has been described in detail previously.26 Fluoroscopy was performed to check that the pressure sensors were approximately located at 7, 14, 25, 35, 45, and 60 cm from the anus with the tip in the mid-transverse colon. These distances between the sensors were chosen to optimise the location of transducers in the rectum, sigmoid colon, descending colon, and transverse colon. The total radiation exposure did not exceed 1144 microrad per subject. The probe was taped securely to the gluteal region and was connected to a portable recorder (MPR-7, Gaeltec, Isle of Skye, UK) that was placed in a shoulder bag. The multichannel recorder had 1 MB memory with a sampling frequency of 8 MHZ. The subjects were free to move. Approximately 10 hours (day 1, 6 00 pm) and 27 hours (day 2, 11 00 am) after probe placement, all subjects received two meals in random order: a high fat or an isoenergy high carbohydrate meal of similar volume. On the second day, after waking and again four hours after consuming the second meal, fluoroscopy was repeated to check for probe migration. The probe was subsequently removed.
FAT MEAL
This meal consisted of a roast beef sandwich on white bread (180 g) with mayonnaise (22 g), milkshake (150 g), vanilla ice cream (130 g), and a non-energy beverage (240 ml). The total energy value of this meal was 4.43 MJ. The energy distribution of the meal was 60% fat, 20% carbohydrate, and 20% protein and the fibre content was 1.2 g. A similar meal has been used previously15 16 for measuring meal stimulated colonic responses.
CARBOHYDRATE MEAL
This meal consisted of a roast beef sandwich on white bread (226 g) with fat free mayonnaise (25 g), skim milk (240 ml), apple juice (240 ml), sherbet (80 g), angel food cake (50 g), and a non-energy beverage. The total energy value of this meal was 4.37 MJ. The energy distribution was 60% carbohydrate, 21% protein, and 19% fat and the fibre content was 3 g.
MEASUREMENTS AND ANALYSIS
Colonic pressure activity and the patterns of motor activity were analysed by separate investigators, who were unaware of the type of meal consumed by each subject. Colonic pressure activity was assessed both manually and with the aid of a software analysis program (Gaeltec, Isle of Skye). Pressure waves with an amplitude of at least 8 mm Hg and duration of at least 3 seconds were included in the analysis26 27; specifically, for the one hour period before each meal (control period) and for each of the first three hours postprandially, the number of waves/hour, the percentage time when motor activity was seen, and the area under the curve of pressure waves were measured. These parameters were analysed with the help of a DOS based software program (AMBB; Gaeltec, Isle of Skye, UK). The three hour postprandial limit was chosen because pilot studies showed that in the fourth postprandial hour, colonic motor activity returned to baseline after both meals. In order to examine the segmental variation of pressure activity, we compared data from the transverse/descending colon (proximal channels; P1–P3) and the rectosigmoid region (distal channels; P4–P6).
When colonic motor patterns were assessed, at least five different patterns were found (described below). However, our software program was unable to assess reliably and consistently the various types of motor patterns. Hence, we analysed the data manually by scanning each page on a monitor at different speeds (range 30 s/page to 4 min/page) and at variable gain settings. One investigator who was unaware of other manometric data or the order of meals performed this assessment. The following patterns were recognised:
Propagating pressure waves
Defined as pressure waves that propagate aborad across three or more consecutive channels with a velocity of 0.5–2.4 cm/s28 29 (fig 1A). The differential spacing between sensors was taken into account when calculating the propagation velocity.
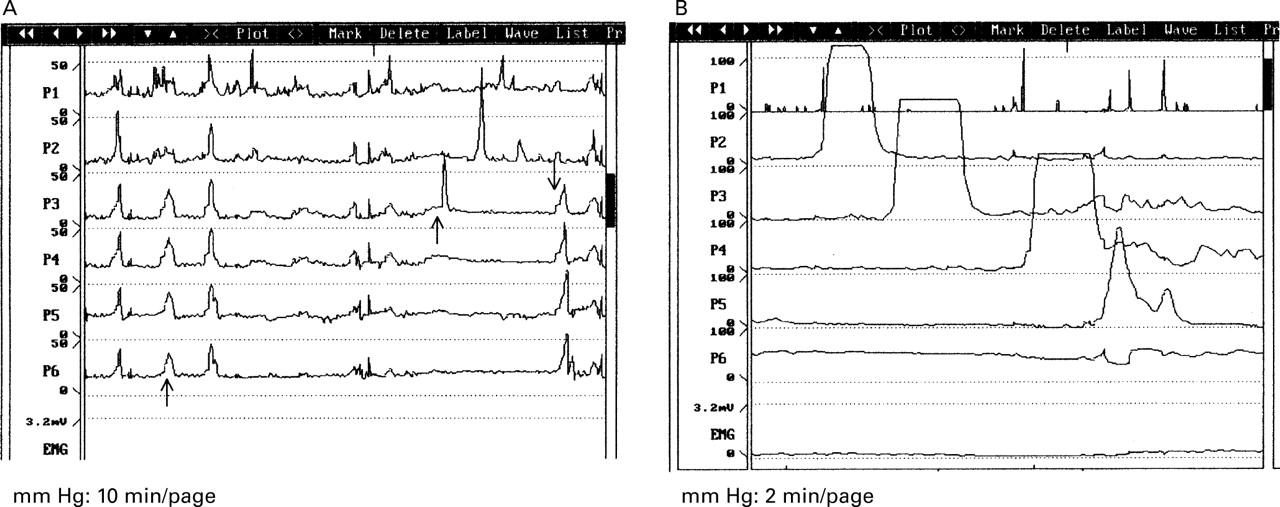
Typical examples of meal induced pressure waves. (A) Simultaneous pressure waves seen in P1–P6, retrograde pressure waves seen in P3–P1, and propagating pressure waves seen in P3–P6. (B) Specialised propagating pressure waves (high amplitude, prolonged duration).
Specialised propagating pressure waves
Specialised propagating pressure waves are defined as a distinct pattern of propagated waves that migrated aborad across three or more consecutive channels (fig 1B) with a high amplitude (more than 103 mm Hg) and a prolonged duration (more than 13 seconds).28 An amplitude of 103 mm Hg and a duration of 13 seconds were chosen because these values were greater than the 95% confidence interval for ordinary propagated pressure waves in the colon.30
Simultaneous pressure waves
Simultaneous pressure waves are defined as pressure waves occurring simultaneously in three or more channels with an onset time of less than 0.5 cm/s between two consecutive channels (fig 1A).
Periodic rectal motor activity
Periodic rectal motor activity consisted of discrete bursts of phasic contractions, at three cycles per minute and with a cycle duration of at least five minutes, that was confined to the rectal or rectosigmoid channel.26
Retrograde pressure waves
Retrograde pressure waves are defined as pressure waves that migrated in an orad direction across three or more consecutive channels with a velocity of 0.5–2.4 cm/s (fig 1A). Also, for each meal, we calculated the time of onset of pressure activity or cyclical activity in the colon (2–4 pressure waves/min) that lasted three or more minutes.
STATISTICS
In order to characterise the meal responses and to determine the effect of fat and carbohydrate content of meals on colonic motility, the manometric data that were obtained during the first, second, and third postprandial hours were compared with a baseline period (one hour before each meal). The significance of differences between the effects of each meal (control versus meal) and the type of meal (fat versus carbohydrate) were compared by using analysis of variance (ANOVA) for repeated measures. Mean contrasts were evaluated byt test and Bonferroni's method was applied to compare and adjust for the multiple comparisons that were performed. Results are expressed as mean (95% confidence interval (CI)).
Results
SUBJECTS
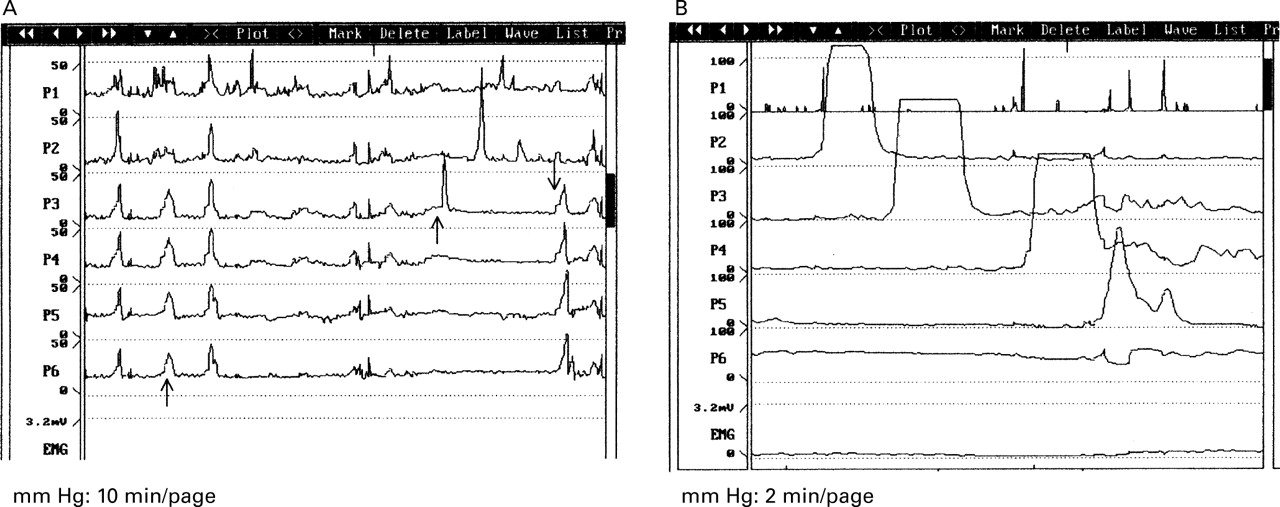
All subjects consumed both meals within 20 minutes. Owing to probe migration, data from one subject were omitted; the results from 18 subjects were analysed. Immediately after ingestion of a meal, there was a prompt increase in colonic pressure activity in all subjects (fig2). Randomisation of meals ensured that the order in which the meals were given did not affect the gastrocolonic response. We found that the two meals induced differential effects on colonic motor response.

Typical changes in colonic motor activity in the same individual, before and after ingestion of: (A) a predominantly fat meal; and (B) a predominantly carbohydrate meal. P1, transverse colon; P2, splenic flexure; P3 and P4, descending colon; P5, sigmoid colon; P6, rectum. After the fat meal, pressure waves persisted for over three hours. After the carbohydrate meal, pressure activity decreased after 2.5 hours. The proximal colonic segments (P1–P3) showed greater activity than the distal (P4–P6) colonic segments.
EFFECTS OF A FATTY MEAL
Pressure activity
When compared with the control period, the number of pressure waves, the area under the curve, and the percentage of recording time when pressure activity occurred were higher (p<0.05) during the first hour following the meal (table 1). The area under the curve was also higher during the second and third hours (fig3).
The effect of each meal on colonic pressure activity and on the duration of response

{kind=link}
{kind=link}
{kind=link}
Effects of each meal on the area under the curve (AUC) of pressure waves. Results expressed as mean (95% confidence interval). * p<0.05 Meal versus control, † p<0.05 fat versus carbohydrate.
Wave patterns
Isolated, simultaneous or propagating pressure waves were seen throughout the four hour period and in each subject (table 2). When compared with the control period, a greater (p<0.05) number of propagating waves and simultaneous waves was seen during all three hours following the meal (table 2). Also, there was a higher (p<0.05) number of retrograde waves in the first hour following the meal compared with the control period (table 2). The mean amplitude of propagating pressure waves did not change significantly (table 2). Periodic rectal motor activity (PRMA) was observed during the preprandial and postprandial hours, but its incidence was not affected by meals (table 2). When compared with the control period, during the first postprandial hour, more subjects exhibited specialised propagating waves (table 3). Although higher, the number of waves was not significant. Seven (39%) subjects did not show specialised propagating waves postprandially. The amplitude, duration, and velocity of propagation of these pressure waves were not affected by the meal.
Patterns of colonic motor activity after ingestion of a high fat meal and a high carbohydrate meal
Incidence and motor characteristics of specialised (high amplitude and prolonged duration) propagating waves
Regional differences
When compared with the control period, the area under the curve of pressure activity was significantly higher (p<0.05) in the transverse/descending colon than in the rectosigmoid colon, during the first postprandial hour (table 1). Also, the area under the curve in the transverse/descending colon was higher during all three hours compared with the control period, but not in the rectosigmoid colon (table 1).
EFFECTS OF A CARBOHYDRATE MEAL
Pressure activity
The number of pressure waves, the percentage activity (table 1) and the area under the curve of pressure waves (fig 3) increased (p<0.05) significantly during the first postprandial hour. During the second and third postprandial hours, the pressure activity decreased to control values (table 1).
Wave patterns
During the first postprandial hour there was a higher (p<0.05) incidence of propagating waves, but not simultaneous or retrograde waves (table 2). The number of simultaneous waves actually decreased (p<0.05) in the third postprandial hour compared with the preprandial period (fig 3). Postprandially, the mean amplitude of pressure waves did not change significantly (table 2). When compared with the control period, during the first hour more subjects showed specialised propagating waves with a higher incidence (table 3). The difference was not significant. The amplitude, duration, and velocity of propagation of these waves were not affected by the meal. PRMA was observed and its incidence was unchanged during the first two hours, but there was a higher incidence during the third postprandial hour (table2).
Regional differences
When compared with the control period, the area under the curve of pressure waves was greater (p<0.05) in the transverse/descending colon than in the rectosigmoid colon during the first postprandial hour, but not during the next two hours (table 1).
COMPARISON OF HIGH FAT AND HIGH CARBOHYDRATE MEALS
The onset of pressure activity or cyclical activity was quicker (p<0.001) after the carbohydrate meal when compared with the fat meal. After ingestion of the carbohydrate meal, the colonic motor activity and cyclical activity were induced at 41.3 (18.8) and 62.1 (18.5) seconds, respectively, whereas after ingestion of the fat meal they were induced at 162 (21.3) and 356 (52) seconds, respectively. Unlike the carbohydrate meal, the fat induced pressure activity persisted well into the second and third postprandial hours (p<0.05) when compared with the control period (fig 3). Both meals induced a greater (p<0.001) number of propagating waves during the first hour (table 2). Only the fat meal, however, induced a greater (p<0.05) number of simultaneous waves during the three hours and retrograde pressure waves during the first hour (table 2). Furthermore, the fat meal induced a significantly higher (p<0.05) number of simultaneous waves than the carbohydrate meal (table 2).
Discussion
Although the colonic motor response which occurs after a fat meal has been described previously,14 16 27 31 this is the first study that has examined colonic manometry after ingestion of a predominantly fat or carbohydrate meal within the same individual. Unlike a previous report,16 we found that a carbohydrate meal not only induced a colonic motor response, but the magnitude of response during the first hour was comparable to that of an isoenergy fat meal.
In the previous study,16 glucose or olive oil were used as opposed to a whole meal, the energy content of the two meals was lower, and the electrical spike activity was recorded from a limited segment (rectosigmoid region only). In this context, our finding that both meals induced greater motor activity in the transverse/descending colon than the rectosigmoid colon is important. This observation not only confirms previous studies,12 27 32 but underscores the fact that colonic motor changes can be missed or misinterpreted if motor activity is recorded from a limited segment. In addition to the examination of a longer segment, we also sought to minimise the effects of colon cleansing,11 13 the effects of infusing fluid into the colon, and the effects of meal consistency, by assessing the colonic motor responses at 10 and 27 hours after probe placement, by using solid state technology, and by giving whole meals rather than liquid meals.12 The smell, sight, and taste of food may each influence colonic motor activity.33 We sought to minimise these influences by presenting meals that looked similar in volume, colour, smell, and appearance. Thus, our study was performed under more physiological conditions.
We cannot exclude the possibility that the small amount of fat which was present in the carbohydrate meal may have exerted some effect on the colonic motor response. The fat component of the carbohydrate meal, however, accounted for only 0.8 MJ, an energy load that does not induce a colonic motor response.15 Furthermore, the differential effects on motor activity and on motor patterns would argue in favour of a direct effect of the carbohydrate component.
Unlike observations in the canine colon,6 we did not observe an early and late colonic response in humans. In one human study a possible bimodal response has been described.12The duration of recording in this study, however, was only 90 minutes, and therefore was insufficient to provide information regarding the late response. Also, a liquid meal was given.12 In contrast, we found that the colonic motor response reverted to the preprandial state within three to four hours, and thereafter no further increase was seen. The late colonic response has been ascribed to the motor activity induced by the arrival of meal residues into the caecum.5 We did not find evidence to support this concept. Instead, our findings suggest that ingestion of a meal seems to be a more important stimulus for colonic motor activity. Whether more frequent ingestion of meals stimulates a greater response merits further study.
After a carbohydrate meal, the onset of motor activity was quicker, albeit small, but the duration of motor response was clearly shorter when compared with the fat meal. Because the colonic motor response may be induced by stimulation of mechanoreceptors in the upper gut2 and possibly mediated by neurohormonal mechanisms,2 31 34 the differential effects of the two meals may be due to either the rate of transit of each meal through the upper gut or the stimulation of different neurohormones or receptors. Previously, it has been shown that meals containing fat delay gastric and small bowel transit.19 35 The infusion of fat into the duodenum also induces a duodenal brake.18 These effects are probably due to the stimulation of specialised mucosal cells such as I cells of the duodenojejunum that secrete cholecystokinin,2 31 34 or due to the release of peptide YY,36 both of which can delay gastric emptying. Thus, the prolonged colonic motor response that is induced by a fat meal may in part be due to the slower transit of this meal through the upper gut and the release of cholecystokinin.31 34 In contrast, the shorter duration and the more rapid onset of the colonic motor response after a carbohydrate meal may be due to the more rapid transit of this meal through the stomach and small bowel.
In order to obviate any bias, the motor patterns were analysed by one investigator who was unaware of the meal composition or the results of other motor parameters. We found that 50% of subjects exhibited high amplitude, prolonged duration, specialised propagating waves after either meal. In those subjects who exhibited this phenomenon, on average one or two specialised propagating sequences were seen. This incidence was much higher than that reported previously11 12 34 and could be due to the more physiological conditions of our study. This finding not only confirms previous observations,37 but suggests that strong propagating waves may shift a larger volume of stool postprandially, particularly when there are no opposing simultaneous or retrograde pressure waves. Similar patterns described previously have been termed high amplitude propagating contractions11 28 in humans and giant migrating contractions5 6 in dogs. Because these waves are not only of a high amplitude but also of prolonged duration (more than 13 seconds), we felt that specialised propagating pressure waves may be a more appropriate term for describing these waves.
We also found that both meals induced a greater number of propagating pressure waves when compared with the preprandial hour. The incidence of simultaneous and retrograde pressure waves showed a differential response, however. After a carbohydrate meal there was a distinct drop off in their incidence, but after a fat meal this pattern persisted for three hours. Because diarrhoea is associated with decreased phasic activity38 39 and constipation with excessive phasic pressure activity,38 40 it is possible that the aforementioned effects of a fat meal on colonic motility may delay stool transport. In contrast, the increased number of propagating and specialised propagating pressure waves that were induced by a carbohydrate meal without an associated increase in the simultaneous or retrograde pressure waves (particularly in the second and third postprandial hours) is less likely to impede stool transport.35 As colon transit was not assessed in this study, however, our statement(s) should be interpreted with caution.
Our investigation reveals that both fat and carbohydrate meals induce a colonic motor response with 50% of subjects exhibiting high amplitude, prolonged duration, propagating pressure waves. The duration of phasic activity appears to depend on nutrient composition: a higher fat content is associated with a more prolonged colonic motor response. Thus, nutrient composition of a whole meal appears to influence the colonic motor response.
Acknowledgments
We are grateful to Mrs Bridget Zimmerman, Biostatistician, Clinical Research Center, UIHC, for her help with the statistical analysis. We also thank P Sadeghi for his help with the manuscript. This work was supported by a grant from the AGA-SKF Beecham Clinical Research Award and Grant RR00059 from the General Clinical Research Center's Program, National Institute of Health.
References
Footnotes
- Abbreviation used in this paper:
- PRMA
- periodic rectal motor activity
Linked Articles
- Commentary