Article Text

Abstract
BACKGROUND Steroid dependent patients with Crohn's disease are at high risk of developing glucocorticosteroid induced side effects.
AIMS We evaluated the possibility of switching from systemic steroids to budesonide (Entocort) in prednisolone/prednisone dependent patients with inactive Crohn's disease affecting the ileum and/or ascending colon.
PATIENTS Steroid dependent patients with a Crohn's disease activity index ⩽200 were included.
METHODS In a double blind multicentre trial, 120 patients were randomly assigned to receive budesonide 6 mg once daily or placebo. Prednisolone was tapered to zero during the first 4–10 weeks and budesonide or placebo was given concomitantly and for a further 12 weeks. Relapse was defined as an index >200 and an increase of 60 points from baseline or withdrawal due to disease deterioration.
RESULTS After one and 13 weeks without prednisolone, relapse rates were 17% and 32%, respectively, in the budesonide group, and 41% and 65% in the placebo group (95% confidence intervals for the difference in percentages −41%, −8% and −51%, −16%; p=0.004 and p<0.001, respectively). The number of glucocorticosteroid side effects was reduced by 50% by switching from prednisolone and was similar in the budesonide and placebo groups. Basal plasma cortisol increased in both groups.
CONCLUSIONS The majority of patients with steroid dependent ileocaecal Crohn's disease may be switched to budesonide controlled ileal release capsules 6 mg without relapse, resulting in a sharp decrease in glucocorticosteroid side effects similar to placebo, and with an increase in plasma cortisol levels.
- budesonide
- Crohn's disease
- steroid dependent
- prednisolone
Abbreviations used in this paper
- 5-ASA
- 5-aminosalicylate
- CD
- Crohn's disease
- CDAI
- Crohn's disease activity index
- CIR
- controlled ileal release
- GCS
- glucocorticosteroids
- IBDQ
- inflammatory bowel disease questionnaire
- QoL
- quality of life
Statistics from Altmetric.com
Crohn's disease (CD) is an inflammatory bowel disorder often initiated by an acute attack and may become chronic in some patients. Systemic glucocorticosteroids (GCS), such as prednisolone and prednisone, are commonly used in the treatment of acute attacks of the disease.1 ,2 Approximately one third of patients initially treated with GCS become GCS dependent: they remain in remission while receiving GCS but relapse when they are stopped.3 However, this treatment is often associated with serious side effects: metabolic (diabetes, hypertension, osteopenia) or cosmetic (moon face, hirsutism, acne).
Budesonide is a GCS with a marked topical anti-inflammatory effect and low systemic activity compared with conventional GCS4because of its marked potency combined with a high first pass metabolism (about 90%) to metabolites with minimal or no steroid activity.4 Budesonide (Entocort) controlled ileal release (CIR) capsules deliver the drug mainly to the ileum and ascending colon. This offers a new topical steroid treatment for patients with ileocolic CD, with a reduced risk of GCS induced side effects. In a placebo controlled dose finding study, budesonide CIR capsules were significantly more effective than placebo in inducing remission of active CD affecting the ileum and/or ascending colon, with an optimal dose of 9 mg daily.5 Budesonide 9 mg daily has also been found to be as effective as oral prednisolone6 ,7 but with fewer GCS induced side effects. In addition, budesonide CIR capsules have been shown to significantly prolong the time to relapse in patients with quiescent disease.8-10
We evaluated the effect of replacing prednisolone/prednisone with budesonide in steroid dependent patients with the possibility of improved tolerability.
Materials and methods
PATIENT SELECTION
The study was performed between April 1996 and October 1998. Eligible patients were at least 18 years of age and had inactive CD, as defined by a Crohn's disease activity index (CDAI) ⩽200. The index assesses eight variables: number of liquid stools, extent of abdominal pain, general well being, occurrence of extraintestinal symptoms, need for antidiarrhoeal drugs, presence of abdominal masses, haematocrit, and body weight.11 Relapse was defined as a score >200 and an increase of at least 60 points from baseline. Disease extent had to be confined mainly to the distal ileum, ileocaecal region, and/or ascending colon, except for scattered aphthous ulcers, and verified (by colonoscopy, small bowel follow through, or barium enema) within 24 months before randomisation. Patients with any major manifestations of CD in the rectum were not eligible, nor were those with septic complications, abscesses, perforations or active fistulae, ileostomy, pouch or colostomy, resection of the ileum of more than 100 cm, or who required immediate surgery. All patients had been receiving prednisolone or prednisone 10–30 mg/day, six months prior to the study, and at least two attempts to taper the dose with subsequent relapses had occurred. Patients receiving immunosuppressive or 5-aminosalicylate (5-ASA) treatment had started this treatment at least six months or one month, respectively, prior to the study and the dose had to be kept constant during the study. Patients treated with steroids in combination with azathioprine were initially excluded. However, to speed up inclusion of patients into the study, the inclusion criteria were changed during the study to allow the combination of steroids and azathioprine. Pregnant or breast feeding women and patients allergic to GCS were excluded.
The study was approved by the institutional review board at each centre and was conducted according to the principles of the second declaration of Helsinki. All patients gave written informed consent.
STUDY MEDICATION
The budesonide formulation used (Entocort capsules, 3 mg, AstraZeneca R&D, Lund, Sweden) is a gelatin capsule containing acid stable microgranules (each approximately 1 mm). The microgranules are composed of an inner sugar core surrounded by a layer of budesonide in ethylcellulose and an outer acrylic based resin coating (Eudragit L 100–55) that dissolves at a pH of 5.5 or higher. Placebo capsules were identical in appearance and taste.
TRIAL DESIGN
The trial was a randomised double blind study performed at 24 centres in six countries (Belgium, Denmark, France, Germany, Israel, and South Africa). Randomisation of patients in permuted blocks of four was performed separately for each centre using sealed and opaque treatment code envelopes. Treatment was scheduled for 16–22 weeks. Tapering of prednisolone (5 mg per week until 20 mg and thereafter 2.5 mg per week until the dose was reduced to zero) started concomitantly with intake of budesonide 6 mg once daily or placebo. Compliance was assessed by pill count. At entry, patient demographics and medical history, current and past diagnoses, and current medication were recorded. Sigmoidoscopy was performed to exclude major sigmoidorectal inflammation. CDAI was assessed before treatment and every four weeks until the prednisolone dose had been zero for a week, and then after a further six and 12 weeks or at the time of withdrawal for patients who discontinued the study. At the visits, a physical examination, quality of life (QoL) assessment, laboratory tests, physician's global evaluation, and an adverse events check were also performed. A short Synacthen test was performed at 8–10 am within 24 hours of the start of the study and after the last intake of study medication. Loperamide or other opiates to control diarrhoea were allowed.
QoL was assessed using the self administered inflammatory bowel disease questionnaire (IBDQ) which contains 32 questions each with seven possible answers numbered 1–7, where 7 is the most favourable.12 Ten questions are related to bowel movements, five to systemic symptoms, 12 to emotional functions, and five to social functions. The total score of the index is 32–224 (an increase in score is an improvement). QoL was also assessed by SF-36 with 36 questions where, in this study, the physical component summary and the mental component summary were used.13 The questionnaire is constructed to give a value of 50 (for mental and physical component summary scores) for the average US population. A high value is favourable.
Patients recorded on diary cards their intake of study medication, frequency of loose stools, abdominal pain, and general well being during the seven days before each visit. Blood samples were obtained for laboratory assessments: haematology, clinical chemistry, liver function tests, and indicators of inflammatory activity (erythrocyte sedimentation rate and C-reactive protein). Blood was drawn for measurements of plasma cortisol at the time of intravenous Synacthen (tetracosactrin, Ciba-Geigy) administration and 30 and 60 minutes later. A normal response was defined as a baseline plasma cortisol concentration of at least 5.4 μg/dl (150 nmol/l) and an increment above baseline of at least 7.2 μg/dl (200 nmol/l), or an absolute value above 14.4 μg/dl (400 nmol/l) at 30 or 60 minutes.
All adverse events were recorded, whether or not they were considered to be related to the study medication. GCS related side effects were actively asked for (moon face, buffalo hump, acne, hirsutism, purple skin striae, bruises easily, swelling of ankles, hair loss, mood swings, depression, and insomnia). A serious adverse event was defined as one which suggested a significant hazard or handicap to the patient (death, permanent disability, cancer, hospitalisation) or was life threatening. Adverse events were assessed for intensity using the scale mild, moderate, or severe (where severe was incapacitating with inability to work or to take part in normal activities). The number of possibly GCS related side effects was recorded at each visit and their intensity graded from 1 to 3. Patients could be withdrawn from the study at any time if their physicians believed their condition had deteriorated substantially. In such cases, CDAI was assessed.
STATISTICAL ANALYSIS
It was estimated that 50 patients per group would have to be studied to detect a 30% difference in relapse rates, assuming a relapse rate of 50% with budesonide treatment. The primary outcome was relapse rate, with relapse defined as a score of >200 and an increase of 60 points from baseline in CDAI, or withdrawal due to disease deterioration. The primary analysis was based on all patients treated with at least one dose of study medication. Exploratory analyses (determined in advance) investigated the influence of prognostic factors on relapse rates by two way analysis of variance, with initial prednisolone dose, treatment, subgroup (for example, sex), and their interaction as factors.
Secondary variables were (1) changes in CDAI, (2) time to relapse, (3) quantitative changes in QoL index, and (4) changes in safety variables (such as plasma cortisol, GCS side effects, and adverse events).
The last value carried forward approach was used for missing data—that is, the value last recorded for the patient was used in the analysis. If a patient suffered a relapse according to the above definition, they were registered as having relapsed for the remaining study period. The χ2 test was used to compare proportions. Time to discontinuation and time to relapse were analysed by Kaplan-Meier curves and a generalised Wilcoxon test.14 The Student'st test, Wilcoxon test, and analysis of variance were used for quantitative variables. All tests were two sided; p values not exceeding 5% were considered significant. The adverse events profile was analysed by means of descriptive statistics and qualitative analysis.
Results
A total of 120 patients were randomly assigned to receive budesonide (60 patients) or placebo (60 patients). One hundred and eighteen patients took at least one dose of study drug. One patient was excluded from the efficacy analysis because of tuberculosis, which was discovered after the patient had completed the study. Baseline characteristics were similar in the two groups (table 1). The mean time during which patients had taken prednisolone before the start of the study was 514 days in the budesonide group and 346 days in the placebo group. A flow chart describing the patients in the study is shown in fig 1.
Baseline characteristics of the patients
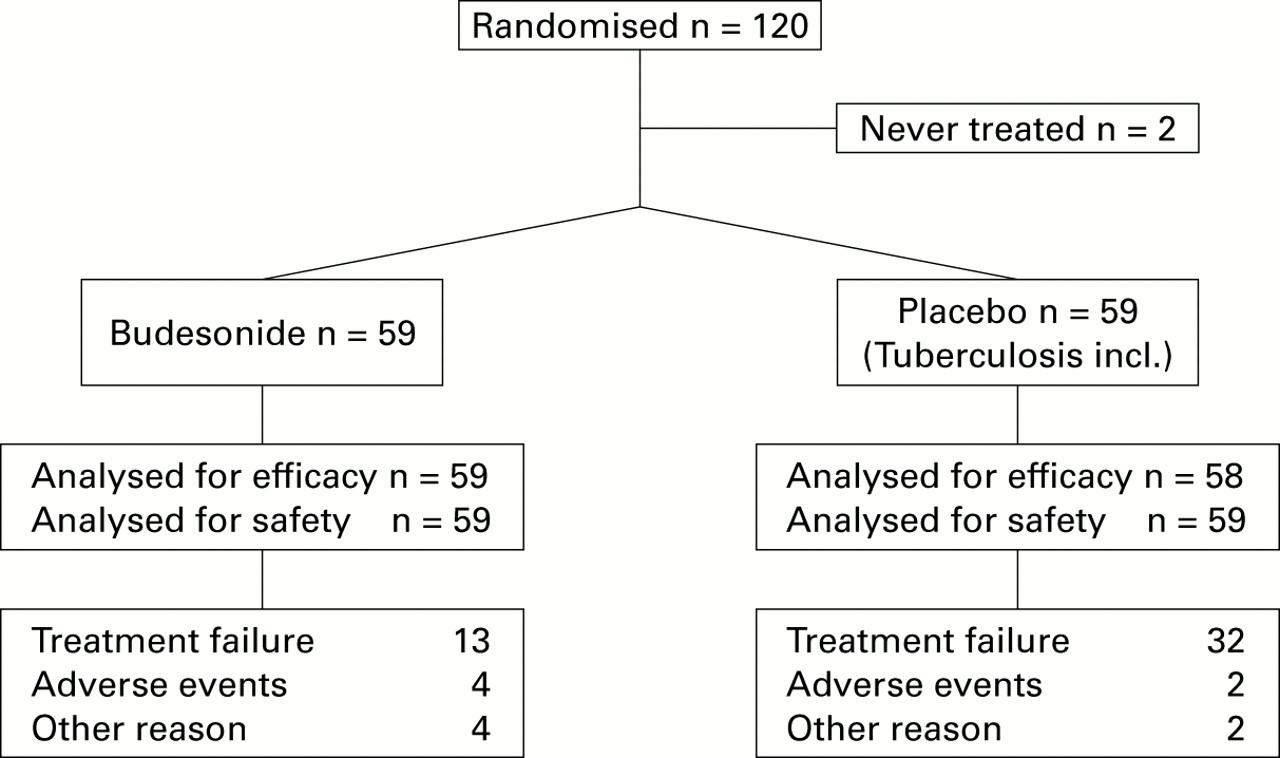
Flow chart of patients and reasons for discontinuation.
CLINICAL EFFICACY
Relapse rates were lower in the budesonide group than in the placebo group; after one and 13 weeks without prednisolone, 10 and 19 patients, respectively, had suffered a relapse (17% and 32%) in the budesonide group and 24 and 38 patients (41% and 65%) in the placebo group (p=0.004 and p<0.001).
Sex, previous intestinal resection, initial prednisolone dose, and use of azathioprine or 5-ASA treatment had no influence on relapse rates.
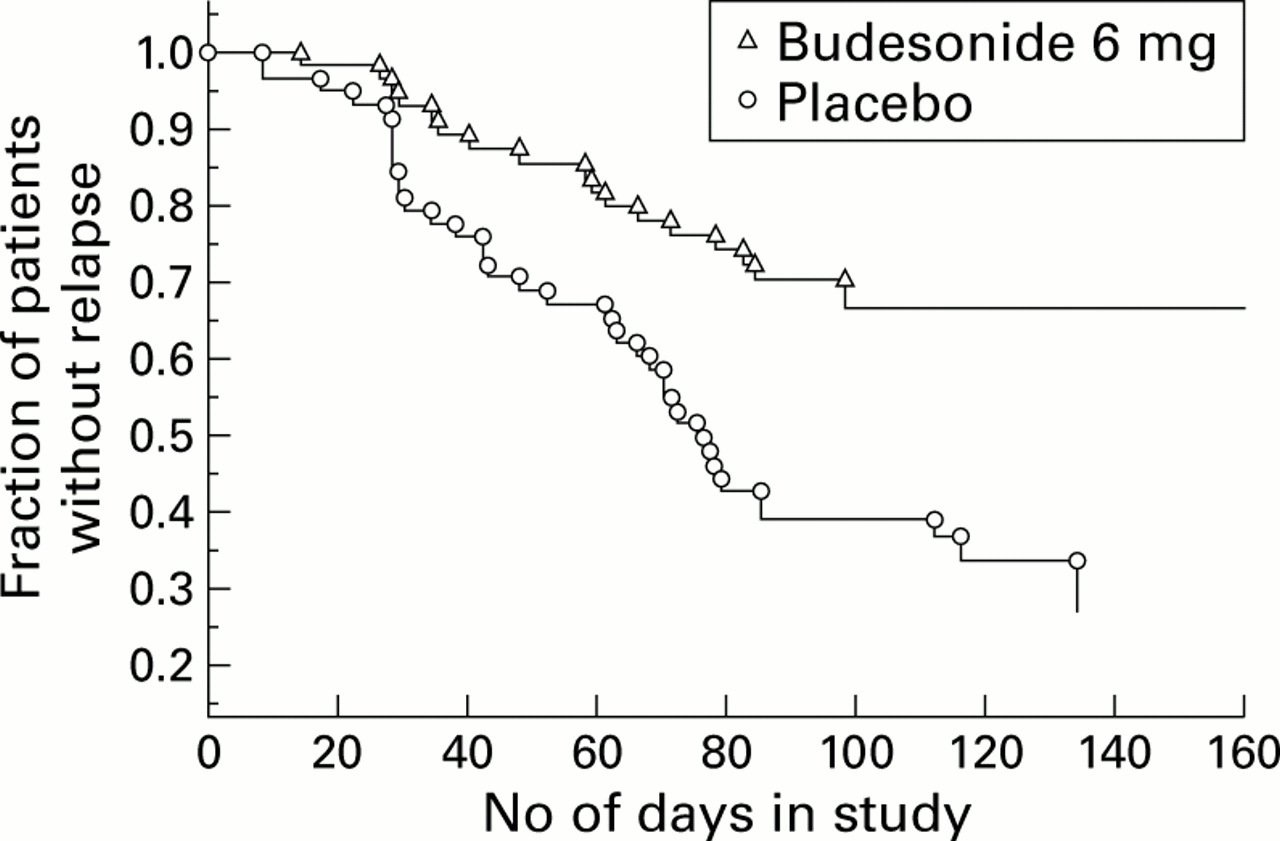
Median time to relapse was significantly longer for budesonide (>160 days) than for placebo (75 days) (p<0.001) (fig 2).

Time to relapse in the budesonide and placebo groups.
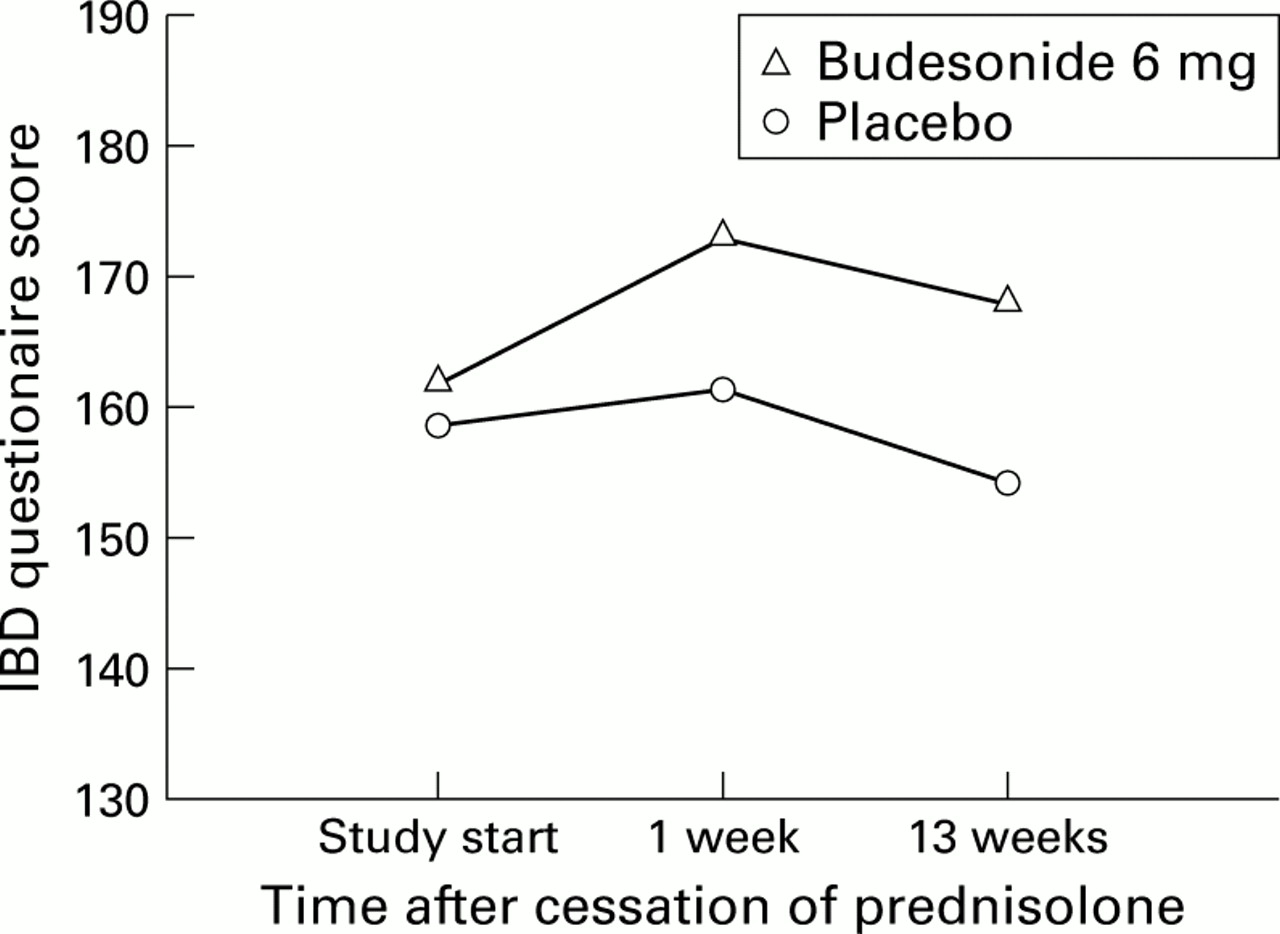
Total averages for IBDQ scores are given in fig 3. The scores were similar in the two treatment groups at the start of the study. IBDQ score was always better in the budesonide group than in the placebo group either at one or 13 weeks, achieving a significant difference (p=0.025) at week 13. Improvement occurred in emotional and social function scores. For SF-36, there was a discrepancy between the evolution of the physical component summary which improved significantly (p=0.005) at week 13 and the mental component summary which did not differ between treatment groups during the study.

Scores from the inflammatory bowel disease (IBD) questionnaire for the budesonide and placebo groups.
No clinically important differences between treatments were found in the assessments of haematological and biochemical variables.
ADVERSE EVENTS
There was a positive correlation between initial prednisolone dose and baseline GCS side effects (p<0.001). The number of side effects was reduced from the start of the study (when patients were receiving prednisolone) in both the budesonide and placebo groups (fig 4). For individual side effects, average intensity observed at each visit decreased mainly in moon face (fig 5), acne (fig 6), insomnia, and mood swings. An intensity score of 1 represents mild intensity.
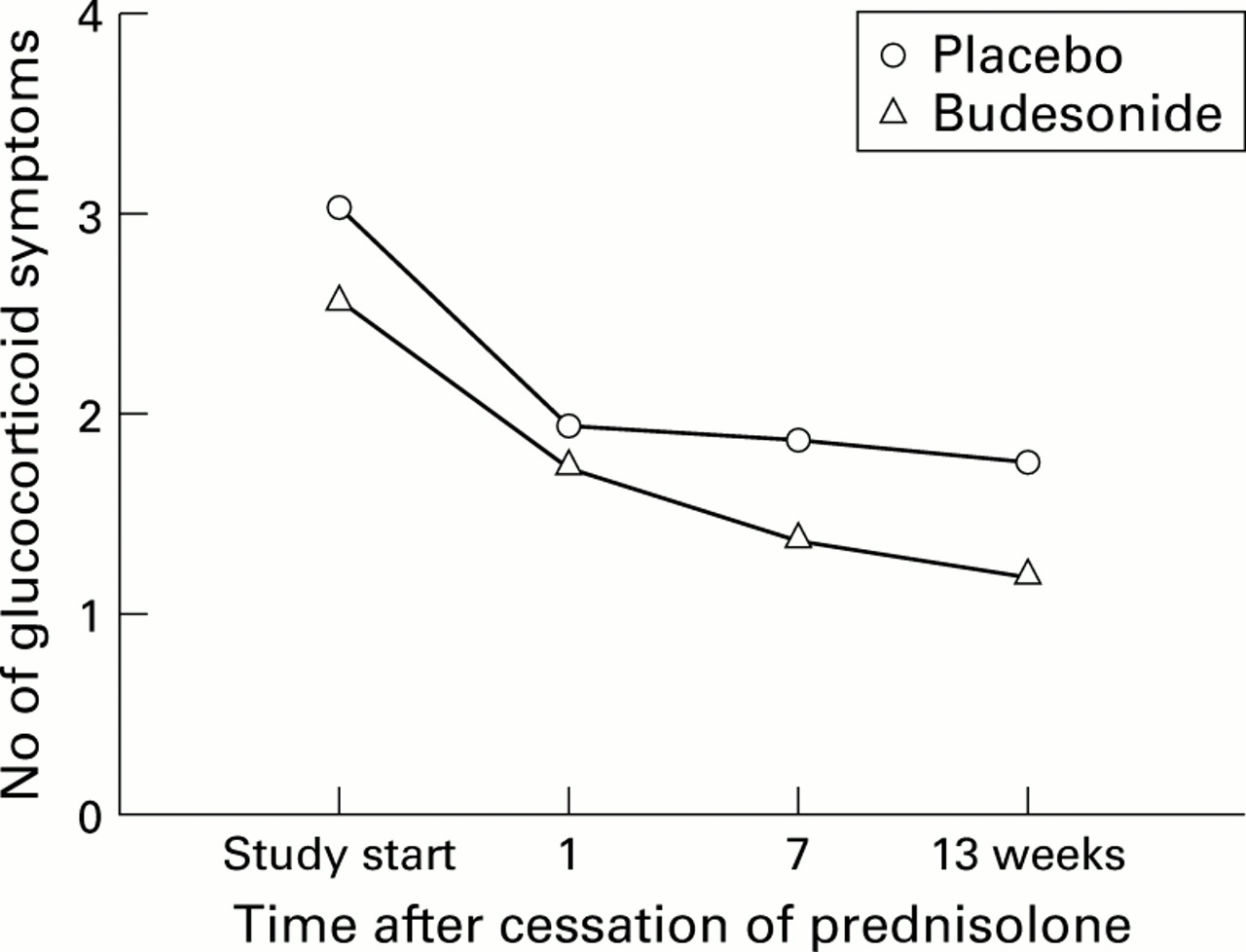
Number of glucocorticosteroid related symptoms in the budesonide and placebo groups.

Average intensity of moon face at each visit in the budesonide and placebo groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Average intensity of acne at each visit in the budesonide and placebo groups.
The number of patients with adverse events was similar in the two groups; the most frequent events are shown in table 2. All serious adverse events were due to hospitalisation of patients. No serious adverse events were considered causally related to the study drug.
Adverse events in the budesonide and placebo groups
ADRENAL FUNCTION
Mean morning unstimulated plasma cortisol increased by 5.0 μg/dl (139 nmol/l) from the first to the last visit in the budesonide group (n=37) and by 9.3 μg/dl (257 nmol/l) in the placebo group (n=30). This increase in unstimulated plasma cortisol from baseline (prednisolone treatment) was statistically significant for both budesonide (p=0.0074) and placebo (p<0.0001). According to our criteria (including basal and stimulated cortisol level), in the budesonide group, 23/37 patients had abnormal adrenal function at entry. Of those 23, 12 (52%) recovered normal function at the last visit. In the placebo group of 30 patients, 23 had abnormal adrenal function of whom 19 (83%) recovered normal function at the last visit.
Discussion
In this study, budesonide capsules (6 mg once daily) were more effective than placebo in maintaining remission in steroid dependent patients with inactive ileocaecal CD when systemic steroid was tapered to zero. Thus systemic steroid dependent patients could be switched to budesonide with a limited risk of relapse (68% without relapse after 13 weeks of budesonide). The majority of flare ups due to a change in steroids should appear within three months given the tough criterion for steroid dependency which implied that patients were in constant need of steroids. Sex, previous intestinal resection, initial prednisolone dose, and use of azathioprine or 5-ASA treatment did not influence relapse rate. Including patients receiving steroids in combination with azathioprine was initially regarded as inadvisable because of the risk of confusing the study. To speed up inclusions into the study however, patients who were receiving azathioprine were eventually included, resulting in a few patients in both groups.
Previous experience of replacement of systemic steroids with budesonide in CD was limited to a shorter study using a different formulation and no placebo group.15 There is greater experience of the use of budesonide in patients achieving remission after treatment, and subsequently being treated with budesonide 3 or 6 mg/day or placebo. Budesonide 6 mg/day significantly prolonged the time in remission by 109 days compared with placebo.10 In chronic systemic steroid dependent asthmatics, a similar finding (inhaled budesonide had a prednisolone sparing effect) was reported.16
Systemic steroids are an important part of the therapy alternatives in CD but their use is limited by side effects, particularly in steroid dependent patients. The use of systemic steroids has a negative impact on QoL in patients with CD, correlated with the dose received by the patient.17 One of the motives behind switching from systemic steroids to budesonide was to reduce the steroid induced side effects, particularly the so called “cosmetic” effects (moon face, acne, easy bruising, hirsutism) and the intensity of mood swing and insomnia. These in part resulted in a global improvement in QoL in both groups. However, QoL improved more in the budesonide group than in the placebo group, probably reflecting the better control of disease activity in the budesonide group. At the start of the study there were more patients with abnormal than with normal adrenal function and this changed towards a higher number of patients with normal than with abnormal function in both groups at the last visit (numerically higher in the placebo group). Average plasma cortisol levels increased in both groups over the course of the study.
Switching from systemic steroids to budesonide (6 mg/day) may be proposed in steroid dependent patients with inactive ileocaecal CD and such a switch has the potential to decrease GCS associated side effects and produce a beneficial effect on the HPA axis in these patients. Azathioprine/6-mercaptopurine and methotrexate are currently regarded as the standard therapy in this situation.18-20Budesonide could however be proposed in patients receiving steroids in whom immunosuppressors are temporarily ineffective or contraindicated. In the light of the results of our study, budesonide could be evaluated as an alternative to standard therapy.
Acknowledgments
Supported by AstraZeneca R&D, Lund, Sweden.
Appendix
In addition to the authors, the following participated in the international budesonide study group: Hopital Nord, Amiens, France (J Dupas); Hopital Charles Nicolle, Rouen, France (E Lerebours); Hopital Saint-Louis, Paris, France (R Modigliani); Hopital Hautepierre, Strasbourg, France (B Duclos); Hopital Rotschild, Paris, France (J Gendre); Hopital Cochin, Paris, France (S Chaussade); Hopital Henri Mondor, Creteil, France (J Delchier); Hospital OLV Middelares, Antwerpen, Belgium (O Peters); Tygerberg Hospital, Cape Town, South Africa (C van Rensburg); Soroka Hospital, Beer-Sheva, Israel (A Fich); Asaf-Harofeh Medical centre, Zrifin, Israel (E Scapa); Haemek Medical Centre, Afula, Israel (E Nussinson); Kaplan Hospital, Rehovot, Israel (D Bass); Medizinische Universität, Lubeck, Germany (E Stange); Medizinische Hochschule, Hannover, Germany (M Göke); Aalborg Sygehus, Aalborg, Denmark (J Fallingborg); Herlev Hospital, University of Copenhagen, Denmark (O Ø Thomsen); Hillerod Sygehus, Hillerod, Denmark (S Kiilerich).
Abbreviations used in this paper
- 5-ASA
- 5-aminosalicylate
- CD
- Crohn's disease
- CDAI
- Crohn's disease activity index
- CIR
- controlled ileal release
- GCS
- glucocorticosteroids
- IBDQ
- inflammatory bowel disease questionnaire
- QoL
- quality of life
References
Footnotes
↵† Members of the study group are listed in the .