Article Text

Abstract
BACKGROUND Patients with liver cirrhosis are at significant risk of hepatocellular carcinoma (HCC) that may develop as well defined nodular lesions or as more aggressive infiltrating tumours.
AIM To compare prospectively risk factors associated with nodular or infiltrating HCC in cirrhotic patients.
PATIENTS AND METHODS We studied 370 patients with cirrhosis, followed prospectively by periodic ultrasound (US) of the liver, for a mean period of 74.6 (SD 32.4) months to define the incidence and patterns of HCC development. Patients who developed HCC were compared according to tumour pattern using univariate and multivariate analysis.
RESULTS Sixty one (16.5%) patients developed HCC: HCC was classified as nodular in 49 (80.3%) and infiltrating in 12 (19.7%) according to US and computerised tomography (CT) imaging. The five and 10 year cumulative probabilities were 8.1% (95% confidence interval (CI) 5.2%-11%) and 25.2% (15.0–35.4%) for nodular HCC and 2.1% (0.5–3.7%) and 6.9% (2.1–11.7%) for infiltrating HCC. Patients with infiltrating HCC were younger than those with nodular HCC (59.5 v66.2 years, 95% CI 55.2–63.8 and 64.1–68.3 years; p=0.014). Using multivariate analysis, development of nodular HCC was associated with older age (p=0.0002; relative risk (RR) 3.1; 95% CI 1.6–5.2), longer duration (p=0.09; RR 2.6; 95% CI 1.8–3.4), and more advanced stage (p=0.002; RR 2.5; 95% CI 1.3–4.5) of cirrhosis but not with the aetiology of liver disease. In contrast, development of infiltrating HCC appeared to be unrelated to age or disease duration or stage, while it was associated with hepatitis B virus infection (p=0.07; RR 3.96; 95% CI 1.1–5.2) and with hepatitis B/hepatitis C virus coinfection (p=0.0007; RR 16.9; 95% CI 3.8–36.7).
CONCLUSIONS In liver cirrhosis, we identified two patterns of HCC developing with distinct risk factors. Nodular HCC was related to the cirrhotic process per se independent of aetiological factors and may depend on the proliferative activity within regenerative nodules, while the infiltrating form of HCC was linked to hepatitis B virus infection and may reflect more direct virus induced carcinogenesis.
- hepatocellular carcinoma
- cirrhosis
- hepatitis B virus
- hepatitis C virus
Abbreviations used in this paper
- AFP
- α fetoprotein
- ALT
- alanine aminotransferase
- CT
- computerised tomography
- HBsAg
- hepatitis B surface antigen
- HBV
- hepatitis B virus
- HCC
- hepatocellular carcinoma
- HCV
- hepatitis C virus
- RR
- relative risk
- US
- ultrasound
Statistics from Altmetric.com
Patients with cirrhosis of the liver are at significant risk of developing hepatocellular carcinoma (HCC).1 Prospective surveillance studies, conducted in different parts of the world, indicate an annual incidence of HCC of 1–6% in patients with cirrhosis of different aetiologies.2-10 These prospective studies have identified two main patterns of tumour development that can be distinguished by imaging techniques. Most patients present initially with single or, more rarely, multiple expanding encapsulated nodules while a minority show a more aggressive infiltrating form of HCC.3 ,8 ,10-15 Nodular HCC has a relatively slow pattern of growth and is usually treated by resection or loco-regional interventions while the infiltrating form of HCC is often unsuitable for any type of intervention. Although several studies have investigated risk factors associated with the development of HCC in patients with cirrhosis, no information is available on whether the pattern of tumour development and growth reflects different aetiopathogenetic mechanisms. In a prospective surveillance programme conducted in 370 patients with liver cirrhosis, we have assessed the probability of developing a nodular or infiltrating form of HCC and compared risk factors associated with these distinct types of HCC.
Patients and methods
PATIENTS
The patients analysed in this study were those included in a prospective follow up surveillance programme of compensated liver cirrhosis which was initiated in our unit in 1986. The criteria for inclusion in this programme were: (1) a diagnosis of liver cirrhosis, classified as stage A or B according to the Child-Pugh scoring system16; and (2) absence of clinical and ultrasonographic evidence of liver cancer and α fetoprotein (AFP) levels <200 ng/ml. A total of 370 consecutive cirrhotics were enrolled between 1986 and 1995; 231 (62.4%) were males and 139 (37.6%) were females, with a mean age at inclusion of 57.7 years (SD 9.2; range 24–81). The diagnosis of cirrhosis had been made by liver biopsy in 328 cases (88.6%) while in 42 (11.4%) who had contraindications to liver biopsy it was based on other criteria (portal hypertension associated with chronic liver disease). The stage of cirrhosis at inclusion was Child-Pugh stage A in 309 (83.5%) and stage B in 61 (16.5%). Two hundred and fifty two patients (68.1%) were anti-hepatitis C virus (HCV) positive, 50 (13.5%) were hepatitis B surface antigen (HBsAg) positive, and 17 (4.6%) were both HBsAg and anti-HCV positive. Of the remaining cases, 31 (8.4%) had alcoholic cirrhosis, eight (2.2%) primary biliary cirrhosis, five (1.3%) autoimmune, and seven (1.9%) a cryptogenic disease. The surveillance programme was aimed at monitoring the natural course of liver cirrhosis, to define the incidence of different complications, and to assess long term outcome. For these purposes, after inclusion all patients were seen at six month intervals for clinical and laboratory evaluation.6 At the same times, all patients also underwent periodic ultrasound examination (US) of the liver, aimed at early detection of HCC. Abdominal ultrasound was performed using a high resolution real time instrument (AUC 940, Ansaldo, Hitachi Medica Corporation, Tokyo, Japan) with a 3.5 MHz convex transducer. Computerised tomography (CT) was also performed to confirm the pattern and stage of HCC initially detected by US.
DIAGNOSIS AND MACROSCOPIC PATTERN OF HCC
All newly discovered focal lesions detected by US during follow up were evaluated by US assisted fine needle biopsy using a 22 gauge needle (Ecojekt, modified Chiba needle, Hospital Service, Hakko Shoji, Japan). Microbiopsy specimens were fixed in 10% formalin and stained with haematoxylin and eosin. The histological diagnosis of HCC was established according to internationally accepted criteria.17 All patients with a histological diagnosis of HCC underwent HCC staging by CT. The macroscopic pattern of HCC was defined as nodular (single or multiple nodules with a well defined margin and expansive/compressive growth) or infiltrating (not clearly defined mass with indistinct margins and infiltrating growth) according to US and CT findings.
SEROLOGICAL TESTING
Anti-HCV was determined by a second generation enzyme linked immunosorbent assay (Ortho Diagnostic System, Raritan, New Jersey, USA) and by a second generation recombinant immunoblotting assay (Chiron Corporation, Emeryville, California, USA). HBsAg was detected using commercially available kits (Abbott Diagnostics, North Chicago, Ilinois, USA).
STATISTICAL ANALYSIS
Kaplan-Meier's product limit survival analysis was performed to evaluate the cumulative probability of developing nodular or infiltrating HCC. Univariate analysis by the Student'st test and Pearson's χ2 test (or the Fisher exact test when appropriate), with 95% confidence intervals (CI), were used to compare age, duration, and stage of cirrhosis at tumour diagnosis, as well as levels of alanine aminotransferase (ALT) and AFP during follow up, and aetiological factors of liver disease in relation to the pattern of HCC. Univariate analysis by Kaplan-Meier's product limit survival and the Mantel-Cox log rank test was used to compare the cumulative probability of developing nodular or infiltrating HCC in different clinical and aetiological strata; continuous variables (age and duration of cirrhosis) were categorised using median values (age, duration of cirrhosis). Multivariate analysis by Cox's proportional hazards regression model was used to estimate the risk (with 95% CI) of developing nodular or infiltrating HCC in relation to age, sex, duration and stage of cirrhosis, ALT, and AFP levels during follow up, and aetiology of liver disease, and p values were calculated using the Wald test after determining the proportional assumption and lack of high correlation between coefficients. ALT and AFP profiles during follow up were considered categorical variables and classified as follows: (1) normal, when ALT and AFP values remained normal or 1.5 times above the upper normal limit and above 20 ng/ml, respectively, during the whole follow up period; or (2) high or fluctuating, when ALT and AFP levels were persistently high or showed continuous fluctuations during the whole follow up period. The same cut off values used for univariate analysis were applied to categorised continuous variables in Cox's regression. The Kaplan-Meier product limit survival analysis and the log rank test were used to compare the cumulative proportion of surviving patients with nodular and infiltrating HCC, independent of treatment options. All statistical tests were two sided, and the type 1 error probability was set to 0.05 for univariate analysis and 0.1 for multivariate analysis. Data analysis was performed using the BMDP statistical package.18
Results
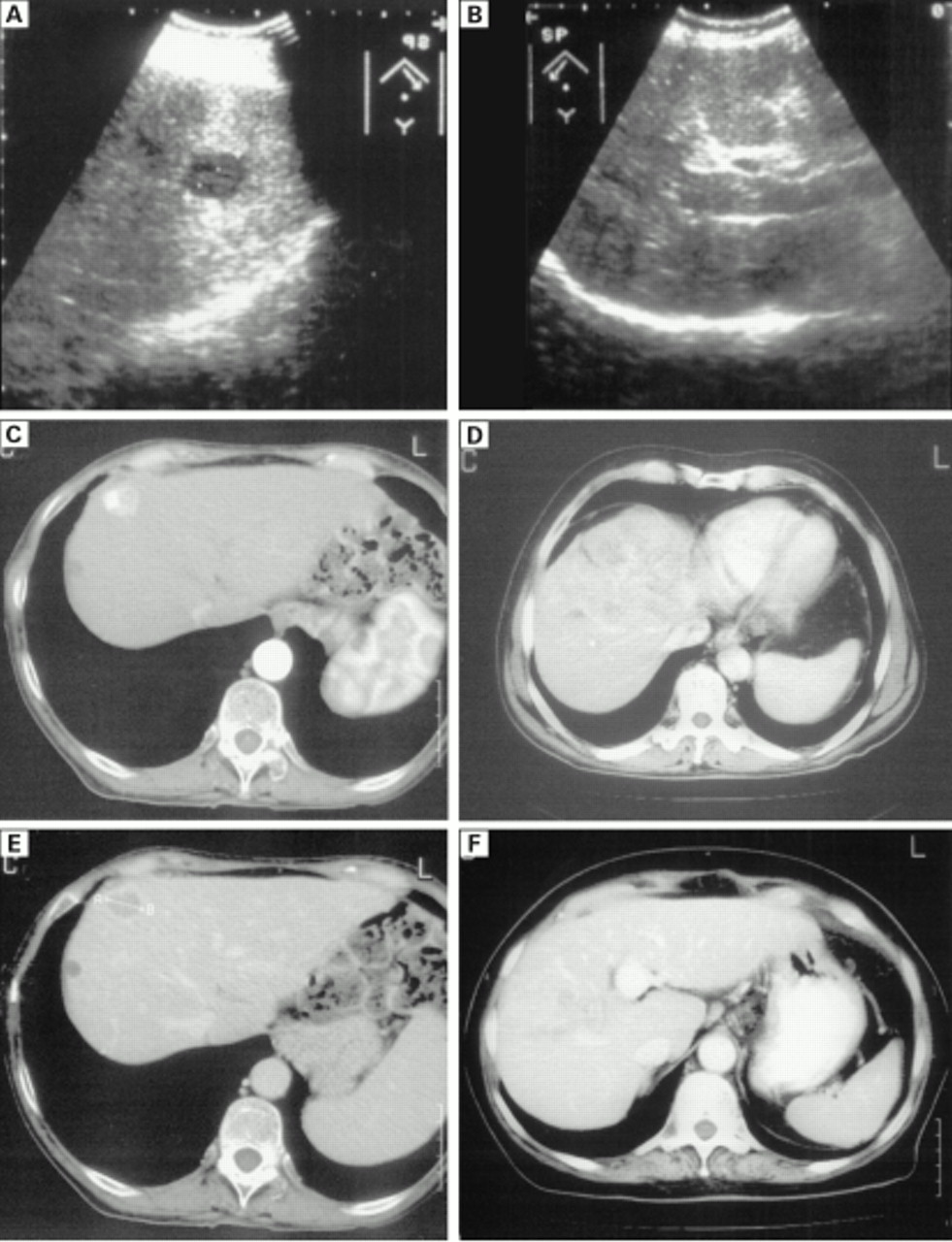
Over a mean follow up period of 74 (SD 32) months (range 24–159), 61 of 370 patients (16.5%) developed HCC. The tumour was classified as nodular in 49 (80.3%) patients, 39 cases having a single nodule and 10 cases having two nodules. At first detection the mean diameter of these nodules was 26.6 (SD 9.3) mm (range 10–50). The remaining 12 (19.7%) patients developed an infiltrating tumour. Characterisation of the morphological pattern of the tumour was obtained in all cases on the basis of US or CT findings (tumour margin, presence or absence of perinodular capsule) (fig 1).19-21 Three patients negative for focal lesions of the liver by US were found to have an infiltrating HCC by CT. None of the patients showed coexistence of nodular and infiltrating HCC at first detection, although in three cases tumour progressed from a nodular to an infiltrating type during the subsequent follow up, after loco-regional therapy. Patients with nodular HCC had a mean age at the time of tumour development that was significantly higher than that of patients with infiltrating HCC (66.2v 59.5 years; 95% CI 55.2–63.8 and 64.1–68.3 years; p=0.014) while there were no significant differences between the two groups for sex, known duration of chronic liver disease, or stage of cirrhosis. However, nodular and infiltrating HCC had a significantly different distribution in the various aetiological groups. In contrast, high or fluctuating levels of ALT during follow up were observed significantly more frequently in nodular than in infiltrating HCC (p=0.02) while there were no significant difference in AFP levels (table 1).

Nodular hepatocellular carcinoma (HCC) type (A, C, E) and infiltrating HCC type (B, D, F) by ultrasonography (A, B) and computed tomography (C–F).
Comparison of different clinical and aetiological parameters in patients with nodular and infiltrating hepatocellular carcinoma (HCC)
CUMULATIVE INCIDENCE OF NODULAR AND INFILTRATING HCC DURING FOLLOW UP
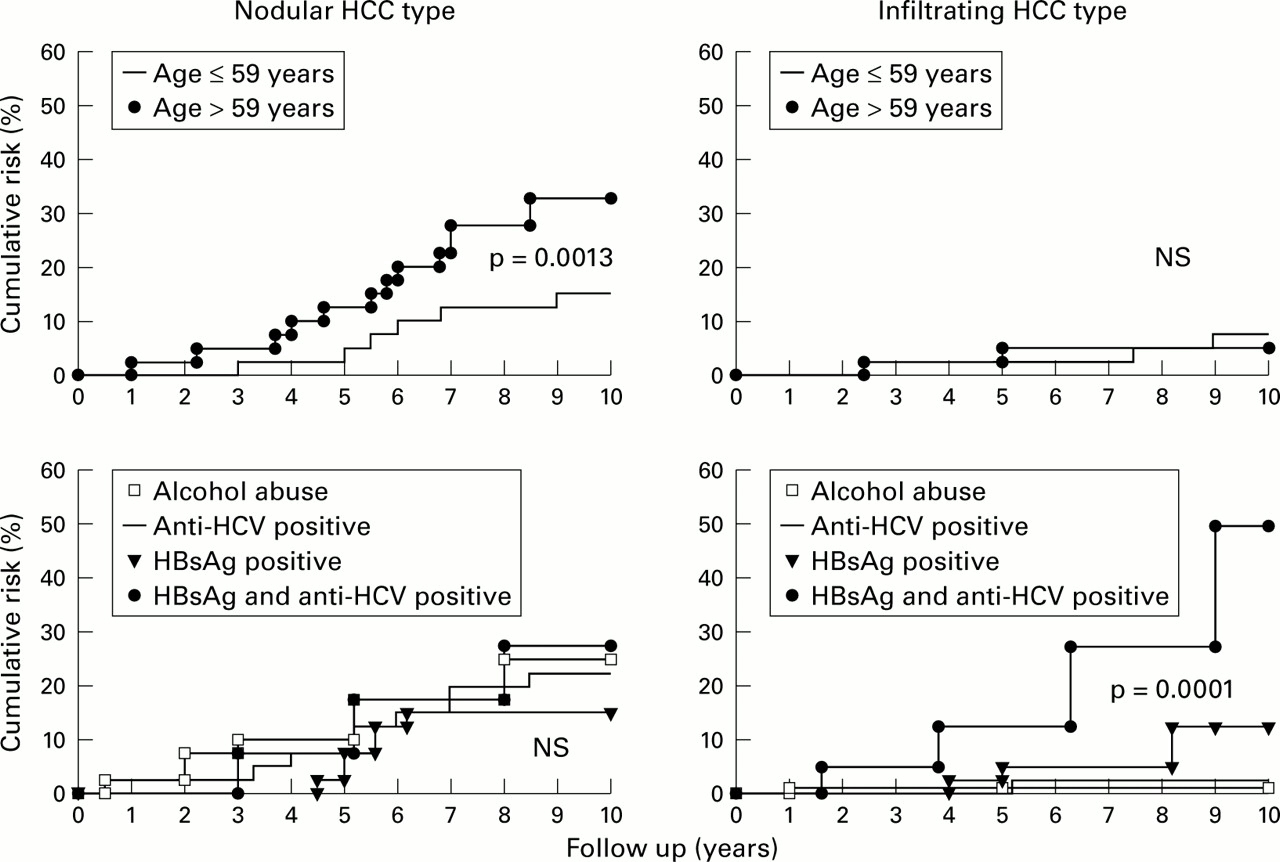
The five and 10 year cumulative probabilities of tumour development were 8.1% (95% CI 5.2–11.0%) and 25.2% (95% CI 15.0–35.4%) for nodular HCC, and 2.1% (95% CI 0.5–3.7%) and 6.9% (95% CI 2.1–11.7%) for infiltrating HCC (fig 2). On univariate analysis (Kaplan-Meier method and log rank test), the cumulative probability of development of nodular HCC was significantly higher in patients older than 59 years of age (p=0.0013), with a longer duration (p=0.019) and more advanced stage (p=0.0001) of cirrhosis at inclusion, and with high or fluctuating levels of ALT (p=0.0031) and AFP (p=0.0029) during follow up, while no difference was observed in relation to sex or aetiology of liver disease. In contrast, the cumulative incidence of infiltrating HCC was significantly higher in patients with hepatitis B virus (HBV) infection and/or with HBV/HCV coinfection (p=0.0001) while it was not influenced by age or sex, liver disease duration or stage, or ALT or AFP profiles. The cumulative risk of nodular and infiltrating HCC in relation to age and aetiology is described in fig 3.
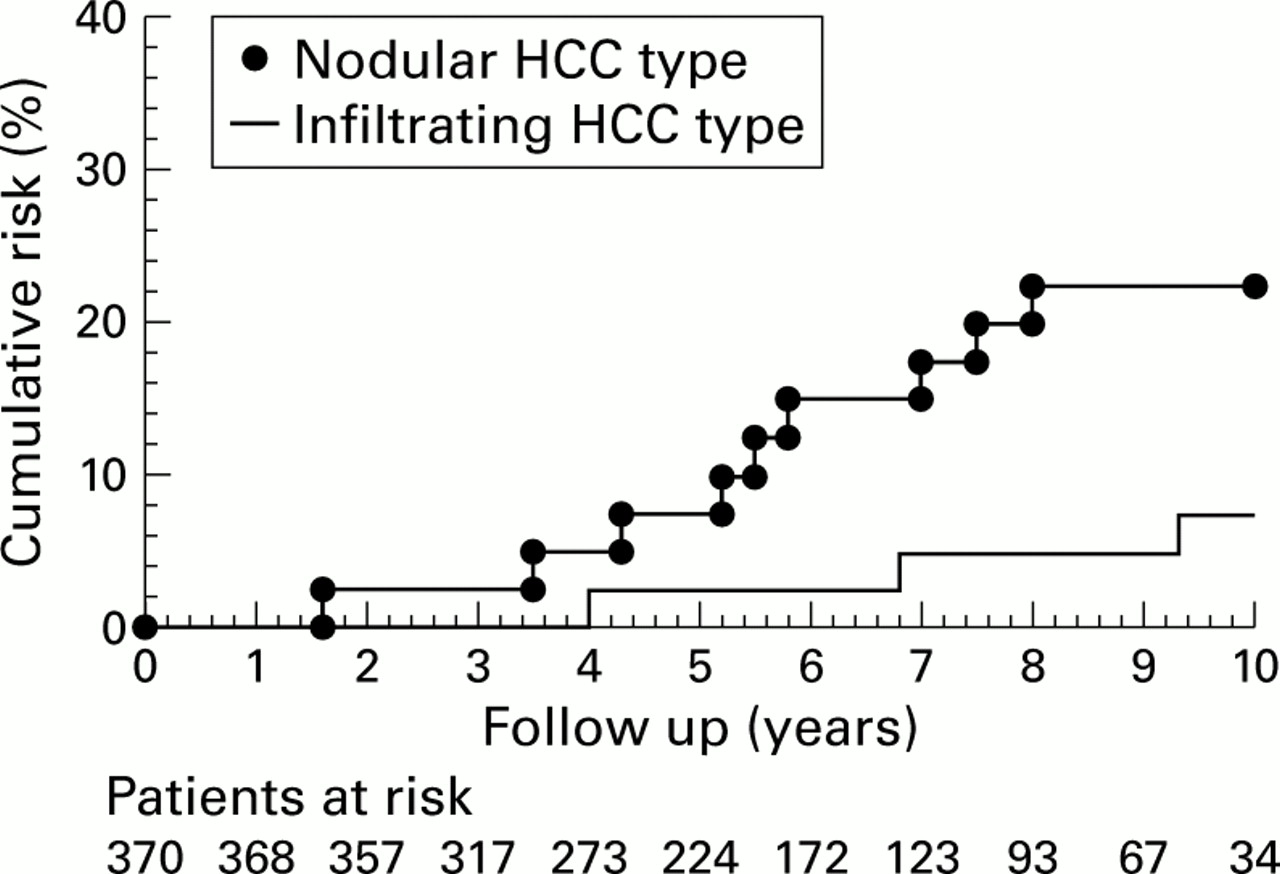
Cumulative probability of developing nodular or infiltrating hepatocellular carcinoma (HCC) in 370 patients with cirrhosis (Kaplan-Meier method).
{kind=link}
{kind=link}
{kind=link}
Cumulative probability of developing nodular (left) or infiltrating (right) hepatocellular carcinoma (HCC) in relation to age and aetiology of cirrhosis (Kaplan-Meier method and log rank test).
MULTIVARIATE ANALYSIS OF RISK FACTORS FOR DEVELOPMENT OF NODULAR AND INFILTRATING HCC
Independent risk factors for nodular and infiltrating HCC identified by multivariate analysis are described in table 2. Older age, longer duration, and more advanced stage of cirrhosis were significantly associated with increased risk of developing a nodular but not an infiltrating type of HCC. In contrast, HBV infection as well as combined HBV and HCV infection were significantly and independently associated with the development of the infiltrating but not the nodular type of HCC. Thus while development of nodular HCC was associated with disease stage and duration, independent of its aetiology, HBV infection was the main risk factor for infiltrating HCC, independent of disease stage or duration. HBsAg positive patients showed a four times higher risk for this type of tumour and the risk increased further to 17 times in the presence of HCV coinfection.
Risk factors for nodular and infiltrating hepatocellular carcinoma (HCC) in 370 patients with cirrhosis by Cox proportional hazards regression analysis and the Wald test
HISTOLOGICAL FINDINGS IN RELATION TO MORPHOLOGICAL PATTERN OF TUMOUR
No significant correlation was observed between microscopic histological findings, including both structure and differentiation of neoplastic tissue, and morphological pattern of HCC. In particular, a poor differentiated HCC was observed in 12.2% of nodular HCC and in 16.6% of infiltrative HCC.
OUTCOME OF PATIENTS IN RELATION TO PATTERN OF HCC APPEARANCE
After HCC was diagnosed, 38 patients (35 with nodular and three with infiltrating type) were treated (19 by percutaneous ethanol injection, 14 by transarterial chemioembolisation, four by resection, one by liver transplant) while 23 did not receive any specific treatment (11 refused therapy, nine had large tumours, three had clinical contraindications). The cumulative probabilities of survival at one and three years after tumour development were 75.4% and 46.0% (95% CI 62.2–88.6% and 27.4–64.4%) in patients with nodular HCC and 33.3% and 13.6% (95% CI 7.9–58.7% and 0–35.1%) in patients with infiltrating HCC (p=0.0067), independent of the treatment received.
Discussion
Our results indicate the existence of two different pathways of HCC development in cirrhosis. A large cohort of cirrhotic patients was followed prospectively by periodic US examination of the liver allowing us to define the incidence but also the morphogenetic pattern of HCC development. While the majority of tumours were detected initially as small and well defined nodules, an infiltrating and more aggressive tumour was observed in a subgroup of patients. When risk factors were assessed by multivariate analysis, they were clearly different for these two types of HCC. Nodular HCC was associated with older age, longer duration, and more advanced stage of cirrhosis, and was unrelated to the aetiology of the underlying chronic liver disease, while development of an infiltrating and aggressive type of HCC was independent of duration or stage of cirrhosis and was strongly related to ongoing HBV infection or HBV and HCV coinfection. Patients developing this type of HCC were significantly younger than those with nodular HCC, indicating accelerated hepatocarcinogenesis in HBsAg carriers. This is in agreement with reports from regions with a high incidence of HCC and high prevalence of HBsAg carriage,22-27 but also with more recent findings obtained in regions with a lower incidence of HCC and lower prevalence of HBV carriers.27 ,28 In interpreting these results, it should be emphasised that patient follow up for survival analysis was censored at the date of developing one of the two types of HCC or at death. As the two forms of tumour should be seen as competing risks, the power in considering the impact of some factors such as, for example, age on infiltrating HCC, may have been reduced as age was a very strong prognostic marker for nodular HCC and older patients were much more likely to develop this form of HCC first, thus removing them from the risk set for infiltrating HCC. The same may have happened for other prognostic factors. Nevertheless, the results strongly suggest that different mechanisms of carcinogenesis may be involved in the two types of tumour. Two main mechanisms of carcinogenesis have been suggested for the development of HCC in patients with liver cirrhosis. One of these mechanisms implicates the cirrhotic process per se through the appearance of foci of hepatocyte dysplasia within the regenerative nodules, followed by definitive neoplastic transformation and clonal expansion as “nodule in the nodule”.29-32 In this pathway, the presence of regenerative nodules in the cirrhotic liver represents the main determinant of both the pathogenesis and morphogenesis of the tumour. Our results are in agreement with these concepts as they clearly demonstrate that development of nodular HCC is strictly dependent on the evolving cirrhotic process per se and may reflect neoplastic transformation within regenerative nodules. This would also be in keeping with the nodular pattern of growth, often with a surrounding capsule.
A second mechanism of carcinogenesis which may overlap with the previous one, implicates the effect of hepatitis viruses and of other aetiologic agents which, while causing chronic liver disease and cirrhosis, may also more directly promote neoplastic transformation by a number of molecular events. The prototype of this group of agents is HBV, which is known to integrate in the hepatocyte genome33-35 and also to express a number of transforming and transactivating proteins.35-37 Tumour could therefore develop in any part of the infected liver, independent of regenerative nodule and could therefore spread more rapidly in the surrounding parenchyma. In our patients, development of infiltrative or diffuse HCC was strongly associated with HBV infection, with or without HCV, independent of disease duration or stage, suggesting a more direct role of virus induced carcinogenesis.
In conclusion, cirrhotic patients may develop two different types of HCC. Cirrhosis per se, independent of aetiology, is associated with nodular HCC, which may represent neoplastic transformation of regenerative nodules with a risk that increases with disease duration and stage. Patients infected by HBV, with or without HCV coinfection, have an additional risk of developing an infiltrative and more aggressive type of HCC, which is independent of duration or stage of cirrhosis and may reflect more direct viral carcinogenesis.
Abbreviations used in this paper
- AFP
- α fetoprotein
- ALT
- alanine aminotransferase
- CT
- computerised tomography
- HBsAg
- hepatitis B surface antigen
- HBV
- hepatitis B virus
- HCC
- hepatocellular carcinoma
- HCV
- hepatitis C virus
- RR
- relative risk
- US
- ultrasound