Article Text

Abstract
BACKGROUND Hepatocellular carcinoma (HCC) is a major cause of death in cirrhotic patients. This neoplasm is associated with liver cirrhosis (LC) in more than 90% of cases. Early diagnosis and treatment of HCC are expected to improve survival of patients.
AIMS To assess the cost effectiveness of a surveillance programme of patients with LC for the early diagnosis and treatment of HCC.
PATIENTS A cohort of 313 Italian patients with LC were enrolled in the surveillance programme between March 1989 and November 1991. In the same period, 104 consecutive patients with incidentally detected HCC were referred to our centre and served as a control group.
METHODS Surveillance was based on ultrasonography (US) and α fetoprotein (AFP) determinations repeated at six month intervals. Risk factors for HCC were assessed by multivariate analysis (Cox model). Outcome measures analysed were: (1) number and size of tumours; (2) eligibility for treatment; and (3) survival of patients. Economic issues were: (1) overall cost of surveillance programme; (2) cost per treatable HCC; and (3) cost per year of life saved (if any). Costs were assessed according to charges for procedures at our university hospital.
RESULTS Surveillance lasted a mean of 56 (31) months (range 6–100). During the follow up, 61 patients (19.5%) developed HCC (unifocal at US in 49 cases), with an incidence of 4.1% per year of follow up. AFP, Child-Pugh classes B and C, and male sex were detected as independent risk factors for developing HCC. Only 42 (68.9%) of 61 liver tumours were treated by surgical resection, orthotopic liver transplantation, or local therapy. The cumulative survival rate of the 61 patients with liver tumours detected in the surveillance programme was significantly longer than that of controls (p=0.02) and multivariate analysis showed an association between surveillance and survival. The overall cost of the surveillance programme was US$753 226, the cost per treatable HCC was US$17 934, and the cost for year of life saved was US$112 993.
CONCLUSION Our surveillance policy of patients with LC requires a large number of resources and offers little benefit in terms of patient survival. The decision whether to adopt a surveillance policy towards HCC should rely on the prevalence of the disease in the population and on the resources of a particular country.
- hepatocellular carcinoma
- surveillance programme
- cost effectiveness
Abbreviations used in this paper
- AFP
- α fetoprotein
- CT
- computed tomography
- HCC
- hepatocellular carcinoma
- LC
- liver cirrhosis
- OLT
- orthotopic liver transplantation
- PEI
- percutaneous ethanol injection
- TACE
- transarterial chemoembolisation
- US
- ultrasonography
Statistics from Altmetric.com
Liver cirrhosis (LC) is a well known risk factor for the development of hepatocellular carcinoma (HCC). In Japan it has been recognised as the major cause of death in cirrhotic patients.1 In Italy and in other areas with an intermediate incidence of HCC (5–20 cases per 100 000 inhabitants) this neoplasm is associated with LC in more than 90% of cases. Based on the availability of new imaging techniques, namely ultrasonography (US), together with serum α fetoprotein (AFP) determinations, many mass screening studies of cirrhotic patients were undertaken in eastern and subsequently in western countries2-14 in the second half of the eighties with the aim of providing earlier diagnosis or more effective treatment for HCC. These studies did in fact provide enhanced knowledge of the prevalence and incidence of liver cancer and of individual risk factors in cirrhotic patients. The reported incidence of HCC, both in eastern and western studies, varied between 3% and 6.5% per year of follow up5-13 and in most studies a high serum AFP level was identified9-11 ,13 ,14as a significant independent risk factor for HCC in cirrhotic patients. In other studies, male sex, hepatitis B virus, hepatitis C virus, ethanol abuse, and previous blood transfusions8 ,10 ,11were identified as additional risk factors but of lower significance than high AFP levels. Some8 ,14 ,15 have also demonstrated that tumours detected in surveilled patients are frequently unifocal and of small size.
A critical point, which remains to be addressed, is the cost effectiveness of these surveillance programmes. Whether they really improve the outcome of the disease (better chance for effective treatment and reduced disease specific mortality) remains to be established as randomised controlled trials comparing surveilled and unsurveilled populations have not been performed.
In order to answer these questions, we evaluated the clinical effectiveness and cost of a prospective surveillance programme of cirrhotic patients undertaken at the Department of Internal Medicine, University of Bologna, in 1989.
Patients and methods
STUDY DESIGN
Between March 1989 and November 1991, a cohort of patients with LC and without HCC, hospitalised at the Department of Internal Medicine, S Orsola-Malpighi University Hospital, or referred as outpatients to the liver unit of the department were enrolled in the study. The diagnosis of LC was histologically proved or made on unequivocal clinical, biochemical, ultrasonographic, and endoscopic findings. Exclusion criteria were: (1) Child-Pugh C class16 in patients older than 60 years; (2) a previous diagnosis of focal liver lesion at US; and (3) a serum AFP level >200 ng/dl. Patients were withdrawn from further surveillance when they were >60 years old and belonged to Child-Pugh C class, developed other neoplasms, or underwent orthotopic liver transplantation (OLT).
The study protocol conformed to the ethical guidelines of the 1975 declaration of Helsinki. All patients gave informed consent to enter the prospective surveillance programme in conformity with the modalities reported below. The initial evaluation included clinical examination, routine biochemical tests, determination of serum AFP, upper gastrointestinal tract endoscopy, and abdominal US.
During the subsequent surveillance period, serum AFP determinations and abdominal US, together with physical examination and routine biochemical tests, were repeated every six months.
DIAGNOSIS AND STAGING STRATEGY
The diagnostic protocol for detection of a nodular liver lesion at US was based on contrast enhanced computed tomography (CT) and echo guided biopsy (when feasible, according to location of the nodule and bleeding risk). When a negative result was obtained after CT and echo guided biopsy, a strict follow up procedure was followed (three month intervals) and the nodule was rebiopsied when an increase in size was detected at US. Morphological staging (number of nodules, location, and vascular involvement) of HCC was based on US and CT findings. Treatment selection was based on this morphological stage and other parameters related to the severity of the underlying cirrhosis and patient characteristics, such as Child-Pugh class, age of the patient, and coexisting diseases (see “treatment schedule” below). Angiography and lipiodol CT were used only for therapeutic purposes and prior to surgical treatments. All diagnoses of HCC were further confirmed on surgical specimens or by follow up.
The incidence of HCC during follow up of the study population was first assessed and individual risk factors for developing HCC were investigated using multivariate analysis.
For the control group, we evaluated a consecutive series of HCC incidentally detected outside any specific surveillance programme in the same period (March 1989 to November 1991) and referred to our centre for definite diagnosis and treatment (contemporaneous non-randomised controls). A comparative analysis was made between characteristics and outcome of HCC detected during the prospective surveillance programme and those which arose in the unsurveilled population. Follow up of patients ended in December 1997 when the data were analysed.
TREATMENT SCHEDULE
When a diagnosis of HCC was established, the following therapeutic options were first considered both for the surveilled and unsurveilled patients:
- (a)
- hepatic resection for patients of Child-Pugh A class with unifocal nodules located in peripheral segments;
- (b)
- percutaneous ethanol injection (PEI) and/or transarterial chemoembolisation (TACE) for all Child-Pugh B patients over 60 years with unifocal nodules, for Child-Pugh A patients with unifocal nodules located centrally in the liver and over 60 years, for patients who refused surgery, and for patients with 2–3 nodules. The choice between the two procedures was done case by case according to the characteristics of the HCC (size, location) and of the underlying cirrhosis;
- (c)
- TACE was the only option for cases with more than three nodules or diffuse HCC involving less than 30% of the liver parenchyma;
- (d)
- OLT was considered for all patients with unifocal nodules <60 years old, except for those Child-Pugh A subjects with resectable nodules. A single session of TACE was performed in Child-Pugh A and B patients prior to assignment to the waiting list for OLT; further sessions were subsequently performed at four month intervals until transplantation.
Exclusion criteria for treatment were neoplastic portal vein thrombosis, diffuse HCC (>30% of the liver involved), other life threatening diseases, and Child-Pugh C class in patients >60 years old. Patients >75 years were considered only for PEI.
OUTCOME MEASURES AND ECONOMIC ISSUES
Outcome measures analysed in patients with HCC were: (1) number and size of HCC nodules detected by US; (2) eligibility for surgical or local treatment; (3) survival of patients with HCC; and (4) survival of all cirrhotic patients. The economic issues were calculated according to the charges at our university hospital for the various diagnostic and therapeutic procedures. They were: (1) overall cost of the surveillance programme (derived from charges for AFP, US, and other diagnostic procedures performed in patients with nodular lesions); (2) cost (derived from charges of diagnostic and therapeutic procedures) per treatable HCC; and (3) cost per year of life saved (if any).
METHODS
AFP assay was performed by immunoenzymology using a commercial kit (Roche Diagnostica). US examination was carried out by three experienced gastroenterologists (SG, SS, GZ) specifically trained in US, using real time scanners (Esaote-Hitachi SSD 450 and Au 590 Asynchronous) with 3.5 MHz convex array transducers provided with pulsed and colour Doppler facilities. The size of any mass lesion detected by US was measured by calculating its volume (in cm3) from the section plane containing the largest diameter and the plane perpendicular to it. The formula 4/3 πr3was used for spherical nodules and 4/3 π(a/2×b/2)3 for non-spherical nodules.17 Lesions with undefined boundaries and appearance of diffuse infiltration or vascular involvement were classified as diffuse or infiltrating and their volume was not measured or their progression assessed.
PATIENTS
A total of 313 patients with LC screened by US and AFP were enrolled in the surveillance programme and had a follow up of at least six months. The characteristics of the study population are summarised in table 1. Contemporaneous controls numbered 104.
Characteristics of the patients enrolled in the study (n=313)
STATISTICAL ANALYSIS
The cumulative rate of HCC detected during the surveillance programme and survival curves for HCC detected during follow up and those in the unsurveilled population were calculated by life tables according to the Kaplan-Maier method18 and differences were tested by log rank test. The incidence of HCC per year of follow up was calculated according to a person time unit method, to fully utilise the whole period of follow up of each person. The Wilcoxon test was applied for comparison between tumour masses. The χ2test was used for comparisons between proportions in different groups.
The following variables were first investigated by univariate analysis in the group of 313 patients undergoing the surveillance programme: age, sex, hepatitis B virus, hepatitis C virus, antibodies to hepatitis B virus, ethanol abuse, primary biliary cirrhosis, cryptogenic cirrhosis, Child-Pugh class at entry, and serum AFP level at entry. The stepwise Cox proportional hazard model19 was used to identify those variables significantly and independently associated with the risk of HCC. All assumptions of the Cox model were tested and met. The relative importance of each variable identified was estimated on the basis of the ratio between the variable coefficient and its standard error. Patients with LC who developed other tumours or hepatic decompensation aged >60 years, those who underwent OLT, those lost to follow up, and those who died of causes unrelated to LC were regarded as censored cases.
To calculate the number of months of life possibly saved in surveilled patients in comparison with those unsurveilled, median survival times obtained from life tables were used, according to the recommendations of Peto and colleagues,20 which were applicable to our series.
The incremental cost per incremental unit of clinical outcome21 was estimated by calculating the incremental cost (if any) for treatable HCC in the surveilled population. The cost per year of life saved was consequently measured by dividing the incremental cost for the number of months of life gained in the surveilled group.
A multivariate analysis was performed to identify variables associated with survival. In this analysis, sex, Child-Pugh class, tumour staging, and inclusion in the surveillance programme were considered.
Results
INCIDENCE OF HCC DURING THE SURVEILLANCE PROGRAMME
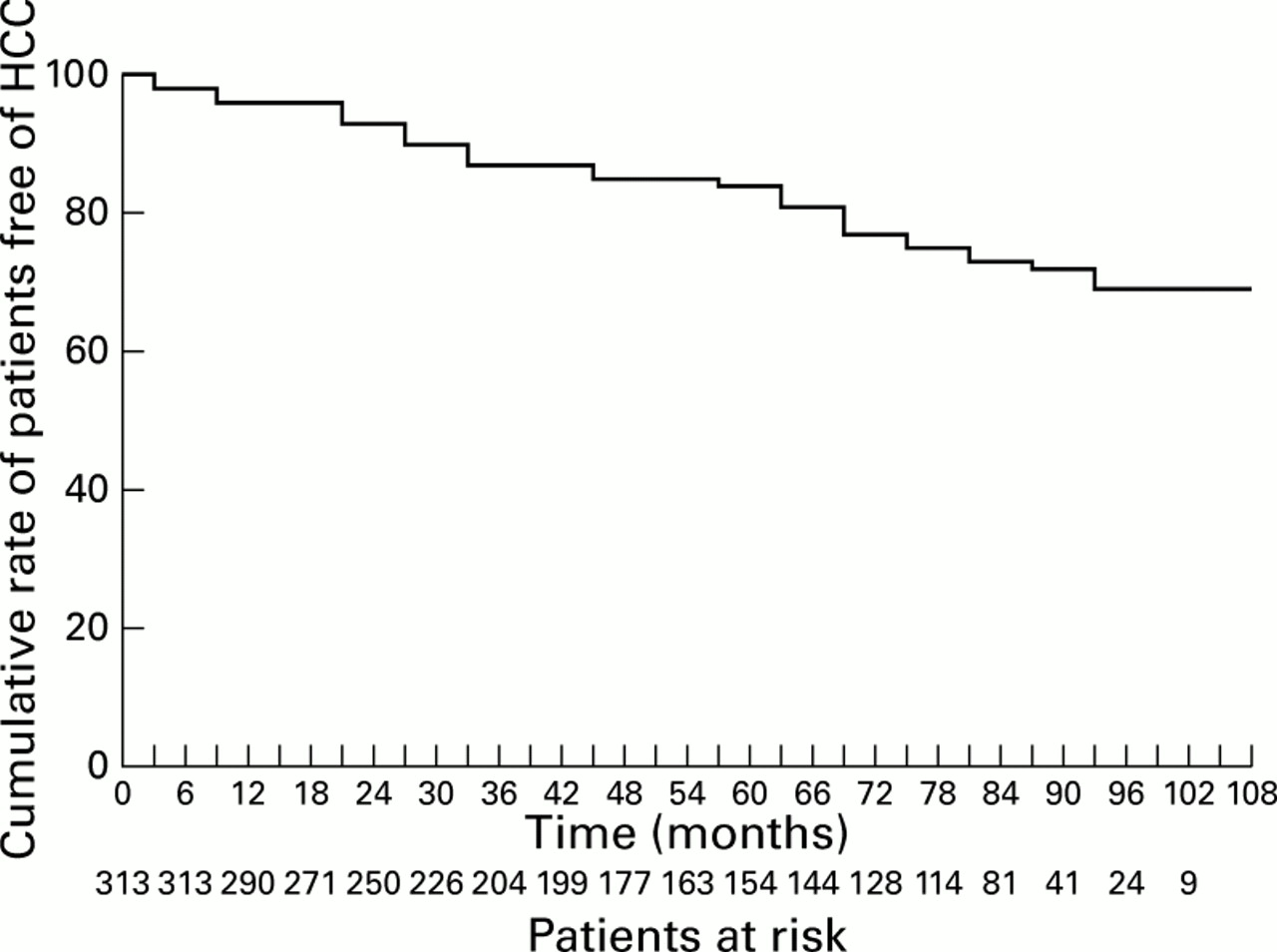
The mean follow up period of the cohort of 313 patients in the surveillance programme was 56 (SD 31) months (range 6–100 months). During this follow up period nodular liver lesions were detected in 74 cases by US (23.6%). In 13 cases (4.1%) the diagnosis of HCC could not be proved at the time of data analysis by other imaging techniques or by US guided biopsy and the final diagnosis was: macroregenerative nodule in six cases, haemangioma in three cases, and undefined in the remainder. All lesions were <2 cm in diameter. In 61 cases (19.5%) the diagnosis of HCC was finally proved by US guided biopsy (in 49 cases) and/or lipiodol CT and was confirmed at follow up. Four of these HCC were first diagnosed as macroregenerative nodules and subsequently met the criteria for a diagnosis of HCC. The sensitivity and specificity of the AFP assay at entry at the cut off level of 20 ng/dl were 41% and 82%, respectively, with a positive predictive value of 46% and negative predictive value of 85%. In none of the cases in the present series was a diagnosis of HCC made on the basis of an increase in AFP above 200 ng/dl in the absence of US visualisation of a liver mass. Figure 1 shows the rate of development of HCC over the period of observation. The incidence of HCC per year of follow up was 4.1%.

Cumulative rate of patients free of hepatocellular carcinoma (HCC) in the cohort of 313 patients with liver cirrhosis.
At the end of the study, 111 (35.5%) patients were still in follow up and 61 (19.5%) had developed HCC. The remaining patients were censored for the following reasons: 65 (20.8%) had died of liver failure or variceal haemorrhage, 24 (7.7%) had undergone transplantation, 24 (7.7%) were lost to follow up, 13 (4.3%) developed a non-hepatic malignant neoplasm, 10 (3.2%) died of non-liver related causes (mainly cardiovascular diseases), and five (1.6%) were over 60 years old in Child-Pugh class C.
ANALYSIS OF RISK FACTORS FOR HCC
Child-Pugh class at entry into the study of the 61 cirrhotic patients who developed HCC during the surveillance programme were as follows: 35 class A (57.4%), 21 class B (34.4%), and five class C (8.2%). Serum AFP levels at entry into the study were normal (<20 ng/dl) in 258 patients (82.4%) and >20 ng/dl in 55 (17.6%).Throughout the follow up period AFP levels remained less than 20 ng/dl in 236/313 patients (75.5%) and were persistently elevated in 37/313 (11.9%). In 24/313 patients (7.6%) (18 from the group with elevated AFP and six with normal AFP levels at entry), AFP levels fluctuated around the upper normal level, and in 16/313 (5.0%) they showed an increasing pattern above the normal range.
Univariate analysis of risk factors for HCC proved significant for sex, AFP >20 ng/dl, and Child-Pugh B/C class (table 2). The Cox model identified serum AFP >20 ng/dl at entry (coefficient/SE 4.03), Child-Pugh B/C class (coefficient/SE 3.06) and male sex (coefficient/SE 2.06) as independent significant risk factors for the development of HCC (table 2). In this model each variable was categorised binomially as 1 or 2 if, respectively, values were below/⩾20 ng/dl for AFP, A or B/C for Child-Pugh class, and female or male for sex. Figure 2 shows the differences in the rates of developing HCC among the different risk classes of cirrhotic patients stratified with respect to the most powerful risk factors (AFP and Child-Pugh class at entry) identified by the Cox model.
Risk factors for hepatocellular carcinoma in 313 patients with liver cirrhosis

Cumulative rates of patients free of hepatocellular carcinoma (HCC) according to Child-Pugh class and α fetoprotein (AFP) level at entry into the study. 1, Child-Pugh class B/C and AFP >20 ng/ml (n=26); 2,Child-Pugh class A and AFP <20 ng/ml (n=173); 3, Child-Pugh class A and AFP >20 ng/ml (n=27); 4, Child-Pugh class B/C and AFP <20 ng/ml (n=87).
NUMBER AND SIZE OF THE DETECTED LESIONS
Table 3 reports the clinical pattern and morphological features of incidental HCC in the surveilled population. Sixty one HCC were unifocal at US in 49 cases (80.4%), multifocal in six cases (9.8%), and diffuse in six (9.8%). In 7/49 (14.3%) HCC that were unifocal at US the subsequent staging and therapeutic procedures revealed a multifocal hepatic disease. The mean (SD) volume of the tumour mass, calculated only in unifocal HCCs, was 12.5 (18.9) cm3. The ultrasonographic stage of HCC at the time of detection did not significantly change during follow up. This implies that HCCs detected in the last period of the study were similar to those detected at the beginning. Only 55 HCC of the unsurveilled population were unifocal (52.9% v 80.4% of HCC in surveilled patients; p<0.001) and the mean (SD) volume of their tumour mass was 20.1 (42.2) cm3 (NS v unifocal HCC in surveilled patients) (table4).
Clinical pattern, staging, and outcome of liver cancers that arose during follow up
Characteristics of incidental hepatocellular carcinomas and of contemporaneous non- randomised controls
ELIGIBILITY FOR TREATMENT
In 19 liver cancers (31.1%) of the 61 detected during the surveillance period, the possibility of treatment was ruled out and no specific therapy was performed for the following reasons: diffuse HCC (six cases), refusal by the patient (five cases), liver failure (two cases), severe portal hypertension with previous bleeding episodes (two cases), and other causes (coexistent systemic disease or congenital splanchnic arterial abnormality preventing TACE; four cases). In the remaining 42 cases (68.9%) the following treatments were carried out (table 3): TACE was performed as the sole treatment in 13 elective patients and in five patients who died while on the waiting list (n=3) or while still awaiting OLT (n=2) at the time of analysis. The mean number of TACE sessions was 2.2 (range 1–3) in this group. TACE+PEI was performed in four patients, with a single session of TACE preceding PEI. PEI was the sole treatment in 10 cases. Hepatic resection was performed in four cases. Eleven patients were selected or considered candidates for OLT; six received OLT 6–12 months after the diagnosis of HCC, three died awaiting OLT, and two are still on the list. All but three patients (who had decompensated LC) in this group received TACE prior to assignment. Eligibility for treatment was not significantly different in cases arising during the first three years of the surveillance programme compared with those arising in the last period (table 3). Sixty one of the unsurveilled HCC patients were treated (58.6% v 68.8% surveilled; NS) (TACE n=28; PEI n=14; hepatic resection n=5; TACE+PEI n=6; OLT n=8).
SURVIVAL ANALYSIS OF PATIENTS WITH HCC
Survival of patients with HCC detected during the surveillance programme proved significantly longer (p=0.02) than that of unsurveilled patients (fig 3). The three year survival rates were, respectively, 45% and 31.7% (median survival 30v 15 months).

Cumulative survival rates of hepatocellular carcinoma (HCC) detected during follow up and HCC detected in unscreened patients. 1, HCC detected in surveilled patients (36 dead, 25 censored); 2, HCC detected in unsurveilled patients (95 dead, nine censored).
SURVIVAL ANALYSIS OF PATIENTS ENROLLED IN THE PROSPECTIVE STUDY
A total of 112 (35.8%) of 313 patients who entered the surveillance programme died; 37 (11.8%) had HCC. The cumulative survival rate of cirrhotic patients and patients with HCC which arose during the follow up, stratified according to Child-Pugh class, is shown in fig 4. The three year survival rates of cirrhotic patients in Child-Pugh A and B/C classes compared with that of patients with HCC in the corresponding Child-Pugh classes were, respectively, 92% versus 66% (p<0.05) and 71% versus 34% (p<0.05). Multivariate analysis identified tumour staging (p<0.001) and Child-Pugh score (p<0.01) as the variables independently associated with survival. However, if tumour staging was removed from the analysis, inclusion in the surveillance programme became significantly associated (p<0.01) with survival, indicating that these two variables, tumour staging and surveillance, are strictly related, but with the former prevailing on the latter.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative survival rates of patients with liver cirrhosis (LC) enrolled in the study and patients with incidental hepatocellular carcinoma (HCC) stratified according to Child-Pugh class. 1, LC and Child-Pugh A class; 2, LC and Child-Pugh B/C class; 3, HCC and Child-Pugh A class; 4, HCC and Child-Pugh B/C class.
COST OF THE SURVEILLANCE PROGRAMME
To carry out the present surveillance programme we performed 2874 abdominal US examinations and AFP determinations. The cost of such a programme, based on charges for US examinations and serum AFP assays performed twice a year during a mean follow up period of 56 months in 313 patients, was US$175 314. Additional charges for the definite diagnosis and staging of the 74 nodular lesions detected during the surveillance programme involving CT scans (n=74), echo guided biopsy (n=60), and charges for treatments—PEI (n=14), hepatic resection (n=4), OLT (n=6) and both diagnostic and therapeutic TACE (total n=51)—resulted in a total charge for the surveillance programme of US$753 226 (table 5).
Charges and cost effectiveness analysis of the surveillance programme (US$)
The cost of treatable HCC was US$17 934 for the surveilled and US$14 555 for the unsurveilled patients (Δ=US$3379) (table 5), resulting in an incremental cost in the surveilled group of US$141 918. Comparison of survival of patients with HCC detected during the surveillance programme (median survival 30 months) with that of patients with HCC detected incidentally in the unsurveilled population (median survival 15 months) showed a cost per year of life saved of US$112 996. This estimate, however, does not take into account other incidental costs such as clinic visits, doctors' time, other costs related to hospitalisation, time lost in employment, and travel costs, which further increase the cost of surveillance. Furthermore, it does not take into account the unknown cost in the unsurveilled population (where US and other diagnostic tests, apart from those performed at the time of detection, were randomly performed prior to our observation) whose inclusion in the analysis would improve the cost effectiveness of the programme.
Discussion
Screening and surveillance programmes based on new imaging modalities can produce a cycle of increasing diagnostic and therapeutic intervention without any definite advantage.22 The clinical effectiveness of these programmes relies on the establishment of early diagnosis, provided that effective treatments are available. As a consequence, an increased proportion of successful treatments and a reduction in disease specific mortality of surveilled patients should be the final result.
The problem is particularly important in screening for neoplasms arising in diseased organs and in aged patients, as is the case for HCC. This implies that cancer eradication (if possible) would possibly not significantly affect patient survival.
Unfortunately, these points have been only partially addressed in previous studies on the problem of screening or surveying cirrhotics for HCC.2-15 ,23 A randomised study on the potential benefit of surveillance programmes comparing survival in surveilled and unsurveilled patients has never been done and at present it is unrealistic and could even be considered unethical, at least in developed countries where the use of US examinations in patients with liver disease is widespread.
In the present study we tried to address this problem, and in addition to the incidence of HCC in a western population we investigated objective measures of effectiveness of a surveillance programme, such as the morphological characteristics of HCC detected during follow up, eligibility for surgical and local treatment, and disease outcome in terms of survival. We then compared these measures with those obtained in HCC incidentally detected outside any specific surveillance programme (non-randomised contemporaneous controls) during the same period of enrollment. Finally, we analysed and reported the costs of the programme in relation to outcome in order to provide data useful for setting priorities in allocating resources.24 The choice of an adequate control group is critical for any study. In our series the volume of unifocal tumours was not significantly different (table 4) between surveilled patients and controls and tumour volume of our controls was smaller than that of other series published recently,25 which included, however, multifocal tumours with clinical symptoms. This fact may support the hypothesis that the same control patients had undergone periodic examinations for their liver disease outside of regular surveillance programmes, a practice that was spreading in Italy at the beginning of the 1990s. On the other hand, the rate of unifocal and diffuse/infiltrating tumours (table 4) between the two groups already favours the efficacy of our surveillance policy, even though the extent of this gain is related to our specific control group.
A critical point for the evaluation of cost effectiveness is the proportion of patients with tumours detected during the surveillance programme who are eligible for surgical or local treatment. In our series only 42 of 61 detected cases (68.8%) were treated, a proportion not significantly different from that of the unsurveilled population (58%) who, however, could have been previously selected. Our proportion of treated patients is particularly high if compared with that of Colombo and colleagues9 (only 14% of HCC detected during follow up and 43% of HCC found at entry were operable), Pateron and colleagues12 (28.6%), and Cottone and colleagues13 (33.3%), but is lower than that reported by Oka and colleagues8 (82.5%). This discrepancy is partially apparent if we consider that Colombo et al evaluated only operable cases, while we and Oka and colleagues8 evaluated the various types of local or surgical treatment. Only 6.5% of cases in our study and 17.5% in the study of Oka and colleagues8 underwent hepatic resection.
Our cumulative three year survival rate for patients with HCC detected during the surveillance programme was significantly higher (p=2) than that of unsurveilled patients (fig 3) and proved similar (45%) to that reported by Oka and colleagues8 (41%). These values are much higher than those reported in the majority of previous studies on the natural history of unselected series of HCC.25-29 A more recent study30 in patients derived from a prospective randomised trial showed a higher three year survival (50%) but only in patients without adverse factors; this was not the case in our series. Such differences could represent lead time bias or may be due to over diagnosis,22 but this bias seems unavoidable and is further confirmed by the presence of more multifocal disease in unsurveilled patients. The problem of over diagnosis is particularly important from a clinical point of view and surprisingly it has rarely been reported in previous studies on surveillance. If not correctly interpreted, this condition could seriously affect the assessment of outcome measures. In our study, in 13 of 74 detected nodules (17.1%) malignancy was not proved and four of the 61 true HCC were classified as macroregenerative nodules prior to the definite diagnosis or their evolution into HCC. This demonstrates that surveillance discloses quite a large number of nodules of uncertain malignant potential31 causing increasing diagnostic and therapeutic intervention without any demonstration of efficacy, as the natural history of this condition is largely unknown.
Another point which has been poorly analysed in previous studies on screening for HCC is cost, and data on this are scarce. Sarasin and colleagues32 recently evaluated the theoretical costs of screening using a decision analysis model but they considered hepatic resection as the only therapeutic option for HCC. Furthermore, even though we believe that theoretical models may have some advantages due to their flexibility, they depend on information derived from different sources and therefore must always be tested and compared with the results obtained in current clinical practice, as in our study. Actual measurement of costs is a major area of methodological inconsistency in cost effectiveness analysis. We adopted the calculation of charges33 because it is the only objective parameter available and comparable in different countries. Therefore, the economic issues reported in this study are based on charges for diagnostic and interventional procedures at our university hospital. As the number of procedures performed is always indicated, readers can easily calculate corresponding charges for their own country. The analysis showed that the cost per year of life saved was US$113 534. This does not represent an exact incremental cost effectiveness ratio21 but it offers an idea of the expenditure requested. Cost utility of the programme has not been measured but it is conceivable that screening procedures do not significantly affect quality of life.
Our results demonstrate that a surveillance programme of patients with LC requires a large number of resources and its implementation in clinical practice on a national basis would be questionable in many countries. This conclusion can be understood if we consider that costs for the screening of breast cancer are estimated at US$13 000–28 000 per year of life saved and still cause debate.34Implementation of any screening programme in the daily practice of each country also requires that such programmes do not consume resources out of proportion of the importance of the disease (prevalence, socioeconomic impact, etc) in the country. Therefore, adoption of screening policies can be different between countries.35However, according to a recent article providing a new perspective in evaluation gains in life expectancy from medical interventions,36 a gain of a year from a preventive intervention targeted at populations with elevated risk similar to what we observed in our study can be considered large.
Finally, it is important to outline that a small proportion of cirrhotic patients seemed to benefit from the surveillance programme (for instance, those transplanted with HCC at a very early stage and not recurring whose life would not have been saved without an early diagnosis). This must stimulate the search for definite individual risk factors or morphological predictors of HCC, such as liver cell dysplasia37 and AgNors quantitation,38allowing for a more targeted surveillance and consequently better cost effectiveness.
Acknowledgments
This research was supported by grants ex-40% and 60% of MURST (Italian Ministry for Technological and Scientific Research).
Abbreviations used in this paper
- AFP
- α fetoprotein
- CT
- computed tomography
- HCC
- hepatocellular carcinoma
- LC
- liver cirrhosis
- OLT
- orthotopic liver transplantation
- PEI
- percutaneous ethanol injection
- TACE
- transarterial chemoembolisation
- US
- ultrasonography
References
Footnotes
↵† M Zanetti died on 22 April, 2000.