Article Text

Abstract
BACKGROUND A high prevalence of osteoporosis is reported in Crohn's disease. The pathogenesis is not completely understood but is probably multifactorial. Longstanding Crohn's disease is associated with a deficiency of fat soluble vitamins, among them vitamin K. Vitamin K is a cofactor in the carboxylation of osteocalcin, a protein essential for calcium binding to bone. A high level of circulating uncarboxylated osteocalcin is a sensitive marker of vitamin K deficiency.
AIMS To determine serum and bone vitamin K status in patients with Crohn's disease and to elucidate its relationship with bone mineral density.
METHODS Bone mineral density was measured in 32 patients with longstanding Crohn's disease and small bowel involvement, currently in remission, and receiving less than 5 mg of prednisolone daily. Serum levels of vitamins D and K, triglycerides, and total immunoreactive osteocalcin, as well as uncarboxylated osteocalcin (“free” osteocalcin) were determined. The hydroxyapatite binding capacity of osteocalcin was calculated. Data were compared with an age and sex matched control population.
RESULTS Serum vitamin K levels of CD patients were significantly decreased compared with normal controls (p<0.01). “Free” osteocalcin was higher and hydroxyapatite binding capacity of circulating osteocalcin was lower than in matched controls (p<0.05 and p<0.001, respectively), indicating a low bone vitamin K status in Crohn's disease. In patients, an inverse correlation was found between “free” osteocalcin and lumbar spine bone mineral density (r=−0.375, p<0.05) and between “free” osteocalcin and the z score of the lumbar spine (r=−0.381, p<0.05). Multiple linear regression analysis showed that “free” osteocalcin was an independent risk factor for low bone mineral density of the lumbar spine whereas serum vitamin D was not.
CONCLUSIONS The finding that a poor vitamin K status is associated with low bone mineral density in longstanding Crohn's disease may have implications for the prevention and treatment of osteoporosis in this disorder.
- Crohn's disease
- bone mineral density
- vitamin K
- osteocalcin
Abbreviations used in this paper
- BMD
- bone mineral density
- BMI
- body mass index
- CD
- Crohn's disease
- CDAI
- Crohn's disease activity index
- Gla
- gamma carboxyglutamate
- Glu
- glutamic acid
- HBC
- hydroxyapatite binding capacity
- OC
- osteocalcin
- OCBOUND
- bound osteocalcin (carboxylated)
- OCFREE
- free osteocalcin (uncarboxylated)
- OCTOTAL
- total osteocalcin
Statistics from Altmetric.com
A high prevalence of osteopenia and osteoporosis is reported in Crohn's disease (CD).1-9 The pathogenesis of low bone mineral density (BMD) in CD is multifactorial. Important factors are disease activity, corticosteroid use, hypogonadism, and nutritional depletion.10 ,11 The latter includes malabsorption of fat soluble vitamins, especially in patients with ileal involvement, and has been proved for vitamin D.12 ,13
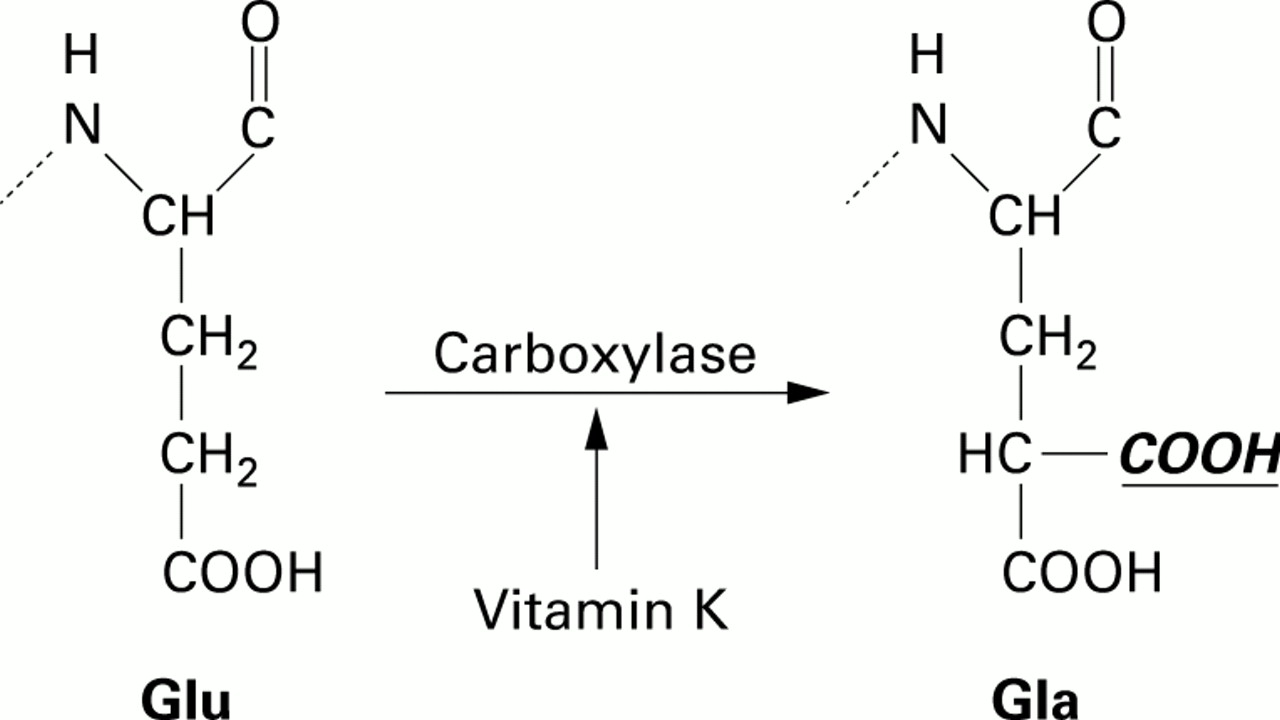
Bone is a living organ with a continuous process of remodelling, consisting of bone resorption by osteoclasts and bone formation by osteoblasts. Osteoblasts need vitamin K as a cofactor for post-translational carboxylation of protein bound glutamate (Glu) residues into gamma carboxyglutamate (Gla) (fig 1). During bone formation, osteoblasts produce three Gla proteins: osteocalcin (OC), matrix Gla protein, and protein S. OC and matrix Gla protein have a regulatory role in the mineralisation and remodelling of bone, whereas the function of protein S in bone metabolism remains unclear. Precursors of all three Gla proteins contain a sequence that serves as a recognition signal for vitamin K dependent carboxylase. Carboxylation renders the proteins capable of binding to calcium.14-16Osteocalcin can have three Gla residues but it is not known how many carboxyl groups are needed for adequate function. Circulating Gla proteins provide information on vitamin K status of bone. Under conditions of subclinical vitamin K deficiency, OC remains uncarboxylated and is transferred into the circulation. In this paper, uncarboxylated osteocalcin is referred to as “free “ osteocalcin (OCFREE).
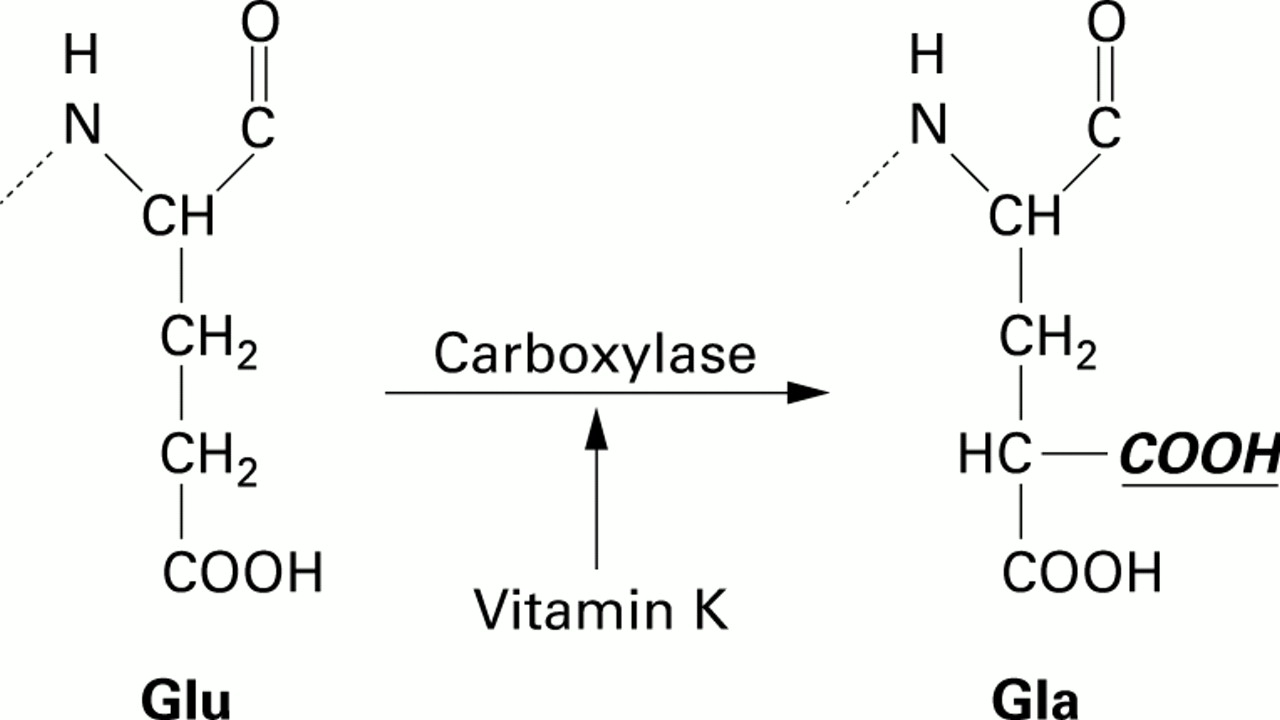
Schematic representation of the vitamin K dependent carboxylation reaction. Reduced vitamin K acts as a cofactor in the carboxylation of glutamic acid residues (Glu) into gamma carboxylation acid residues (Gla). These residues render the protein osteocalcin capable of calcium binding to bone.
Several studies have reported evidence of a relation between vitamin K status and bone mineralisation. Low serum concentrations of vitamin K have been reported in patients with osteoporotic fractures.14 Higher concentrations of uncarboxylated OC have been shown to be related to advanced age, low BMD, and the risk of hip fracture.14 Loss of bone mass was associated with poor vitamin K status in postmenopausal women.15 Oral anticoagulant therapy was associated with an increased risk of fracture.17 Vitamin K supplementation decreases bone loss and calcium excretion.14
The aim of this study was to investigate serum and bone vitamin K status in patients with longstanding CD and to elucidate the relation between vitamin K status and BMD in these patients. Furthermore, the relationship between vitamin K status and serum concentrations of vitamin D and triglycerides was established.
Methods
PATIENTS
Patients were randomly asked to participate in the study while attending the gastroenterology outpatient clinic of the University Hospital of Maastricht. Thirty three patients with CD (13 males, 20 females) were included in the study in April and May 1997. Characteristics of the patient population are given in table1.
Characteristics of patients with Crohn's disease (n=32) compared with age and sex matched healthy controls (n=34)
CD was diagnosed by clinical findings and a combination of radiology, endoscopy, and histology for which the Lennard-Jones criteria were applied.18 At the time of the study all patients were in clinical remission. Disease activity was measured using the Crohn's disease activity index (CDAI).19 All patients had small bowel involvement and 13 patients also had inflammation of the colon. In 24 patients an ileal resection had been performed. All patients were using mesalazine (5-aminosalicylic acid). Four patients were receiving prednisolone or a steroid equivalent; however, for inclusion, the prednisolone equivalent dose had to be less than 5 mg/day. Six patients were taking vitamin D supplements (400 IU /day) and four also used calcium supplements (500 mg/day). Six female patients were postmenopausal; none was receiving hormone replacement therapy. Five other women were taking oral contraceptive medications. At the time of inclusion, 14 patients were regular cigarette smokers. Body mass index (kg/m2) was calculated. One female patient, who had been taking vitamin K supplements, was excluded during the course of the study. The study protocol was approved by the ethics committee of the University Hospital of Maastricht and all patients gave informed consent before the start of the study.
BIOCHEMICAL MEASUREMENTS
Total OC was measured using the Osteometer test kit (Biotech, Herlev, Denmark). Since carboxylated OC and uncarboxylated OC differ substantially in their affinity for insoluble calcium salts, these fractions can be quantified by measuring serum OC before and after extraction with a standard amount of hydroxyapatite. The fraction which does not bind to hydroxyapatite consists of uncarboxylated “free” osteocalcin (OCFREE). To measure the OCFREEfraction, 45 mg of hydroxyapatite were added to 300 μl of serum. The fraction of carboxylated OC (OCBOUND) is calculated from the difference between the total immunoreactive OC (OCTOTAL) and OCFREE. OCBOUNDexpressed as a percentage of total OC is known as the hydroxyapatite binding capacity (HBC) of osteocalcin.16 The percentage HBC of circulating OC was calculated using the formula: HBC (%)=((OCTOTAL−OCFREE)/OCTOTAL) ×100. OC levels and HBC (%) were compared with those of an age and sex matched control group of 34 healthy men and women.20 ,21
Vitamin K was assessed using a HPLC technique with post-column reduction and fluorescence detection, as previously described.22 Serum vitamin K levels in patients were compared with those of a reference population of 384 healthy men and women. Serum 25-hydroxyvitamin D concentration was measured using a125 I radioactive immunoassay (Incstarr Corporation-Stillwater, Minnesota, USA) in specimens obtained in April and May for which the winter reference value was applied (25–70 nmol/l).23
BONE MINERAL DENSITY
BMD was measured using dual energy xray absorptiometry (DXA; Lunar DPX-L, Lunar software version DPX-L 4.7; Lunar Radiation Corp., Madison, Wisconsin, USA) of the lumbar spine (L2–L4), femoral neck, and total body.24 BMD was expressed in absolute values (g/cm2), T scores (one SD of the mean of a young adult sex matched reference population), and z scores (one SD of the mean of an age and sex matched reference population), respectively. Reference data were based on populations from the USA, UK, and Northern Europe. There was 1.3% SD of the average density values of populations contributing to normative data in the various geographical areas. The prevalence of osteopenia and osteoporosis was assessed according to the WHO classification in which osteopenia is defined as a T score between −1 and −2.5 and osteoporosis as T <−2.5.25
STATISTICAL ANALYSIS
Results are shown as mean (SD). The (unpaired) independentt test was used for comparison of CD patients with the reference population for serum vitamin K concentration, OCFREE, and HBC (%). One way ANOVA was used to evaluate vitamin K status in CD patients with either normal BMD or osteopenia and osteoporosis. Non-parametric tests were used for the remaining statistical evaluations. Correlations between continuous variables were assessed using Pearson's correlation coefficient. Multiple linear regression analysis was performed to identify independent risk factors for BMD and to correct for vitamin D deficiency as a potential confounder. The following independent variables were used separately in this analysis: absolute BMD, T score, and z score of the femoral neck, lumbar spine, and total body, respectively. Two tailed tests for significance were used in all statistical analyses. A p value <0.05 was considered statistically significant. The Statistical Package for the Social Sciences (SPSS 7.5 for windows package 1996, SPSS inc., Chicago, Illinois, USA) was used for the analysis.
Results
Mean BMD, expressed as absolute values in g/cm2, of the femoral neck, lumbar spine, and total body were 0.89 (0.13), 1.10 (0.16), and 1.11 (0.09), respectively. Mean T scores were −0.61 (1.29) for the total body, −0.98 (1.16) for the femoral neck, and −0.66 (1.13) for the lumbar spine. Mean z scores were −0.49 (1.07) for the total body, −0.45 (1.25) for the femoral neck, and −0.28 (1.10) for the lumbar spine. The prevalence of osteopenia and osteoporosis in these patients according to the WHO definition is given in table 2.
Prevalence of osteoporosis and osteopenia in patients with longstanding Crohn's disease (n=32), according to the WHO definition
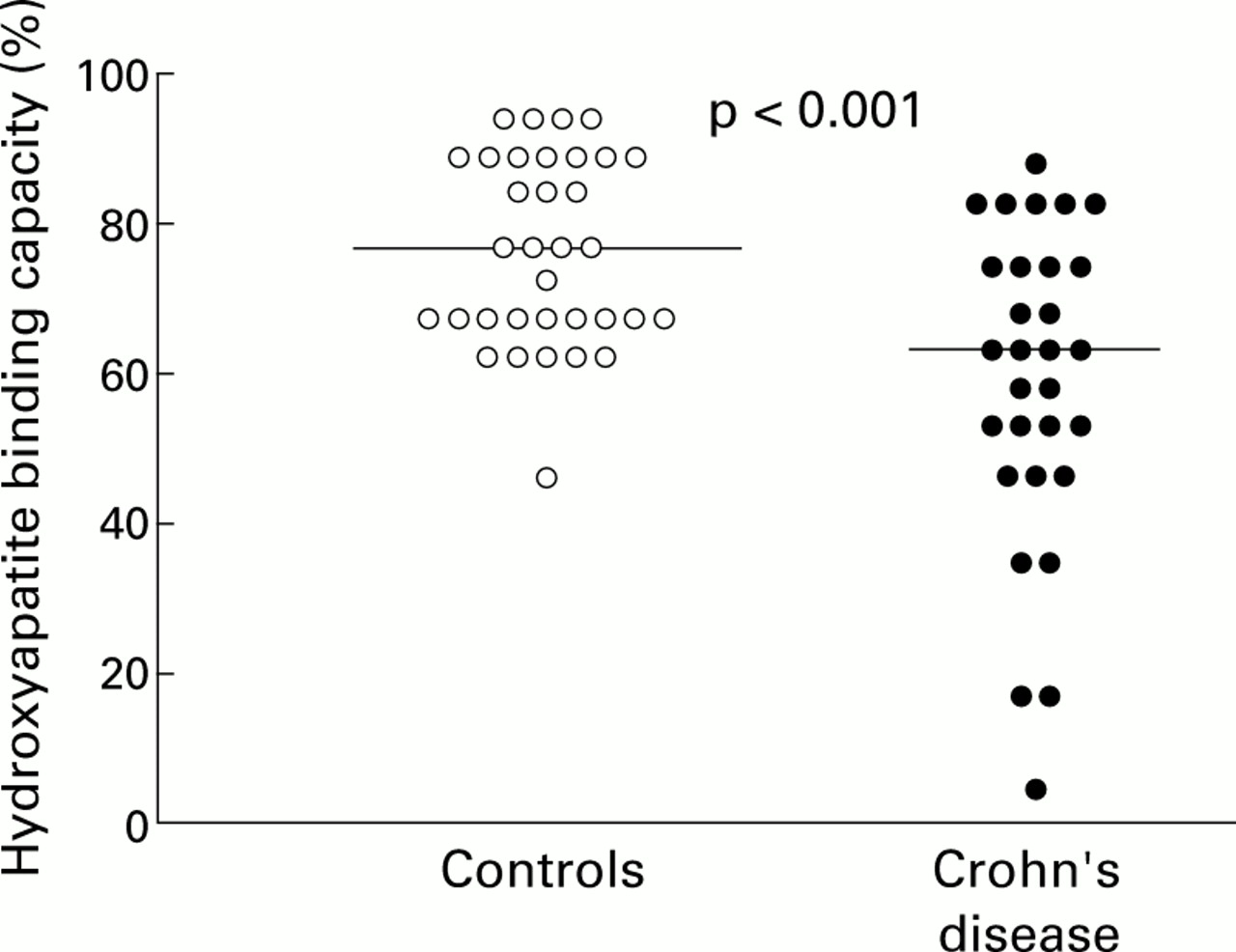
Serum vitamin K concentrations in patients with CD were significantly lower than in a reference population of 384 healthy men and women (p<0.01) (fig 2). Patients with CD had higher serum OCFREE(p<0.05) and lower HBC values (p<0.001) compared with values obtained from the age and sex matched control group of 34 healthy men and women randomly selected from the community registry (figs 3, 4). Serum vitamin K, OCFREE, and HBC did not differ significantly between male and female patients. Although mean OCFREE was generally lower and mean serum vitamin K was higher in patients with normal BMD than in patients with a T score <−1 (osteopenia plus osteoporosis), this difference was not statistically significant. In patients, a negative correlation was found between lumbar spine BMD and OCFREE (r=−0.375, p<0.05) (fig 5) and between lumbar spine z score and OCFREE(r=−0.381, p<0.01) (fig 6).

Serum vitamin K concentrations in patients with longstanding Crohn's disease (n=32) compared with healthy controls (n=34). Median for patients with Crohn's disease is 0.402 ng/ml; median for healthy controls is 0.610 ng/ml.

Serum concentrations of “free” (uncarboxylated) osteocalcin in patients with longstanding Crohn's disease (n=32) compared with age and sex matched healthy controls (n=34). Lines indicate median values. Median for patients with Crohn's disease is 3.89 ng/ml; median for healthy controls is 1.51 ng/ml.

Hydroxyapatite binding capacity in patients with longstanding Crohn's disease (n=32) compared with age and sex matched healthy controls (n=34). Lines indicate median values. Median for patients with Crohn's disease is 61.71%; median for healthy controls is 76.84%.

Correlation between “free” (uncarboxylated) osteocalcin and bone mineral density (BMD) of the lumbar spine in patients with longstanding Crohn's disease (n=32). Correlation coefficient (Pearson's) r=−0.375; p<0.05.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of “free” (uncarboxylated) osteocalcin and bone mineral density z score of the lumbar spine in patients with longstanding Crohn's disease (n=32). Correlation coefficient (Pearson's) r=−0.381; p<0.01.
Mean serum level of vitamin D in patients was 28.4 (10.5) nmol/l; 11 patients (34%) were vitamin D deficient (serum 25-hydroxy vitamin D <25 nmol/l). Of patients taking a vitamin D supplement (400 IU/day for more than two months), three patients still had serum vitamin D levels <25 nmol/l (13, 14, and 23 nmol/l, respectively). A significant correlation was found between serum concentrations of vitamin D and K (r=0.681, p<0.01). No correlation was found between concentrations of vitamin D and vitamin K status of bone (either OCFREE or HBC (%)). Mean serum triglyceride level was 1.5 (1.1) mmol/l. A positive correlation was found between serum concentrations of vitamin D and triglycerides (r=0.707, p<0.01) and vitamin K and triglycerides (r=0.789, p<0.01), respectively.
In the patient group, the variables sex, age, body mass index, serum vitamin K, OCFREE, and vitamin D were included in a multiple linear regression. No correlations were found between serum vitamin K levels and BMD, or T and z scores at any measurement site. We found that OCFREE correlated significantly with BMD of the lumbar spine (p=0.05) and with the lumbar spine z score (p=0.035) (table 3). The correlation between OCFREE and the T score of the lumbar spine did not reach significance (p=0.091). No correlations were found between BMD, T and z scores of the femoral neck and total body, and OCFREE. No correlations were found between serum vitamin D levels and BMD, or T and z scores at any measurement site.
Results of multiple linear regression analysis in patients with longstanding Crohn's disease (n=32), with absolute bone mineral density (BMD) and z scores of the lumbar spine as dependent, and vitamin D and “free” (uncarboxylated) osteocalcin as independent variables
Discussion
The results of the study reveal low serum vitamin K and low bone vitamin K status (increased OCFREE and lowered HBC (%)) in a group of patients with longstanding CD compared with normal controls. Serum OCFREE status, but not serum vitamin K concentration, correlated with BMD of the lumbar spine.
To exclude the effects of disease activity and corticosteroid use, we investigated a group of patients with inactive CD, all with small bowel involvement, and/or a previous ileal resection. They were receiving no or very low doses of steroids. In some patients with ileal resection, CDAI scores were relatively high, in spite of clinical remission. The index obviously reflects high frequency of liquid stools in these patients due to ileal resection rather than current intestinal inflammation.
In patients with CD and ileopathy, caused by either inflammation or previous resection, bile acid and fat malabsorption causes steatorrhoea and malabsorption of fat soluble vitamins. Serum vitamin K concentrations are influenced by plasma triglyceride concentrations and reflect recent dietary intake in healthy subjects.16 ,26While there are several publications on the role of vitamin D in metabolic bone disease in CD,1 ,13 ,27-30 only few data are available with regard to vitamin K status in CD. In a study in which uncarboxylated prothrombin was used as a marker, vitamin K deficiency was identified in 46% of CD patients with ileal involvement but not in patients with Crohn's colitis.31 It has also been reported that OCFREE, as used in the present study, is a much more sensitive marker for vitamin K status than prothrombin.32
The fact that vitamin K serves as a cofactor for carboxylation of bone Gla proteins and is of potential importance for bone formation is reflected by a significant independent and inverse correlation between OCFREE and BMD of the lumbar spine (BMD and z score). The trabecular bone of the spine is metabolically more active than the cortical bone of the hip and may thus be more susceptible to vitamin K deficiency. This may explain the lack of correlation between OCFREE and BMD of the femoral neck and total body. Surprisingly, no correlation was found between HBC (%) and BMD at any site. This finding could indicate that the absolute amount of circulating uncarboxylated osteocalcin (OCFREE) is more indicative of a low bone vitamin K status than the fraction of OCBOUND expressed by HBC (%).
Bone mineral loss in CD is a multifactorial process and vitamin K deficiency is certainly only one factor in this process. In the present study there are indications that in patients with longstanding CD, vitamin K deficiency of bone has a greater influence on BMD than serum 25-hydroxy vitamin D levels. The body vitamin D stores are reflected by serum concentrations of 25-hydroxy vitamin D. In accordance with our expectations, significant correlations between serum vitamin D and K concentrations and triglycerides were found. In the present study, however, patients who were vitamin D deficient did not have significantly decreased BMD. Published data are equivocal in this respect: a significant correlation between vitamin D and BMD of the forearm was found in one of three large studies on vitamin D deficiency and BMD in patients with CD.27-29 Vitamin D deficiency may cause secondary hyperparathyroidism which predominantly affects cortical bone.
The questions remaining are whether or not bone that is vitamin K deficient is rendered sensitive to other pathogenetic factors of osteoporosis, such as corticosteroids, and whether vitamin K supplementation can improve bone mineralisation in CD patients, as has been demonstrated in other conditions. In prednisolone treated rats, vitamin K supplementation inhibited bone loss.33 Treatment with vitamin K (menatetrenone) has been reported to increase BMD in disused bones in vitamin K and D deficient hemiplegic patients.34 In a study in cystic fibrosis patients, a significantly elevated level of OCFREE was found in patients who were not supplemented with vitamin K (phylloquinone) versus supplemented patients.35 The questions addressed above require further study. It has recently been demonstrated that vitamin K treatment effectively prevents the occurrence of new vertebral fractures in patients with osteoporosis.36
In summary, low serum and bone vitamin K status was found in patients with longstanding CD, currently in remission. The poor vitamin K status correlated with low lumbar spine BMD. Circulating uncarboxylated osteocalcin in particular was found to be an independent risk factor of low BMD of the lumbar spine in these patients whereas low serum vitamin D was not. Further studies are needed to assess the implications of low serum and bone vitamin K status and the value of vitamin K supplementation for the prevention of osteoporosis in CD.
Abbreviations used in this paper
- BMD
- bone mineral density
- BMI
- body mass index
- CD
- Crohn's disease
- CDAI
- Crohn's disease activity index
- Gla
- gamma carboxyglutamate
- Glu
- glutamic acid
- HBC
- hydroxyapatite binding capacity
- OC
- osteocalcin
- OCBOUND
- bound osteocalcin (carboxylated)
- OCFREE
- free osteocalcin (uncarboxylated)
- OCTOTAL
- total osteocalcin
References
Linked Articles
- Commentary