Article Text

Abstract
BACKGROUND Although antisecretory medications such as histamine type II receptor antagonists or proton pump inhibitors have been used to treat reflux oesophagitis, a considerable number of patients do not achieve complete mucosal healing or suffer from either sustained symptoms or ensuing complications, suggesting other damaging factors or impaired mucosal resistance are also involved in the pathogenesis of reflux oesophagitis.
AIMS The present study was designed to evaluate oxidative stress as the major pathogenic factor of reflux oesophagitis and to determine the usefulness of antioxidants in the treatment of reflux oesophagitis.
MATERIALS AND METHODS Reflux oesophagitis was induced by insertion of a 3 mm calibre ring into the duodenum, 1 cm distal to the ligament of Treitz, in Sprague-Dawley rats.
RESULTS DA-9601, a novel antioxidant substance, significantly attenuated the gross and histopathological scores of reflux oesophagitis compared with those treated with ranitidine alone or reflux oesophagitis controls in a dose dependent manner. Only scattered erosions were observed in the antioxidant pretreated group but acid suppression by ranitidine was not effective in decreasing the severity of reflux oesophagitis. Significantly increased amounts of malondialdehyde (MDA), increased nuclear factor κB (NFκB) activation, and depletion of reduced glutathione (GSH) were observed in experimentally induced reflux oesophagitis. DA-9601 pretreatment attenuated the decrement in mucosal GSH levels and decreased MDA formation significantly. DA-9601 treatment caused significant reductions in activation of NFκB transcription factor, especially the p50 subunit, in accordance with the significantly higher levels of inhibitory protein of NFκB expression.
CONCLUSION Reflux oesophagitis caused considerable levels of oxidative stress in the oesophageal mucosa and antioxidant treatment should be considered as supplementary therapy in the prevention or treatment of reflux oesophagitis with acid suppression.
- reflux oesophagitis
- antioxidants
- oxidative stress
- rat
Abbreviations used in this paper
- NFκB
- nuclear factor κB
- IκBα
- inhibitory protein of NHκB
- H2-RA
- histamine H2 receptor antagonist
- MDA
- malondialdehyde
- GSH
- reduced glutathione
- PMSF
- phenylmethylsulphonyl fluoride
- NP-40
- Nonidet P-40
- EMSA
- electrophoretic mobility shift assay
- SDS
- sodium dodecyl sulphate
- HAI
- histological activity index
- MPO
- myeloperoxidase
- PPI
- proton pump inhibitors
Statistics from Altmetric.com
Reflux oesophagitis is a common disease entity in which gastric juice gains access to the oesophagus via an incompetent lower oesophageal sphincter.1 The presence of refluxed materials induces different grades of oesophageal damage ranging from low to high grade oesophagitis.2 Some pathological conditions in the lower oesophagus, including erosions, stenosis, ulcer, or metaplastic epithelium are considered complications of chronic reflux oesophagitis.3 ,4 It is generally believed that reflux of gastric contents causes inflammation, ulceration, and destruction of the normal squamous epithelium of the oesophagus.5 However, the exact pathophysiological mechanisms of oesophageal cell damage during gastro-oesophageal reflux are not fully explained by acid reflux alone.
Although lesions induced by acid and pepsin in the rabbit mimicked human reflux oesophagitis, the fact that a relatively short period of contact of the acid in the oesophageal mucosa does not allow the development of the more complex potential mechanisms of oesophageal defence, and the degree of damage does not completely correlate with the amount of refluxed materials, suggests other contributing mechanisms in reflux oesophagitis.6 Therefore, the severity of reflux oesophagitis cannot be accurately predicted simply on the basis of acid exposure and other damaging factors need to be considered. Also, impaired mucosal resistance may be involved in the pathogenesis of reflux oesophagitis.7 ,8
In recent studies it has been shown that mucosal damage in reflux oesophagitis is mediated primarily by oxygen derived free radicals.9 ,10 The role of oxygen derived free radicals has been studied in acute gastric and oesophageal mucosal injury caused by ischaemia, anti-inflammatory drugs such as non-steroidal anti-inflammatory agents, and ethanol. Administration of various free radical scavengers has been found to prevent oesophageal mucosal damage.11 DA-9601, an ethanol extract ofArtemisia asiatica, was reported to have antioxidative and cytoprotective actions in various models of gastric mucosal damage in experimentally induced colitis. This new antioxidative drug scavenged the superoxide and hydroxyl radicals which lessened the severity of trinitobenzoic acid induced colitis.12 ,13 DA-9601 was also reported to be effective in attenuating cerulein induced pancreatitis through reduction of lipid peroxidation and induction of apoptosis in damaged pancreatic acinar cells.14
Here, we investigated if blockade of acid or administration of an antioxidant attenuated the severity of experimentally induced reflux oesophagitis in a rat model and which method (acid suppression or antioxidant) was more effective in decreasing mucosal damage from reflux oesophagitis. To prove that oxygen derived free radicals play an important role in reflux oesophagitis, oxygen derived free radical mediated nuclear factor κB (NFκB) activation was studied. NKκB is a dimeric transcription factor involved in the regulation of a large number of genes that control various aspects of the immune and inflammatory response. It is activated by a variety of stimuli ranging from cytokines and various forms of radiation, to oxidative stress.15
Materials and methods
GENERATION OF REFLUX OESOPHAGITIS IN RATS
Eight week old male Sprague-Dawley rats with a body weight of about 200 g were used for the experiments. Rats were starved for 24 hours before the experiments but were allowed free access to water. Experiments were carried out under general anaesthesia which was induced by intramuscular injection of ketamine hydrochloride (20 mg/100 g body weight). In 60 rats duodenogastro-oesophageal reflux was caused by insertion of a 3 mm diameter ring into the fourth portion of the duodenum, 1 cm distal to the ligament of Treitz. A longitudinal cardiomyotomy was also performed to enhance gastric reflux into the oesophagus. The vagus nerves were left intact. Sixty operated rats were divided into four groups of 15 rats each. In group II (reflux oesophagitis control group), no further treatment was performed in addition to the above surgical procedure. However, all other groups (III, IV, and V) were additionally treated with either antioxidant or H2 receptor antagonist (H2-RA); group III was pretreated with DA-9601 30 mg/kg orally, group IV with DA-9601 100 mg/kg orally, and group V with ranitidine hydrochloride (Zantac; GlaxoWellcome, UK) 10 mg/kg orally. All drugs were administered 30 minutes before the surgical procedure. Fifteen additional rats were subjected to a sham operation and served as a normal control group (group I). The sham operation involved a midline laparotomy alone. All five groups of rats were starved of food for 36 hours after surgery but had free access to water. After 36 hours the rats were sacrificed and the entire oesophagus was removed and examined for gross and microscopic mucosal injury. The oesophageal mucosa was stripped of the muscle layer, frozen in liquid nitrogen, and stored at −70°C for the following biochemical assays.
BARIUM STUDY
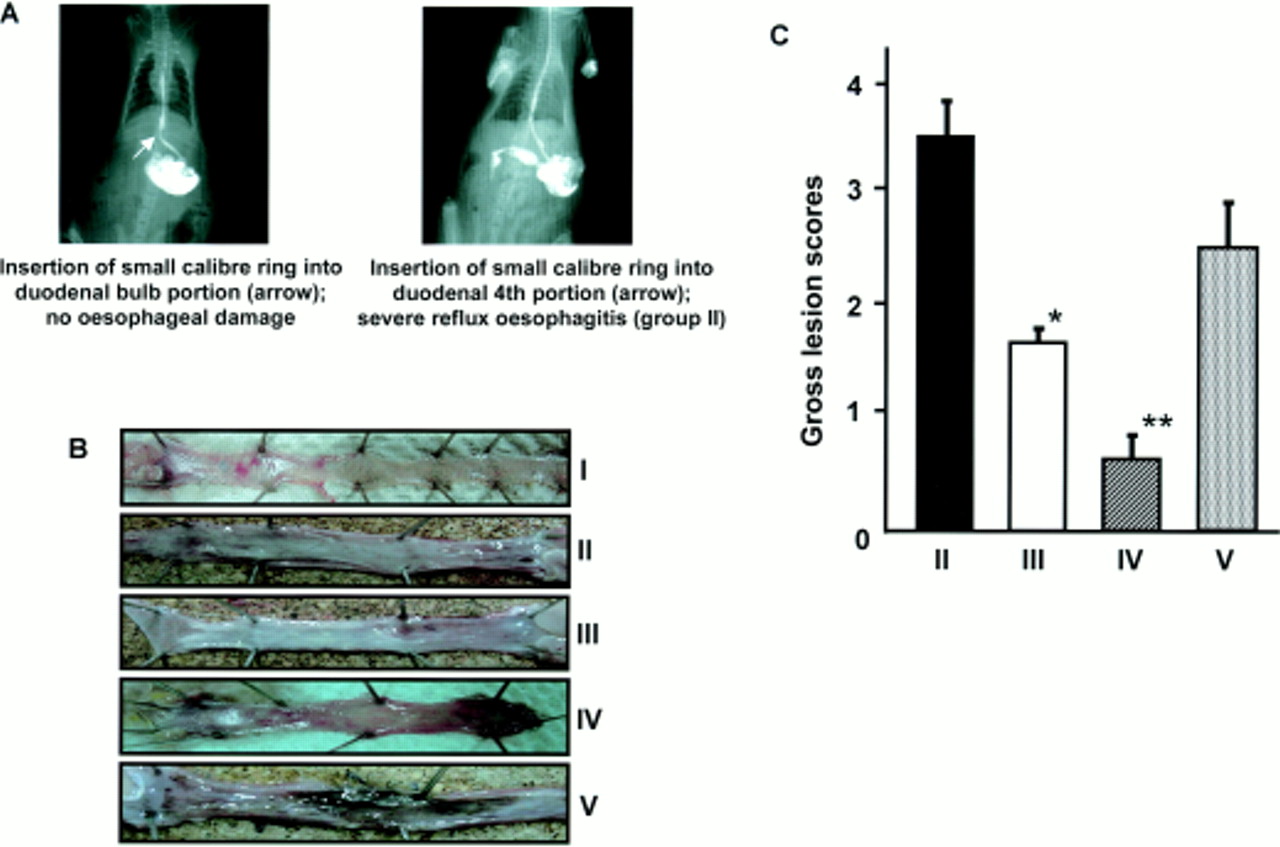
To confirm the effectiveness of surgery in narrowing the diameter of the duodenum, facilitating reflux of mixed contents, barium studies were performed using contrast media containing barium phosphate under fluoroscopic guidance (fig 1A).

(A) Generation of reflux oesophagitis in the rat oesophagus according to the surgical method. No significant reflux oesophagitis was observed in the group in whom a small calibre ring, 3 mm in diameter, was inserted into the duodenal bulb whereas a considerable degree of reflux oesophagitis was effectively generated in the group where the 3 mm small calibre ring was inserted into the duodenum, distal to the Treitz ligament, suggesting mixed reflux could provoke reflux oesophagitis rather than acid reflux alone in rats. (B, C) Gross appearance of the total oesophagus in each group. Multiple linear ulcerations were observed in the reflux oesophagitis control group (group II). In the DA-9601 pretreated groups (III and IV), only scattered haemorrhagic spots or focal erythematous lesions were observed in the oesophageal mucosa. Ranitidine alone (group V) was not effective in decreasing reflux oesophagitis. Group I, sham operated group. *p<0.05, **p<0.01 versus group II.
MACROSCOPIC AND MICROSCOPIC EXAMINATION
The oesophagus was opened, gently rinsed with 0.9% NaCl, and photographs were taken of specific areas of damage under a dissecting microscope with a magnification of ×3. Gross lesions were scored as follows: normal glistening mucosal appearance (score 0); oedematous mucosa with focal haemorrhagic spots (score 1); multiple erosions with haematins attached (score 2); linear ulcerations with yellowish exudates (score 3); and haemorrhagic coalesced ulcerations (score 4). The entire area of damage was then fixed in 10% formalin for histological evaluation. The degrees of epithelial loss (splitting, erosion, ulceration), regenerative epithelial changes (basal hyperplasia, mitosis, balloon cells, akantosis, parakeratosis), vascular alterations (oedema, congestion, bleeding, vessel lesions), and inflammation (polymorphonuclear leucocytes, lymphocytes, eosinophils, intensity, and extension) were determined and scored as reported previously.3
BIOCHEMICAL ASSAYS OF OESOPHAGEAL MUCOSA
When oxygen derived free radicals are generated in excess of the capability of the scavenging system, cells can be damaged by peroxidising lipids. Malondialdehyde (MDA), an index of lipid peroxidation, was determined according to the method of Buege and Aust,16 measuring spectrophotometrically the formation of thiobarbituric acid reactive substances. Glutathione (GSH) levels, which reflect the cellular redox status, were measured according to the manufacturer's instructions (Bioxytech GSH-400 assay; Oxis International, Inc., Portland, Oregon, USA). Quantitation was done using reduced GSH purchased from Sigma (St Louis, Missouri, USA).
ELECTROPHORETIC MOBILITY SHIFT ASSAY (EMSA) AND SUPERSHIFT EMSA ASSAY
Nuclear proteins were extracted from tissues of groups I, II, III, IV, and V. Each tissue was washed twice with ice cold phosphate buffered saline and homogenised in 1 ml of hypotonic buffer A (10 mM HEPES, pH 7.8, 10 mM KCl, 2 mM MgCl2, 1 mM DTT, 0.1 mM EDTA, 0.1 mM phenylmethylsulphonyl fluoride (PMSF)). To the homogenates was added 125 μl of 10% Nonidet P-40 (NP-40) solution, and the mixture was centrifuged for 30 seconds at 12 000 rpm. The supernatant was collected as postnuclear (cytoplasmic) extracts for further assays and the pellets were washed once with 400 μl of buffer A plus 25 μl of 10% NP-40, centrifuged, resuspended in 100 μl of buffer C (50 mM HEPES, pH 7.8, 50 mM KCl, 300 mM NaCl, 0.1 mM EDTA, 1 mM DTT, 0.1 mM PMSF, and 10% glycerol), and centrifuged for five minutes at 12 000 rpm. Nuclear proteins (10 μg) were incubated for 30 minutes at 25°C with 20 pg of 32P labelled oligonucleotides containing the NFκB binding site (5′-AGTTGAGGGGACTTTCCCAGGC-3′). The NFκB oligonucleotide probe was labelled with [γ-32P] ATP by T4 polynucleotide kinase and purified on a nick spin column (Pharmacia Biotech, Uppsala, Sweden). The binding reaction was carried out in 25 μl of the mixture containing 5 μl of incubation buffer (10 mM Tris HCl, pH 7.5, 100 mM NaCl, 1 mM DTT, 1 mM EDTA, 4% (v/v) glycerol, and 0.1 μg/ml sonicated salmon sperm DNA), 10 μg of nuclear extracts, and 100 000 cpm of the labelled probe. To determine the sequence specificity of the NFκB DNA interaction, 100 fold excess amount of unlabelled oligonucleotide was added. After incubation, 2 μl of 0.1% bromophenol blue was added and the mixtures were electrophoresed through a 6% non-denaturing polyacrylamide gel at 150 V in a cold room. After electrophoresis, gels were dried and exposed to radiographic film for 24 hours at −70°C with intensifying screen. Supershift EMSAs were also performed using rabbit antibodies against four Rel proteins to determine the subunit composition of functionally active NFκB dimers in nuclear extracts of oesophageal mucosa of reflux oesophagitis. Each anti-p50, anti-p65, anti-p52, anti-c-Rel antibody (Santa Cruz, Santa Cruz, California, USA) was mixed with the NFκB probe at the start of the 30 minute incubation.
WESTERN BLOT ANALYSIS
Each tissue was washed twice with ice cold phosphate buffered saline and homogenised in 1 ml of ice cold hypotonic lysis buffer (10 mM HEPES, pH 7.8, 10 mM KCl, 2 mM MgCl2, 1 mM DTT, 0.1 mM EDTA, 0.1 mM PMSF) with Teflon for 20 seconds. The homogenates were kept on ice for 15 minutes and 100 μl of 10% NP-40 solution was added. The homogenates were centrifuged at 12 000 rpm for 30 seconds at 4°C. The supernatant was collected as a cytosol fraction and protein content was determined using a bicinchonic acid assay (Sigma). The homogenates were mixed with sodium dodecyl sulphate (SDS) loading buffer and boiled for five minutes. Equal amounts of protein (30 μg/lane) were electrophoresed in 4–12% SDS-polyacrylamide gels. Proteins were transferred to polyvinylidene difluoride membranes. The membranes were saturated with 5% non-fat dry milk in phosphate buffered saline with 0.1 % (v/v) Tween-20 for 30 minutes. The membranes were incubated with purified polyclonal rabbit IgG antibody against murine inhibitory protein of NFκB (IκBα) diluted at 1:1000 in the above solution for one hour at room temperature. The blots were washed three times (five minutes each) in phosphate buffered saline with 0.1 % (v/v) Tween-20. Further blots were incubated for one hour at room temperature with the goat antirabbit IgG antibody coupled to horseradish peroxidase at a 1:2500 dilution in phosphate buffered saline with 0.1 % (v/v) Tween-20, followed by three washes (five minutes each) in phosphate buffered saline with 0.1 % (v/v) Tween-20 before visualisation. The enhanced chemiluminescence kit was used for detection and exposed to film.
STATISTICAL ANALYSIS
Data are expressed as mean (SD) for each group. The Student'st test was used for statistical analysis; p<0.05 was considered statistically significant.
Results
GROSS MUCOSAL LESIONS OF REFLUX OESOPHAGITIS
Severe longitudinal ulcerations with yellowish exudates were observed in the oesophagus of all reflux oesophagitis controls (group II). Grossly, the thickness of the oesophagus in group II was increased compared with that in the sham operated group (group I). However, the gross appearance of the oesophagus in groups III and IV, groups pretreated with DA-9601 30 or 100 mg/kg respectively, showed only scattered erosions or mild haemorrhagic spots with whitish exudates scattered along the oesophagus (fig 1B). Although five of 30 rats in groups III and IV pretreated with DA-9601 30 or 100 mg/kg showed linear ulcerations, the mean gross lesion scores were markedly lower compared with group II. Acid suppression with ranitidine was not effective in decreasing the severity of reflux oesophagitis. Only DA-9601 pretreatment showed statistically significant decreases in mean scores for the extent of mucosal ulcerations and degree of mucosal inflammation. Although ranitidine pretreatment attenuated the extent of mucosal ulcerations, its protective effect was not as prominent as that of DA-9601 (fig 1C).
HISTOLOGICAL ACTIVITY INDEX OF REFLUX OESOPHAGITIS
Figure 2A shows the extent of oesophageal ulceration according to group. Twelve of group II rats with mixed reflux (80%) developed large coalesced longitudinal ulcers in the lower and middle parts of the oesophagus whereas only four of 14 rats (26.7%) in group III and three of 15 rats (20%) in group IV showed focal and non-longitudinal ulcerations. The ranitidine treated group showed oesophageal ulcerations in nine of 15 rats (60%). Scattered erosions rather than ulceration were prominent lesions in the DA-9601 pretreated group whereas large longitudinal ulcerations were frequently observed in groups II and V. Figure 2B shows the severity of inflammation with oesophageal wall thickness. The mean inflammation scores of groups III and IV (DA-9601 treated group) were significantly lower than those of the reflux oesophagitis control (group II) or ranitidine pretreated group (group V). In the oesophageal mucosa of groups III and IV, high powers of regenerating activities were observed. The representative pathological values are shown in fig 2C, demonstrating severe inflammatory cell infiltrations with large excavated ulcerations. Statistically significant improvements in mean histological activity index (HAI) scores were observed in antioxidant-treated groups (fig3A). Nearly all oesophageal mucosa showed excellent regenerating activities in groups III and IV whereas none or scant evidence of regenerating activities was observed in groups II and V (fig 3B). Therefore, antioxidant pretreatment provided the resistance to oesophageal ulceration against mixed refluxates and imposed active regenerating activities on affected oesophageal mucosa in accordance with attenuated inflammatory cell infiltrations.

(A) Extent of oesophageal ulcers in the four groups (HAI, histological activity index). In the reflux oesophagitis control (group II) and ranitidine pretreated (group V) groups, oesophageal mucosa was almost denuded and moderate to severe degrees of inflammation replaced the submucosa of reflux oesophagitis. However, only scattered erosions or shallow ulcers were observed in groups III (pretreated with DA-9601 30 mg/kg) and IV (pretreated with DA-9601 100 mg/kg). A statistically significant decrease in the extent of oesophageal ulcer was noted in group IV (*p<0.05 compared with group II). (HAI ulcer: 0, none; 1, erosions; 2, multiple erosions; 3, ulcer; 4, large excavated ulcers.) (B) Degree of oesophageal inflammation in the four groups. In the reflux oesophagitis control and ranitidine pretreated groups, the oesophageal submucosa was almost replaced with inflammatory cell infiltrations in accordance with the occurrence of oesophageal ulcerations. DA-9601 pretreatment (groups III and IV) was excellent in decreasing oesophageal inflammation. A statistically significant decrease in the degree of oesophageal inflammation was noted in the DA-9601 100 mg/kg pretreated group (*p<0.05 compared with group II). (HAI inflammation: 0, none; 1, mild; 2, moderate; 3, severe.) (C) Oesophageal regenerating activities in the four groups. Any evidence of oesophageal regenerations was not seen in group II, with only scanty regeneration activities in group V, whereas significant oesophageal regeneration was observed in antioxidant pretreated group. Statistically significant increases in oesophageal regeneration were noted in groups III and IV (*p<0.05 compared with group II). (HAI regeneration: 0, none; 1, a little; 2, some; 3, many.)

Changes in histological activity index (HAI) and representative pathological photographs. (A) Changes in HAI. DA-9601 treatment (groups III and IV) significantly decreased mean HAI scores for oesophageal ulcer and inflammation. *p<0.05, **p<0.01 versus group II. (B) Disappearance of oesophageal squamous epithelia with oesophageal inflammatory cell infiltration was noted after generation of reflux oesophagitis (group II). Excellent evidence of epithelial regeneration and attenuation of inflammatory cell infiltrations were noted in DA-9601 treated groups (groups III and IV). Treatment with antisecretory drug was not as effective in either decreasing the degree of oesophageal inflammation or imposing regenerating capacities (×100 original magnification). Group I, sham operated group; group V, ranitidine pretreated group.
OESOPHAGEAL MUCOSAL MALONDIALDEHYDE (MDA), REDUCED GLUTATHIONE (GSH), AND MYELOPEROXIDASE (MPO) ACTIVITIES
Accumulation of MDA reflected the extent of oxygen derived free radical induced cell damage. Mucosal MDA levels were significantly increased in the reflux oesophagitis control group compared with the normal control group (p<0.001). Absolute levels of mucosal MDA were significantly lower in groups III and IV compared with groups II and V (fig 4A). Reflux oesophagitis caused the oesophageal mucosa to deplete its GSH contents. GSH levels were markedly decreased after generation of reflux oesophagitis in group II (p<0.001). However, statistically significant preservation of mucosal GSH content was observed in the DA-9601 pretreated groups (groups III and IV) (fig 4B). Ranitidine did not affect MDA levels or GSH content of oesophageal mucosa. A statistically significant increase in mucosal myeloperoxidase (MPO) activity was noted in group II compared with group I. Although DA-9601 treatment decreased mean MPO activities of the affected oesophagus compared with group II, this was not statistically significant (fig4C).

Changes in malondialdehyde (MDA) levels, glutathione (GSH) content, and myeloperoxidase (MPO) activity in the five groups. (A) MDA levels in the reflux oesophagitis control group (group II) were significantly increased compared with those of normal controls (group I). DA-9601 pretreatment (groups II and III) significantly decreased the amount of MDA formation, which suggested inhibition of reflux oesophagitis associated lipid peroxidation by antioxidant treatment. Ranitidine (group V) was not effective in decreasing MDA formation. (B) Mucosal levels of GSH were significantly decreased in group II compared with the normal control group (group I) . However, DA-9601 pretreatment (groups II and III) preserved GSH levels significantly, which suggested supplementation of scavenging activities through DA-9601 treatment. (C) MPO activity was significantly increased after generations of reflux oesophagitis. DA-9601 treatment decreased mucosal MPO activity. **p<0.01, ***p<0.001 versus group I.
INHIBITION OF NFκB ACTIVATION BY ANTIOXIDANTS IN OESOPHAGEAL MUCOSA OF REFLUX OESOPHAGITIS
Figure 5 shows the NFκB complex of nuclear proteins extracted from each group. Pretreatment with DA-9601 decreased NFκB DNA binding in a dose dependent manner. Radioactivities of 32P in each NFκB band of tissues treated with DA-9601 30 mg/kg, DA-9601 100 mg/kg, and ranitidine 10 mg/kg were 55%, 40%, and 60% of control levels, respectively. According to the supershift assay, p50 Rel protein was a major subunit of reflux oesophagitis associated NFκB activation (fig 5B). IκBα protein expression in the reflux oesophagitis group was significantly decreased in group II compared with group I, consistent with the findings of the NFκB EMSA. Decreased IκBα in cytoplasm suggested significant degradation of this inhibitory protein after dissociation from NFκB (fig 5C). Nuclear extracts from DA-9601 treated rats exhibited higher levels of IκBα protein, which suggested less translocation of inflammatory transcription factor NFκΒ, reflecting attenuated oxidative stress in DA-9601 treated oesophageal mucosa.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in nuclear factor κB (NFκB) transcription factor according to group. (A) Electrophoretic mobility shift assay (EMSA) for NFκB. The reflux oesophagitis control group (group II) showed high activity of NFκB in nuclear extracts of inflamed oesophageal mucosa. DA-9601 pretreatment (groups III and IV) caused decreases in the amounts of inflammation associated transcription factor NFκB in a dose dependent manner. (B) EMSA and supershift EMSA. EMSA, using various types of antibodies against the components of NFκB, showed binding of the p50 subunit of NFκB with nuclear extracts of inflamed oesophageal mucosa. (C) IκBα expression according to group. The reflux oesophagitis control group (group II) showed low level IκBα expression in cytoplasmic extracts of inflamed oesophageal mucosa whereas DA-9601 pretreatment (groups III and IV) caused preservation of significant amounts of IκBα, which suggested the possibility that reflux oesophagitis through mixed reflux caused increased proteosomic degradation of phosphorylated IκBα and activation of NFκB.
Discussion
This study provides concrete evidence that oxygen free radicals are involved in oesophageal mucosal damage from reflux oesophagitis in rats. The study also suggests that antioxidants should be considered as firstline therapy in the treatment of reflux oesophagitis based on the experimental results that the oxidative stress response NFκB pathway played a major role in generation of reflux oesophagitis and antisecretory treatment alone was not as effective in either decreasing the degree of reflux oesophagitis or attenuating inflammation associated NFκB activation. Compared with antisecretory drugs, antioxidant pretreatment was excellent in decreasing the gross and histopathological scores of reflux oesophagitis and decreasing oxidative injury mediated NFκB activation.
As reflux oesophagitis is a chronic disease caused by a mechanically defective lower oesophageal sphincter or excess refluxates, acid loads into the oesophagus appeared to be the major mediator in oesophageal mucosal damage.17 However, according to recent animal studies,9 ,10 ,18 ,19 it has been shown that gastro-oesophageal reflux enhances production of oxygen derived free radicals which subsequently caused oesophageal mucosal damage. Free radicals seem to be a major cause of reflux induced oesophageal damage as it has been shown that administration of free radical scavengers such as superoxide dismutase almost completely inhibited oesophagitis in rats.11 Clinically, Wetscher and colleagues9 demonstrated increased production of oxygen derived free radicals in distal oesophageal biopsy samples of patients with reflux oesophagitis compared with those of controls. Increased production of oxygen derived free radicals was accompanied by enhanced oesophageal mucosal lipid peroxidation which is a sensitive marker of membrane damage caused by free radicals.
Interestingly we observed that acid refluxates alone were not sufficient to cause reflux oesophagitis. Initially, we made the duodenal lumen narrower by inserting a small calibre ring 1 cm behind the pyloric channel to generate reflux oesophagitis, but it failed to provoke significant reflux oesophagitis in rats. Instead, we developed a rat model of reflux oesophagitis by inserting the same small calibre ring into the duodenum, distal to the ligament of Treitz, which caused mixed reflux (fig 1A). The former group showed only several gastric ulcers instead of reflux oesophagitis. Mixed reflux has been shown to produce more free radical damage in the oesophageal mucosa than pure acid reflux.20 Several researchers also found similar results: rats exposed to acid reflux had much smaller ulcers than those with mixed reflux and acid reflux alone did not generate oxygen derived free radicals.21 ,22 This is also supported by clinical observations that patients with severe oesophagitis and diverse complications of reflux oesophagitis experienced significantly prolonged episodes of alkaline reflux rather than acid reflux and high production of free radicals.23 It could also explain why Barrett's oesophagus carries an increased risk of malignant transformation as prolonged exposure to alkaline reflux has been demonstrated for this group of patients and it is known that oxygen derived free radicals act as carcinogens by causing DNA damage, increased generation of 8-hydroxydeoxyguanosine formation, or deletion/mutation of cell cycle regulators.24
Hence therapy should be aimed at permanently reducing free radical production in the affected oesophageal mucosa with antisecretory drugs. Medical therapy with antisecretory medications such as H2-RAs or proton pump inhibitors (PPIs), although initially effective in 90% of reflux oesophagitis patients, does not permanently control reflux oesophagitis in patients with an ineffective antireflux barrier.25 This could be inferred from the fact that medical therapy with antisecretory medications is not effective in either inhibiting free radical formation or scavenging free radicals generated, which may explain the low treatment success rate in patients with reflux oesophagitis. The importance of antioxidants in the treatment of reflux oesophagitis also comes from the fact that oxidative damage has long been related to carcinogenesis in human cancers and animal cancer models18 ,26 and oxidative damage has been reported to be related to columnar lined oesophagus (Barrett's oesophagus).27 Reactive oxygen species increased with the grade of oesophagitis and were reported to be highest in Barrett's oesophagus.28 Chen and colleagues18 developed a rat oesophageal adenocarcinoma model by using oesophagoduodenal anastomosis plus iron supplementation. Oxidative damage to DNA, proteins, and lipids in the oesophagus was significantly higher than that of non-operated controls. Columnar lined oesophagus cells were believed to be the target cells of oxidative damage because they overexpressed haeme oxygenase 1 and metallothionein, both known to be responsive to oxidative damage.29
NFκB is recognised as a redox sensitive transcription factor and has been implicated in the cellular response to oxidative stress.30 Several laboratories have demonstrated that treatment of cells with H2O2 can activate the NFκB pathway.31 The observation that inducers of NFκB activity, such as tumour necrosis factor α, interleukin 1, lipopolysaccharide, PMA (phorbol 12-myristate 13-acetate), UV, and ionising radiation generated elevated levels of reactive oxygen species prompted speculation that reactive oxygen species may function as common mediators of NFκB activation.32 Nearly all inflammatory pathways leading to NFκB activation were blocked by a variety of antioxidants, includingN-acetyl-l-cysteine, GSH, thioredoxin, pyrrolidine dithiocarbamate, or by overexpression of antioxidant enzymes.30 Generation of oxidative stress to specific cells results in the appearance of the hyperphosphorylated form of IκB, which undergoes rapid degeneration in the absence of proteosome inhibitors.33 This suggests that reactive oxygen species generated through mixed reflux act upstream or directly on the IκBα kinase complex. We found that pretreatment with DA-9601 completely blocked IκB phosphorylation and degradation in our reflux oesophagitis model.
Our study has provided the first confirmative evidence that antioxidant treatment seems to be more important in the prevention and treatment of reflux oesophagitis than current antisecretory treatments such as H2-RA or PPI. However, we could not entirely exclude the useful role of antisecretory medications in the prevention and treatment of reflux oesophagitis as acid and pepsin also contributed to the development of reflux oesophagitis.34 ,35 Lanas and colleagues6 developed experimental oesophagitis mimicking human reflux oesophagitis through induction by acid and pepsin. Therefore, we infer that a combination regimen, including both antioxidants and antisecretory drugs, may be beneficial in either preventing direct mucosal cell damage or supplementing regenerating capabilities. Conclusively, oxygen derived free radicals seem to be important mediators in the generation of reflux oesophagitis and the combination of antioxidant and antisecretory medications is the treatment of choice in the prevention and treatment of reflux oesophagitis.
Acknowledgments
The authors thank Miss Yu-Jin Kim and Ju-Hyun Jin (Laboratory of Liver and Digestive Disease, Department of Gastroenterology, Ajou University School of Medicine, Suwon, Korea) for help with the experiments.
Abbreviations used in this paper
- NFκB
- nuclear factor κB
- IκBα
- inhibitory protein of NHκB
- H2-RA
- histamine H2 receptor antagonist
- MDA
- malondialdehyde
- GSH
- reduced glutathione
- PMSF
- phenylmethylsulphonyl fluoride
- NP-40
- Nonidet P-40
- EMSA
- electrophoretic mobility shift assay
- SDS
- sodium dodecyl sulphate
- HAI
- histological activity index
- MPO
- myeloperoxidase
- PPI
- proton pump inhibitors