Article Text

Abstract
BACKGROUND Eradication of Barrett's mucosa by thermal or photoablation combined with high doses of proton pump inhibitors is a potentially attractive strategy in the management of this preneoplastic condition. However, major concerns of this method are the persistence of residual metaplastic glands beneath the new squamous epithelium and the absence of any knowledge of its impact on long term outcome.
CASE REPORT The case of an intramucosal adenocarcinoma diagnosed 18 months after apparently complete squamous re-epithelialisation achieved using argon plasma coagulation and high dose omeprazole (40 mg/daily) is reported in a 68 year old patient presenting initially with a Barrett's oesophagus without dysplasia. Intramucosal adenocarcinoma was located under the new squamous layer and presented as a bulging area covered by the squamous epithelium. It probably originates from residual metaplastic glands after therapy although a pre-existing tumour cannot be definitely excluded.
CONCLUSION This observation might question future application of this experimental endotherapy in non-dysplastic Barrett's oesophagus. It suggests that the residual glands might still be premalignant and that the early diagnosis of neoplastic changes might be compromised by the squamous re-epithelialisation.
- argon plasma coagulation
- Barrett's oesophagus
- omeprazole
Statistics from Altmetric.com
Barrett's oesophagus is a premalignant condition in which the normal stratified squamous epithelium is replaced by a specialised columnar epithelium referred to as intestinal metaplasia.1Recently, thermal ablation or photoablation of Barrett's oesophagus combined with suppression of acid secretion have been reported as able to lead to squamous re-epithelialisation.2 3 A precursor progenitor cell within the metaplastic tissue was suggested to harbour the potential to differentiate into either squamous epithelium or specialised columnar epithelium.4 5 Several studies have confirmed the effectiveness of laser therapy, photodynamic therapy, multipolar electrocoagulation, and argon plasma coagulation (APC) combined with acid suppression for successfully ablating Barrett's oesophagus and inducing re-epithelialisation.5-9
However, an important finding, which is found in several of the reported series is the persistence of columnar epithelium remnants beneath the new squamous epithelium.6 8 9 This finding is observed whatever the technique used for Barrett's oesophagus ablation and the relevance of these residual glands in the outcome of re-epithelialised mucosa remains unknown. There are no available data showing that the apparent squamous re-epithelialisation after such treatment is able to avoid further development of dysplasia and/or cancer, as the maximal follow up period reported is 12 to 18 months.6-9 The recent results we have previously reported also suggested that relapse of Barrett's oesophagus may occur rapidly after re-epithelialisation.9 We report a case where an intramucosal adenocarcinoma was evidenced within the treated Barrett's segment beneath the new squamous layer, suggesting that residual metaplastic glands below the squamous mucosa might still harbour a malignant potential.
Case report
A 68 year old man with a long history of gastro-oesophageal reflux was diagnosed at endoscopy as having an 8 cm circumferential Barrett's segment above a hiatal hernia. Four quadrants biopsies (a total of 20 biopsies) performed every 2 cm confirmed the presence of intestinal metaplasia without dysplasia. The patient was informed and accepted for inclusion into an experimental protocol approved by our local ethics committee.9 The purpose of this protocol was to evaluate the potential for complete squamous re-epithelialisation of Barrett's oesophagus after APC coagulation and its mid-term outcome.9 Barrett's mucosa was thermoablated using APC over four sessions on an ambulatory basis. The patient received 40 mg omeprazole daily starting before the first APC treatment and continued to receive it during and after the endotherapy. After four APC sessions, complete eradication of Barrett's oesophagus was visualised at endoscopy with a squamous appearing mucosa replacing the previous specialised columnar epithelium (fig 1). Histologically, some remaining metaplastic glands were evidenced beneath the new squamous epithelium, localised in the distal part of the treated segment just above the new squamoglandular junction (fig 2). The patient continued to receive 40 mg omeprazole daily. Endoscopy with multiple biopsies was performed every six months and was planned for three years in the setting of the experimental protocol. No dysplastic foci were evidenced during the first year of follow up.
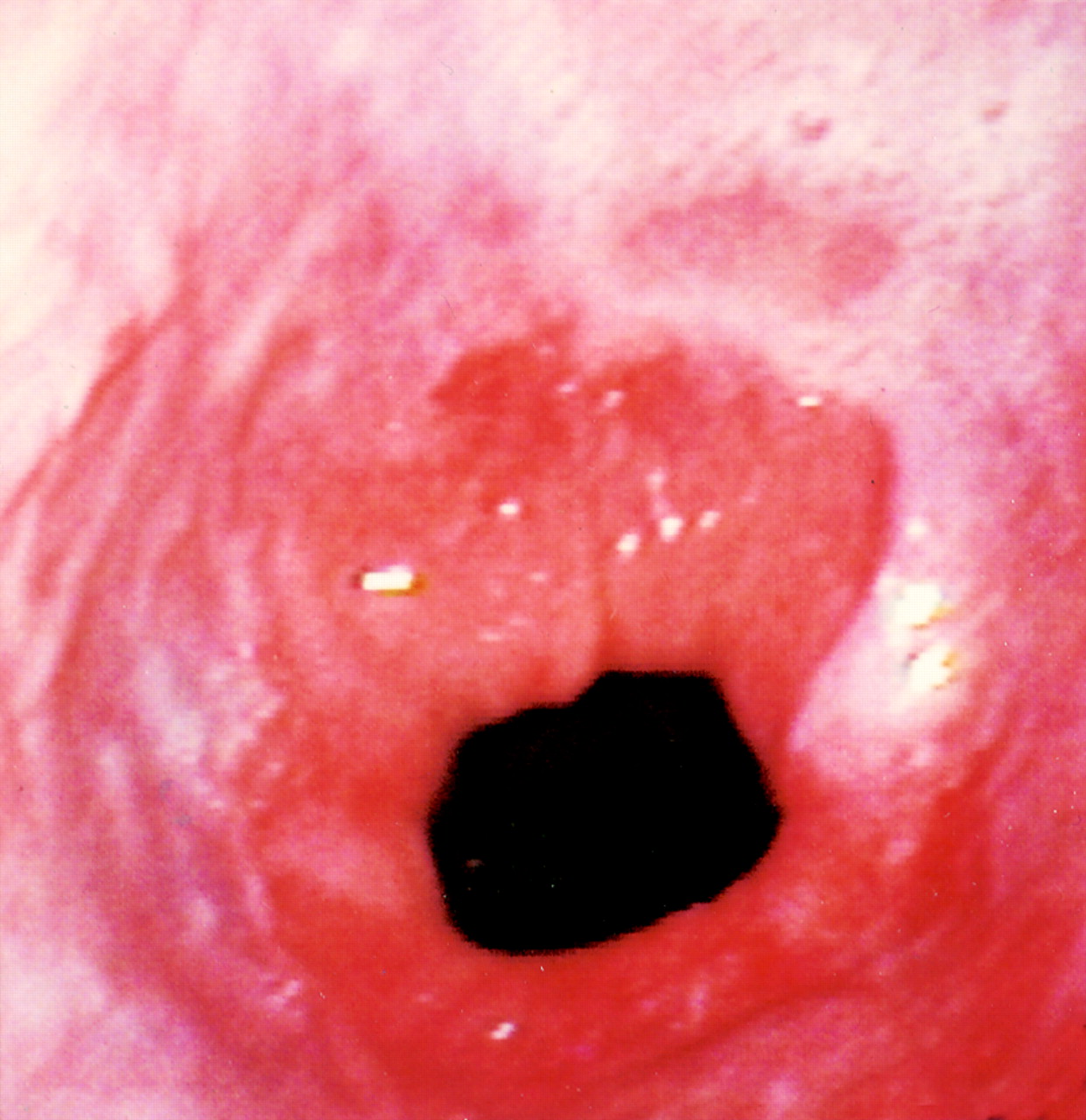
Endoscopic view of the lower part of the re-epithelialised Barrett's mucosa after four argon plasma coagulation sessions.
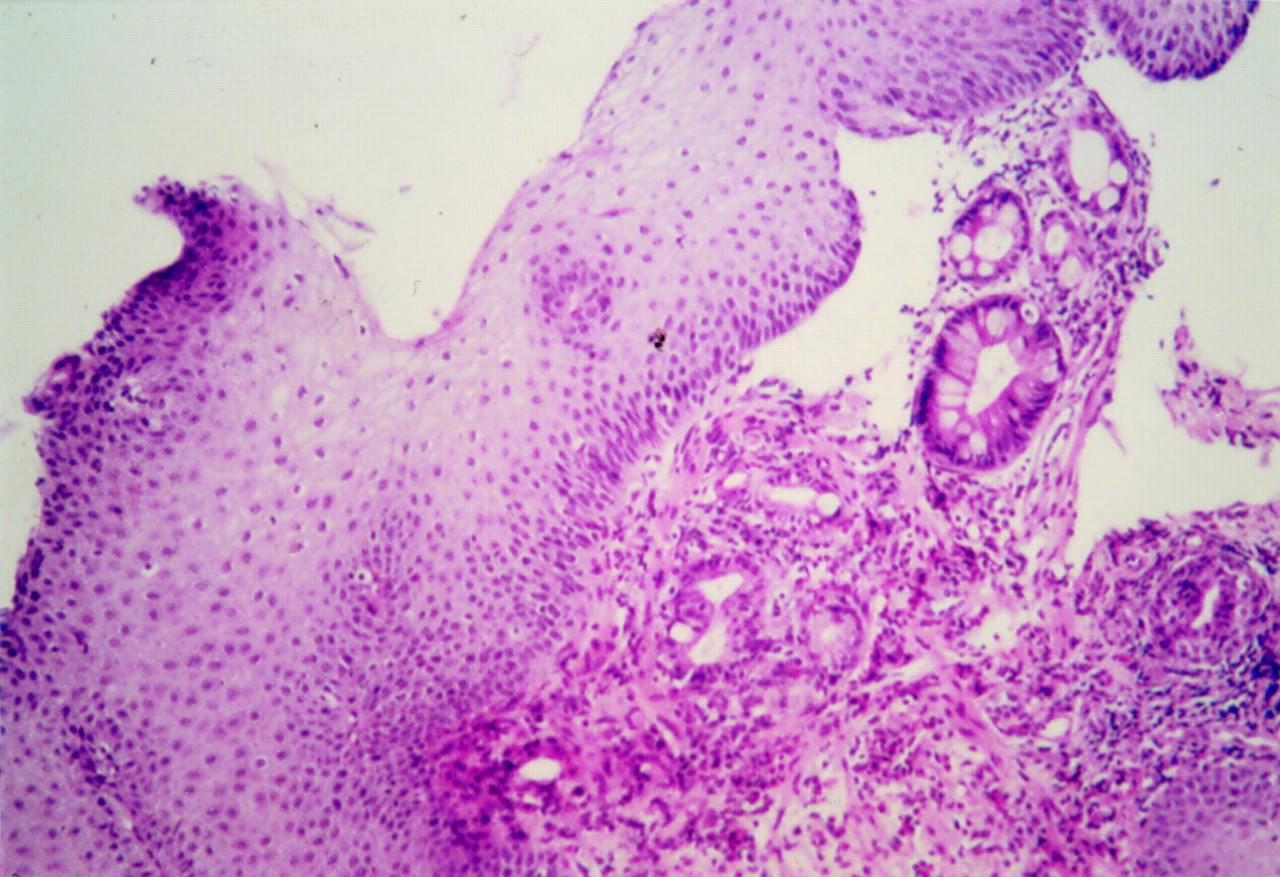
Residual metaplastic glands are found beneath the new squamous epithelium after completion of endoscopic treatment.
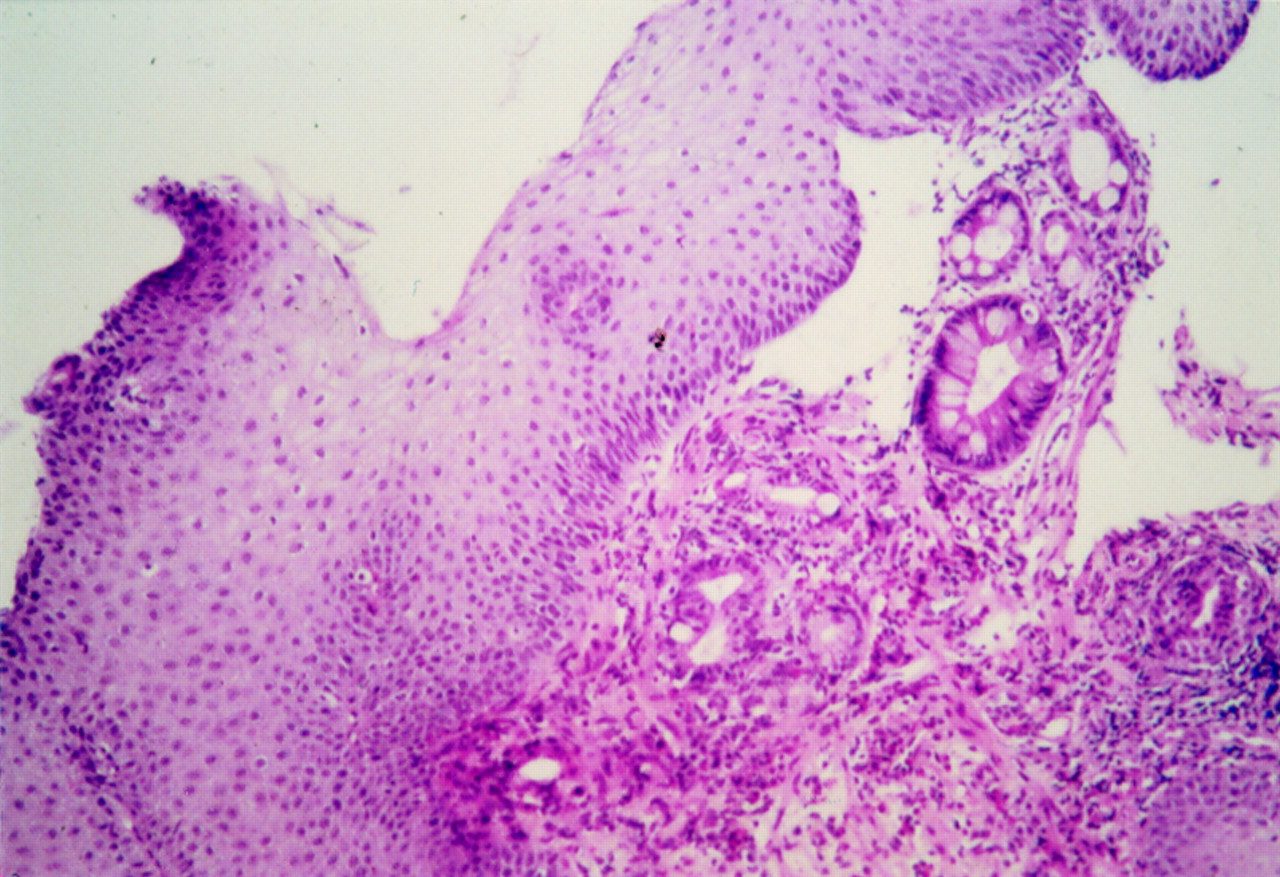
Eighteen months after the end of APC treatment, endoscopy continues to show an apparent complete re-epithelialisation over the whole length of the oesophagus. However, a bulging area (⊘ 10 mm) was observed just above the squamocolumnar junction (fig 3). Biopsy specimens, sampled using 9 Fr forceps, disclosed specialised columnar epithelium with high grade dysplasia below a very thin squamous layer (fig 4). Endoscopic untrasonography confirmed the non-invasive character of the tumour which was confined to the mucosa (TisN0).
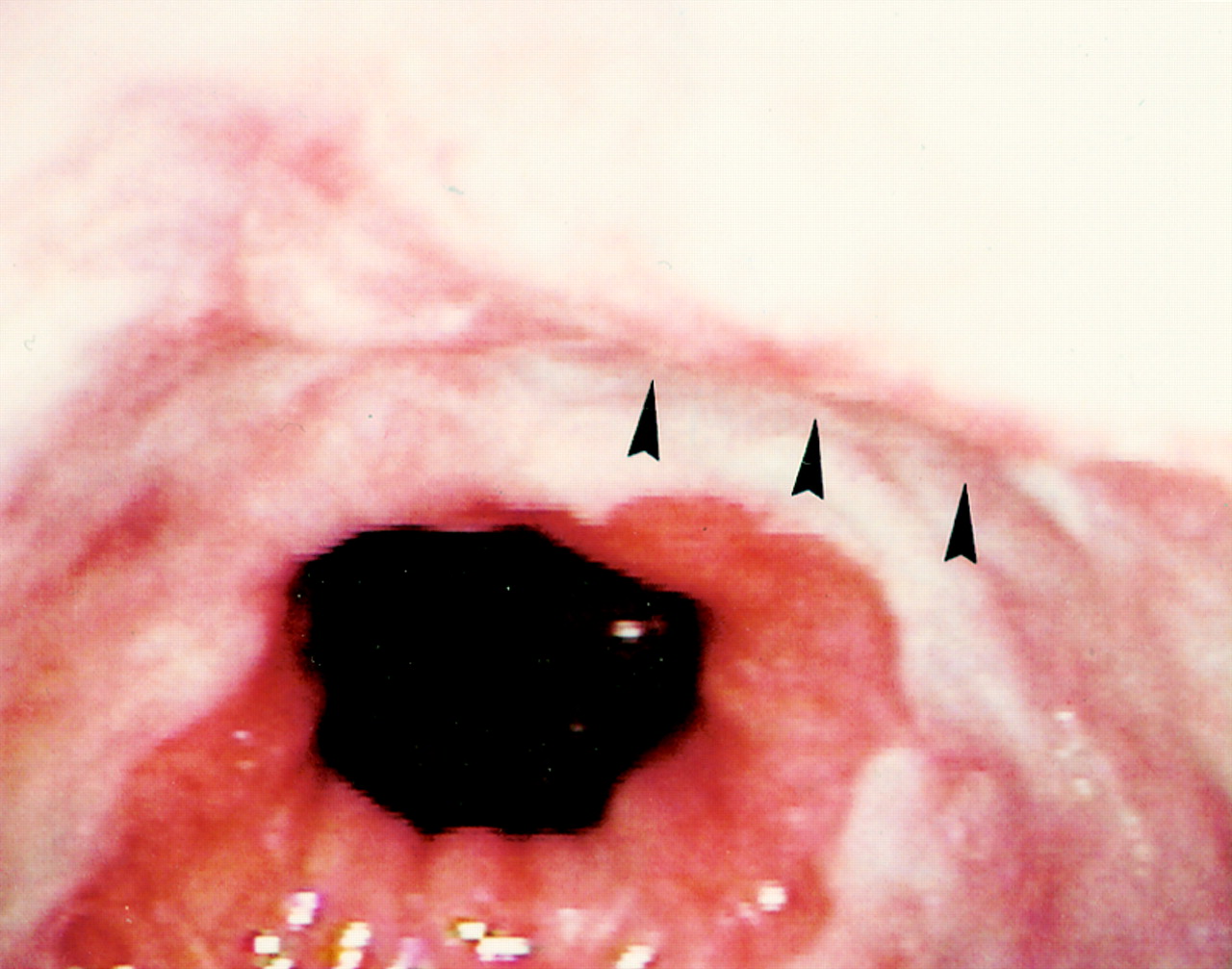
Eighteen months after complete apparent re-epithelialisation, mucosal bulging (arrowheads) was observed just above the new squamocolumnar junction.

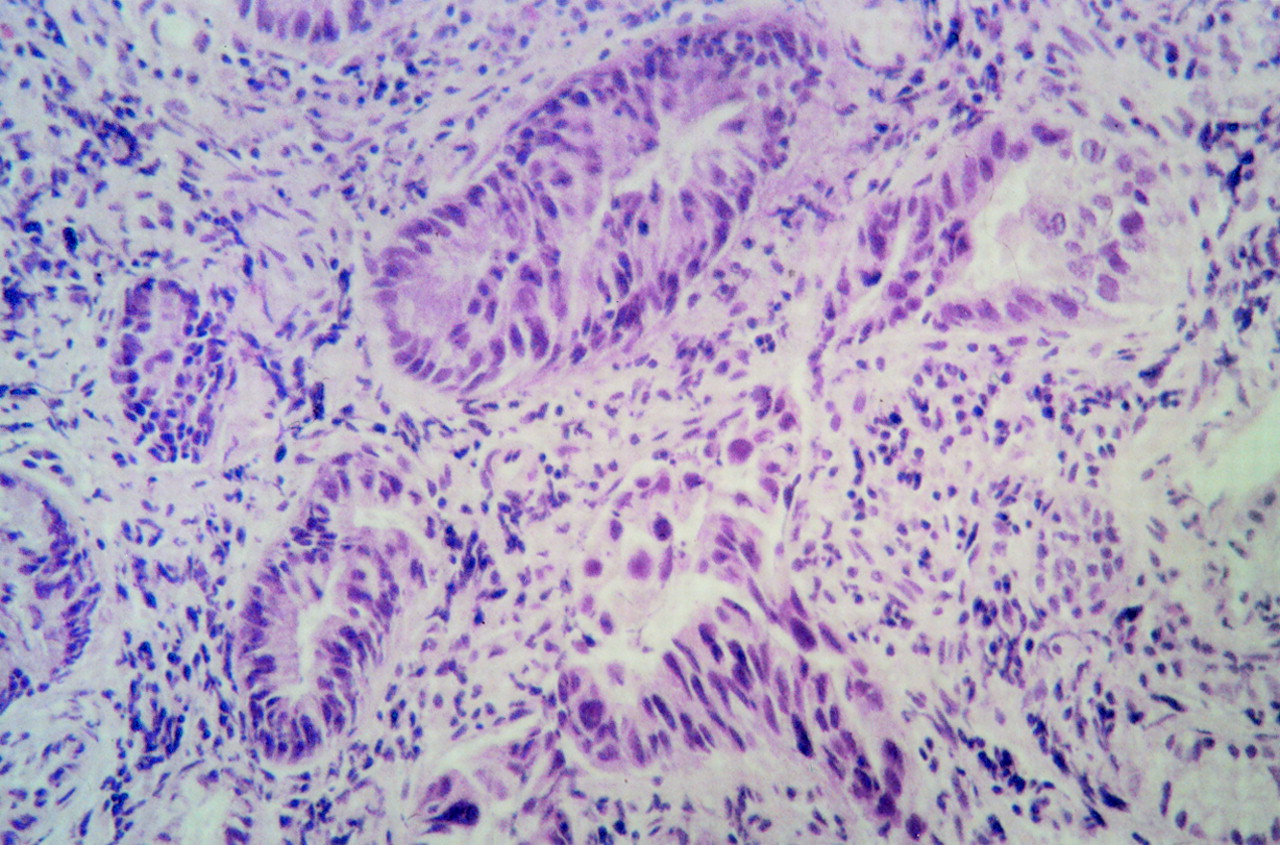
Histology showed a specialised columnar epithelium with high grade dysplasia below a thin surface squamous layer clearly attached to the dysplastic glands (arrow).
Oesophagectomy was proposed but refused by the patient. Alternatively, an endoscopic mucosectomy was successfully performed, with complete resection of the neoplastic lesion. Histological examination confirmed the presence of an intramucosal adenocarcinoma (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Part of the histological view of the mucosectomy specimen confirming the presence of an intramucosal carcinoma.
Endoscopic and histological follow up disclosed the absence of neoplasia 12 months after the mucosectomy. Serial endoscopic assessments are planned every three months for the next two years. The patient will continue to receive proton pump inhibitor therapy (omeprazole 40 mg daily).
Discussion
We have reported the first case, to our knowledge, of a Barrett's adenocarcinoma which developed 18 months after squamous re-epithelialisation of a non-dysplastic Barrett's segment and was located beneath the squamous epithelium. Although it is not possible to definitely exclude the fact that the tumour might have been present before endotherapy, the present finding could represent a important concern regarding this potential therapeutic approach of Barrett's oesophagus.
Indeed, several centres including ours, have become enthusiastic about the future potential therapeutic application of these experiments which have shown that ablating the specialised mucosa effectively leads to squamous re-epithelialisation when associated with high doses of proton pump inhibitors.5-9 This enthusiasm was probably strengthened by the increased incidence of oesophageal adenocarcinoma over the past 20 years.1 2 Therefore, if a squamous re-epithelialisation occurs and persists, this might theoretically avoid further development of dysplasia and/or cancer. Although no data are currently available for proposing this treatment on a routine basis, some potential future strategies have been advocated, consisting of thermal or photodynamic ablation followed by antireflux surgery. However, in the majority of the studies reported so far, the presence of surface squamous epithelium with underlying residual glandular cells was commonly reported whatever the technique used, notably photodynamic therapy, argon laser, and argon plasma coagulation.5-9 In our series, this residual columnar mucosa was observed in 20% of our patients with an endoscopically apparent complete eradication of Barrett's mucosa.9 The relevance of this finding remains undetermined in terms of potential malignant evolution, as long term follow up studies of these patients are not yet available and the possible development of cancer in the subsquamous Barrett's glands remains critical to the assessment of this type of therapy.
We have diagnosed the presence of an intramucosal adenocarcinoma 18 months after apparently complete squamous re-epithelialisation of an initially non-dysplastic Barrett's mucosa. A previous observation was reported by Sampliner and Fass, but in this case, the Barrett's mucosa disclosed initially high grade dysplasia. After evidence of squamous re-epithelialisation, the patient subsequently underwent oesophagectomy; histology from the resected specimen showed foci of intramucosal carcinoma with overlying squamous epithelium.10 As unanimously advocated,11 12a careful histological mapping of the Barrett's mucosa was performed before APC treatment, making less probable the possibility of missing foci of severe dysplasia, although the hypothesis of a pre-existing neoplastic lesion cannot be positively excluded. Additional multiple biopsy specimens were taken after thermal ablation and none of them have shown evidence of neoplastic glands.
The interval time of 18 months between thermal ablation and the development of intramucosal carcinoma can be considered as relatively short and one can speculate that the growth rate of neoplastic tissues in treated Barrett's mucosa might be more rapid than in non-treated Barrett's. This hypothesis might deserve further studies assessing, for example, the proliferation index of subsquamous metaplastic glands, and should enable us to gain a better knowledge on the characteristics of the new epithelium.
The endoscopic aspect of the mucosa cannot be considered for defining complete squamous re-epithelialisation as residual columnar cells are frequently found in biopsy specimens taken from areas of endoscopically apparent squamous mucosa. Our observation suggests that these residual cells still carry a continuing risk of malignant progression. This is why any experimental attempt to eradicate Barrett's oesophagus should be done with extreme caution in prospective clinical studies, with maintained regular endoscopic surveillance and multiple biopsies. Indeed, not only might the residual glands still have the potential to become dysplastic but also the squamous re-epithelialisation might hide, as in the present case, an intramucosal adenocarcinoma developing under the squamous layer. Fortunately, in the present case, it was a bulging area in the distal oesophagus which caught the endoscopist's eye and allowed an early diagnosis. This might represent an important concern for the applicability of the technique, especially in patients with non-dysplastic Barrett's at the time of treatment. This is true for any technique used for endoscopic treatment, as the persistence of residual columnar mucosa does not seem to be related to the method of ablation, similar findings having been observed with the other procedures, notably photodynamic therapy.7-13
In summary, we have reported the possible risk of developing carcinoma in patients with endoscopic squamous re-epithelialisation of Barrett's oesophagus after thermoablation. Identification of residual columnar mucosa underlying squamous epithelium is of major importance in all patients who have had Barrett's ablation and must be systematically checked despite the endoscopic appearance of complete squamous re-epithelialisation. In addition, detection of dysplastic glands, which could arise de novo or be already present before therapy, may be hampered by the overlying squamous epithelium and large biopsies should therefore be sampled along the re-epithelialisation areas. This observation suggests that, at least in patients with persistent columnar cells under the squamous layer, the risk of neoplastic progression might persist and the surveillance programme of Barrett's should be maintained in experimental protocols pertaining to ablative therapy.
References
Footnotes
- Abbreviations used in this paper:
- APC
- argon plasma coagulation