Article Text

Abstract
BACKGROUND/AIMS For pretherapeutic staging of squamous cell carcinoma of the oesophagus, endoscopic ultrasonography (EUS) is considered the most profitable modality because it can provide cross sectional imaging of the tumour. The aim of this study was to evaluate the relation between prognosis and EUS findings, especially tumour area, in squamous cell carcinoma of the oesophagus.
PATIENTS/METHODS A total of 113 patients with squamous cell carcinoma of the oesophagus underwent EUS for pretherapeutic examination at Nagoya University Hospital. We compared EUS findings, histological results, and outcome. In addition, we measured the area of the tumour on EUS images (n=113) and evaluated if EUS area correlated with volume of the tumour on histological findings (n=50).
RESULTS The overall accuracy rate of EUS was 83.2% (94/113) for depth of tumour invasion and 67.6% (69/102) for perioesophageal lymph node metastasis. The EUS area increased in proportion to the development of tumour infiltration, and patients with lymph node metastasis had a larger EUS area than patients without lymph node metastasis. There was a close correlation between EUS area and volume of the tumour on histological findings. If EUS area of the tumour was less than 50 mm2, the five year survival rate was 100%. As EUS area increased, the survival rate decreased.
CONCLUSIONS Measurement of EUS area of the tumour is reliable for quantification of the tumour and prediction of prognosis in patients with squamous cell carcinoma of the oesophagus.
- squamous cell carcinoma
- oesophagus
- endoscopic ultrasonography
- prognosis
- preoperative staging
Abbreviations used in this paper
- EUS
- endoscopic ultrasonography
- EMR
- endoscopic mucosal resection
Statistics from Altmetric.com
The prognosis of oesophageal cancer patients is poor because the majority of lesions are in the advanced stage at the time of diagnosis.1 Recently however, because of more widespread knowledge of early stage oesophageal cancer and the use of videoendoscopy with Lugol staining for high risk patients, it has been possible to detect oesophageal cancer at earlier stages.2-4 If we can detect oesophageal cancer in the mucosal stage, we can use endoscopic mucosal resection, which is effective and the minimum local treatment.5 ,6 Recently, endoscopic mucosal resection (EMR) has become widely used in Japan, and contributes to the improved quality of the patient's life after treatment.
Endoscopic ultrasonography (EUS) can provide cross sectional imaging of the gastrointestinal wall and adjacent structures7-9 and thus provide information on choice of treatment and evaluation of prognosis in oesophageal cancer. We believe that EUS is an essential part of the pretherapeutic examination for staging of oesophageal cancer. To make the most of the specific characteristics of EUS, we measured the area of the tumour on EUS images and assumed that the tumour area on the EUS image was generally in proportion to the volume of the tumour. As the relation between EUS findings and prognosis of oesophageal cancer patients is not well known, the aim of this study was to evaluate the relation between prognosis and EUS findings, especially tumour area, in squamous cell carcinoma of the oesophagus.
Materials and methods
PATIENTS
From January 1988 to December 1997, 319 patients with oesophageal cancer underwent EUS for pretherapeutic examination at the Second Department of Internal Medicine, Nagoya University Hospital. In 113 of 319 patients it was possible to compare EUS findings and histopathological results, with obvious outcome after treatment. The remaining 206 patients were excluded from the study because of chemotherapy or radiation therapy before operation, follow up in another institution, inoperable lesions, or death from another disease. A total of 113 patients (99 men, 14 women; mean age 60 years, range 42–78) underwent EMR (n=11) or surgery (n=102) for initial treatment at our institution. The observation period after treatment was 30.1 (2.2) months (mean (SEM)). All were found to have histopathologically confirmed squamous cell carcinoma.
For pretherapeutic evaluation, we examined invasion of the tumour and perioesophageal lymph node metastasis with EUS. We performed EUS using the water infusion or water filled balloon method. In all cases, EUS findings were compared with histopathological findings of resected specimens. Histopathological evaluation was based on guidelines established by the Japanese Society for Esophageal Disease.10 There were no complications in this study.
INSTRUMENTS
We used the radial sector scanners GF-UM2 (7.5 MHz), GF-UM20 (switchable 7.5 MHz and 12 MHz), and GF-UM200 (switchable 7.5 MHz and 20 MHz; Olympus Optical Co. Ltd, Tokyo, Japan), and the ultrasound probes MP-PN15–08M (15 MHz; Aloka Co. Ltd, Tokyo, Japan), UM-2R (12 MHz) and UM-3R (20 MHz; Olympus Optical Co. Ltd).
PRETHERAPEUTIC STAGING (DEPTH OF TUMOUR INVASION AND PERIOESOPHAGEAL LYMPH NODE METASTASIS) BY EUS
We performed pretherapeutic staging of oesophageal cancer by EUS. For evaluation of the depth of tumour invasion by EUS, we used diagnostic criteria based on hypoechoic tumour area and oesophageal wall structure which was destroyed by tumour infiltration. Interpretation of EUS findings of normal oesophageal wall was guided by previous reports.8 ,9 For assessment of perioesophageal lymph node metastasis, we investigated all 102 patients who underwent open surgery with perioesophageal lymph node dissection. For determination of perioesophageal lymph node metastasis by EUS, a sharply rounded node with a size greater than 1 cm in diameter and a hypoechoic internal echo was considered a positive metastatic node.11
MEASUREMENT OF AREA AND VOLUME OF THE TUMOUR
After pretherapeautic staging, the maximum area of the tumour was measured on the EUS image in which the tumour as a low echoic area appeared largest. Firstly, for fundamental examination, we evaluated if the EUS area correlated with the volume of the tumour on histological findings. We measured the area of the tumour on sequentially prepared specimens of the entire tumour which was divided into rectangular slices (45×4 mm), and calculated volume of the tumour by integration of tumour area and width (4 mm) of the prepared specimen. It was possible to compare the EUS area and the resected specimen volume in 50 cases. All 50 prepared specimens were fixed by the same method, and we considered that shrinkage of tissue occurred to the same degree in all specimens. If we could not detect the tumour as a low echoic area on the EUS image, we arbitrarily took the EUS area of the tumour as 0 mm2. Then we evaluated EUS area in relation to depth of invasion and lymph node metastasis. A practical method of measurement of EUS area and pathological tumour volume is represented in fig 1. In this study, we digitised EUS images by digital scanner and captured them with Photoshop (Adobe Systems Incorporated). We then used NIH Image (Internet, NIFTY-Serve software, ftp://zippy. nimh. nih. gov/pub/nih-image/) for measurement of the area of tumours by EUS.

Measurement of tumour area, by endoscopic ultrasonography (EUS), and pathological tumour volume. (A) Ultrasound probe image of submucosal cancer. The ultrasound probe reveals a hypoechoic mass region extensively invading into the high echoic third layer (submucosal layer). In this case, the EUS area of the tumour was 36.1 mm2. (B) Histological findings after surgery showed the tumour limited to the submucosa (haematoxylin-eosin, original magnification). Pathological tumour volume (cm3) is the total tumour area (a+b+c+d) (cm2)×width of prepared specimen (0.4 cm) In this case, the pathological tumour volume was 3.20 cm3.
SURVIVAL OF PATIENTS
We evaluated the relation between EUS findings and prognosis of oesophageal cancer patients. Firstly, we calculated survival rates according to the EUS area of the tumour. Then we calculated survival rates according to histological and EUS findings on depth of tumour invasion and perioesophageal lymph node metastasis.
STATISTICAL METHODS
Values are expressed as mean (SEM). The χ2 test was performed to investigate the difference in EUS areas according to depth of tumour invasion, and the Mann-Whitney U test was performed to investigate the difference in EUS areas between positive and negative lymph nodes. Pearson's correlation coefficient was used for evaluation of the correlation between EUS area and pathological tumour volume. Survival curves were calculated using the Kaplan-Meier method. The log rank test was performed to investigate differences between survival curves. A p value less than 0.05 was considered significant.
Results
PATIENT CHARACTERISTICS
The characteristics of patients are listed in table 1. We followed Japanese guidelines on location of the tumour and macroscopic findings.10 Mucosal cancer patients had no lymph node metastasis and 11 of 19 patients were treated with EMR. For cases of tumour invading the submucosa, 16 of 34 patients (47.1%) had lymph node metastasis and none underwent EMR. For cases of tumour invasion to the adventitia or adjacent structures, 30 of 42 patients (71.4%) had lymph node metastasis.
Patient characteristics
EVALUATION OF DEPTH OF TUMOUR INVASION BY EUS
For evaluation of depth of tumour invasion, we compared EUS findings with histological findings. The results of EUS assessment of the depth of tumour invasion are summarised in table 2. The accuracy rate for depth of tumour invasion was 89.5% for mucosal cancer, 76.5% for submucosal cancer, 55.6% for tumours invaded to the muscularis propria, and 97.6% for tumours invaded to the adventitia or adjacent structures. The overall accuracy rate was 83.2% (94/113). Positive and negative predictive values are given in table 2.
Comparison between pretherapeutic EUS findings and pathological diagnosis on depth of tumor invasion
ASSESSMENT OF PERIOESOPHAGEAL LYMPH NODE METASTASIS BY EUS
For diagnosis of perioesophageal lymph node metastasis, we compared EUS findings with histological findings in all 102 patients who underwent open surgery with perioesophageal lymph node dissection. The results of EUS assessment of lymph node metastasis are summarised in table 3. The sensitivity of the EUS diagnosis for lymph node metastasis was 75.9% (41/54) and specificity was 58.3% (28/48). The overall accuracy rate was 67.6% (69/102).
Comparison between pretherapeutic EUS findings and pathological diagnosis on perioesophageal lymph node metastasis
AREA AND VOLUME OF THE TUMOUR
We investigated the relation between EUS area and volume of the tumour calculated from the sequentially prepared specimens. The results of the correlation between EUS area and pathological volume of the tumour are displayed in fig 2. There was a close correlation between the two groups. The results of EUS area of the tumour according to depth of invasion and lymph node metastasis are shown in table 4. EUS area increased in proportion to progression of tumour infiltration. Patients with lymph node metastasis had a significantly larger area than patients without lymph node metastasis (p<0.001).

Correlation between area, measured by endoscopic ultrasonography (EUS), and pathological volume of the tumour. There was a high correlation between EUS area and pathological tumour volume. Pearson's correlation coefficient was 0.92.
EUS area of the tumour according to depth of tumour invasion and perioesophageal lymph node metastasis
SURVIVAL OF PATIENTS
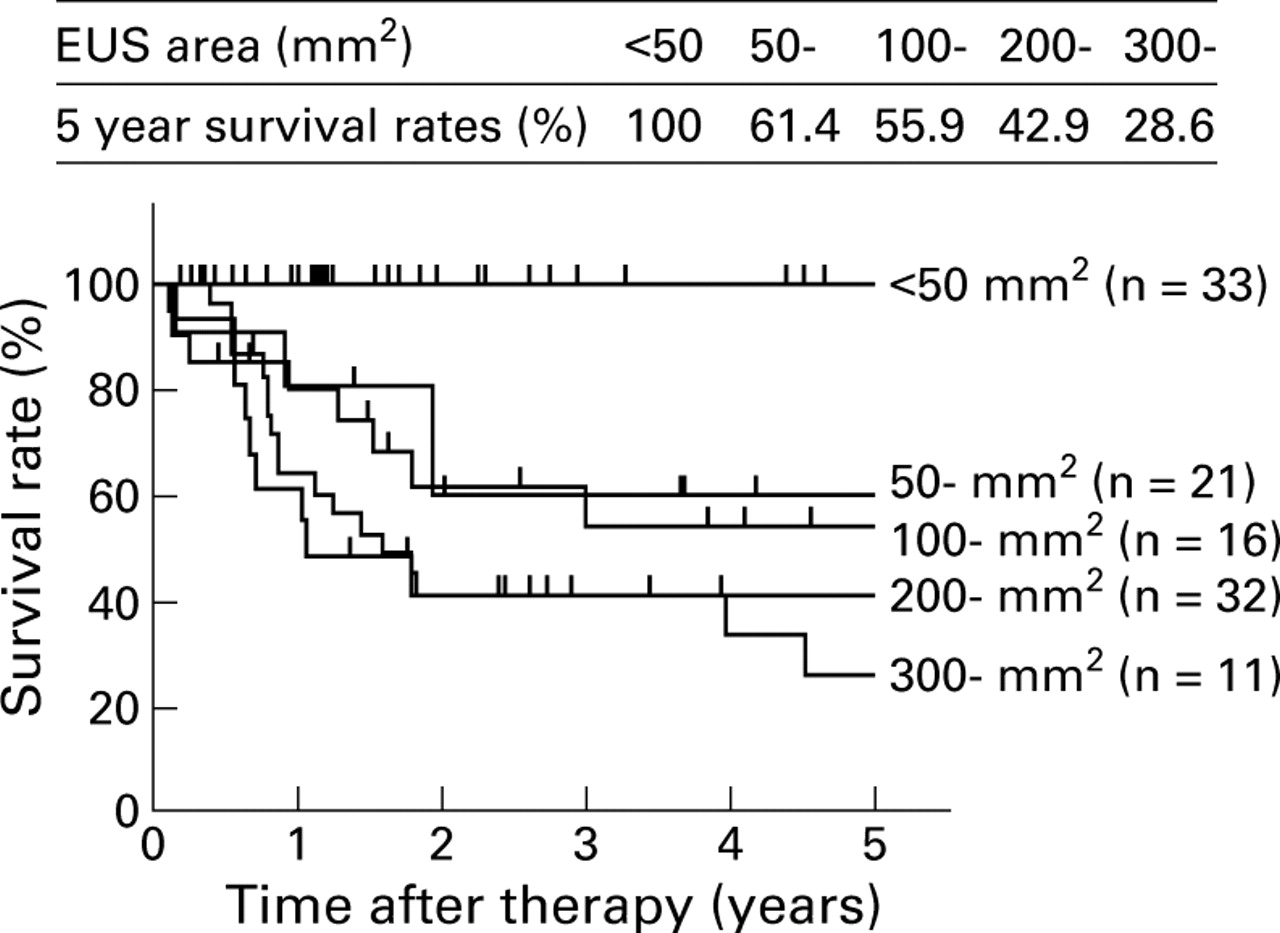
The relation between patient survival and EUS area is displayed in fig 3. When the EUS area of the tumour was smaller than 50 mm2, the five year survival rate was 100%. As EUS area increased, the survival rate decreased. The prognosis of patients with an EUS area of more than 300 mm2 was very poor (five year survival rate 28.6%). Figure 4 shows the survival of patients with oesophageal cancer related to depth of tumour invasion. In patients with mucosal cancer diagnosed by EUS or pathological findings, the five year survival rate was 100%. With greater tumour infiltration, the survival rate decreased. Figure 5 shows survival of patients with oesophageal cancer related to perioesophageal lymph node metastasis. The survival rate of patients with lymph node metastasis was lower than that of patients without lymph node metastasis. There was a significant difference between the two groups.

Kaplan-Meier survival curves for patients with oesophageal cancer, according to area, measured by endoscopic ultrasonography (EUS), of the tumour. Five year survival rates of all patients with a tumour area less than 50 mm2 on EUS findings was 100%.

Kaplan-Meier survival curves for patients with oesophageal cancer according to depth of tumour invasion. (A) Survival curves according to histological diagnosis. (B) Survival curves according to endoscopic ultrasonography (EUS) findings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves for patients with oesophageal cancer according to perioesophageal lymph node metastasis. (A) Survival curves according to histological diagnosis. (B) Survival curves according to endoscopic ultrasonography (EUS) findings. There was a significant difference between positive and negative lymph node metastasis ((A) p<0.001, (B) p=0.0021).
Discussion
The prognosis of oesophageal cancer is poorer than that of other gastrointestinal cancers although many early stage oesophageal cancers have been detected recently owing to advances in diagnostic techniques.12 ,13 In our study, the five year survival rate of all patients was 54.5% although inoperable patients were excluded from the study. If advanced oesophageal cancer patients are operable, they undergo oesophagectomy with two or three field lymph node dissection.12 ,13 Inoperable patients undergo various therapies such as chemotherapy, radiation therapy, laser therapy, or stenting for the purpose of palliation. At present, great efforts in the diagnosis and treatment of oesophageal cancer are being made towards improving the patient's quality of life.
For predicting the prognosis of oesophageal cancer patients, depth of tumour invasion and lymph node metastasis are the most important features.6 ,14 ,15 Therefore, until now, we have made efforts to diagnose accurately these two areas. Based on our present data, when the tumour invaded the adventitia or adjacent structures, the five year survival rate was 26.1%, and when lymph node metastasis was positive it was 30.9%. In contrast, in patients with mucosal cancer, the five year survival rate was 100%, and 11 of 19 cases (57.9%) were treated with EMR. Therefore, accurate pretherapeutic staging is one of the most crucial points for prediction of prognosis and appropriate selection of treatment.
EUS is the most reliable method for local staging of oesophageal cancer. In evaluating the depth of tumour invasion, lymph node metastasis, and relation to adjacent structures, EUS is more accurate than computed tomography.8 ,16 ,17 In this study, the accuracy rates for EUS were 83.2% for diagnosis of depth of tumour invasion and 67.6% for evaluation of perioesophageal lymph node metastasis.
To date, we have performed staging of oesophageal cancer by tumour depth and lymph node metastasis. In this study, we concentrated on the ability of EUS to directly visualise the tumour on cross sectional images. Oesophageal cancer is not greatly affected by peptic ulcerative change as is gastric cancer and thus we were able to determine the oesophageal cancer tumour volume by EUS measurement of tumour area. Strictly speaking, the EUS area of the tumour is not equal to the area of the resected specimen, as in Japan EUS findings are shown as cross sectional images and histopathological findings give a longitudinal sectional picture.10 For evaluation of gastric ulcer healing, we have previously proved that EUS images of resected ulcer specimens are equivalent to histological photographs. With respect to tumour area of the resected specimen, the expected contraction for specimens embedded in paraffin was 92% of the original area, and we could calculate a rough estimate of tumour volume by integration of tumour area and width of the prepared specimen.18 There have been few reports on EUS area of tumours until now, and even fewer reports that investigated the relation between EUS findings and prognosis of patients with oesophageal cancer. Isenberg et al reported that standard EUS staging is not accurate after neoadjuvant chemoradiation, and that measurement of maximal cross sectional area of the tumour is useful for assessing response of oesophageal cancer to preoperative chemoradiation.19 In patients who have undergone preoperative chemoradiation, evaluation of depth of tumour invasion is difficult because of inflammation or fibrosis in the oesophageal wall. Thus in our study, patients treated with preoperative chemoradiation were excluded. For EUS assessment of response to chemoradiation, further studies are needed. In another report, Bruggeet al found that EUS measurement of the maximal thickness of a malignant oesophageal mass can accurately predict extraoesophageal extension.20 In this way, EUS measurement of length and area of the tumour is very useful for assessment of diagnosis and treatment.
In the present study there was a close correlation between EUS area and volume based on histopathological findings. Measurement of EUS tumour area can be performed simply using existing EUS systems, and as EUS measurement of tumour area correlates closely with tumour volume on histopathological findings, it can substitute for tumour volume. From our results, prognosis of patients with an EUS area less than 50 mm2 was excellent but became worse with an increase in EUS area, indicating that tumour volume correlates with prognosis of patients with oesophageal cancer. We believe that this new method is simple and reliable for assessment of oesophageal cancer.
Erroneous diagnosis of depth of tumour invasion was caused by an undetectably small quantity of tumour invasion or inflammatory change in the submucosa. In our study, underdiagnosis of depth of tumour invasion was principally caused by a small quantity of tumour invasion into the submucosa. With the present level of EUS technology, we can diagnose cancer massively invading the submucosa but it is very difficult to detect minimal invasion of the submucosa. This change was extremely minute, and we do not believe it had a significant effect on measurement of EUS area of the tumour. Regarding evaluation of lymph node metastasis, specificity was low (58.3%) because our diagnostic criteria are still insufficient. However, EUS area of the tumour in patients with positive lymph node metastasis was significantly larger than in patients with negative lymph node metastasis. Measurement of EUS area of the tumour might contribute to a diagnosis of lymph node metastasis.
Recently, three dimensional EUS was developed to visualise surface and internal structures of the tumour and its relation with adjacent structures; it is also applicable in the diagnosis of gastrointestinal tumours21 and can measure tumour volume. This system holds mind boggling possibilities but has not yet become widely used because of its high cost. We believe this technology can be used for diagnosis and judgment of treatment of oesophageal cancer in the future.
In conclusion, EUS and quantification of the EUS image are the most reliable modalities for preoperative staging and prediction of prognosis in oesophageal cancer because they provide an abundance of information on the depth of invasion, lymph node metastasis, tumour area, and volume.
Abbreviations used in this paper
- EUS
- endoscopic ultrasonography
- EMR
- endoscopic mucosal resection