Article Text

Abstract
BACKGROUND Most low grade gastric lymphomas arising from the mucosa associated lymphoid tissue (MALT) are related to Helicobacter pylori colonisation. Cases with disease limited to the stomach can be cured after H pylori eradication and remain in remission for years. In contrast, high grade lymphomas of the stomach, although also related toH pylori, do not usually respond to eradication treatment.
CASE REPORT A 36 year old patient was referred from another hospital with a diagnosis of a low grade gastric MALT lymphoma associated with H pylori. The patient was in stage I and while waiting for the biopsies to be reviewed H pylori eradication therapy was given as the first step of treatment. Review of the biopsies showed a high grade immunoblastic lymphoma with areas of low grade gastric MALT lymphoma (high grade gastric MALT lymphoma or diffuse large B cell lymphoma with areas of MALT type lymphoma of the WHO classification). The patient received no further treatment but has been closely followed up for 32 months with sequential endoscopies to obtain biopsies for histological studies, H pylori cultures, and polymerase chain reaction analysis of the IgH gene.
RESULTS AfterH pylori eradication the patient had a complete histological response that has been maintained for 32 months. Monoclonal IgH gene rearrangement persisted for 32 months.
CONCLUSION The response of this patient indicates the possibility that some cases of high grade gastric MALT lymphoma (possibly patients in stage I with a superficial or limited disease) may still be responsive toH pylori antigenic drive and may be cured with eradication therapy. Prospective studies should be performed to identify patients with high grade gastric MALT lymphomas that may respond to eradication therapy and be spared of other more aggressive treatments.
- mucosa associated lymphoid tissue
- lymphoma
- gastric lymphoma
- immunoblastic lymphoma
- Helicobacter pylori
Statistics from Altmetric.com
Helicobacter pylori eradication can cause regression of the histological lesions of low grade gastric lymphomas derived from the mucosa associated lymphoid tissue (MALT) in 50–90% of patients when the disease is limited to the stomach (stage I),1-4 and remission seems to be maintained in most cases for years.3 ,4 Eradication also appears to be effective with more extensive disease, at least in a few cases, as five patients with extragastric disease stage II T3 N1 were also reported to be cured.5 However, high grade gastric MALT lymphoma is not usually thought to respond toH pylori eradication as the sole therapy. We describe a case of high grade gastric MALT lymphoma stage I that showed sustained remission after H pylorieradication.
Case report
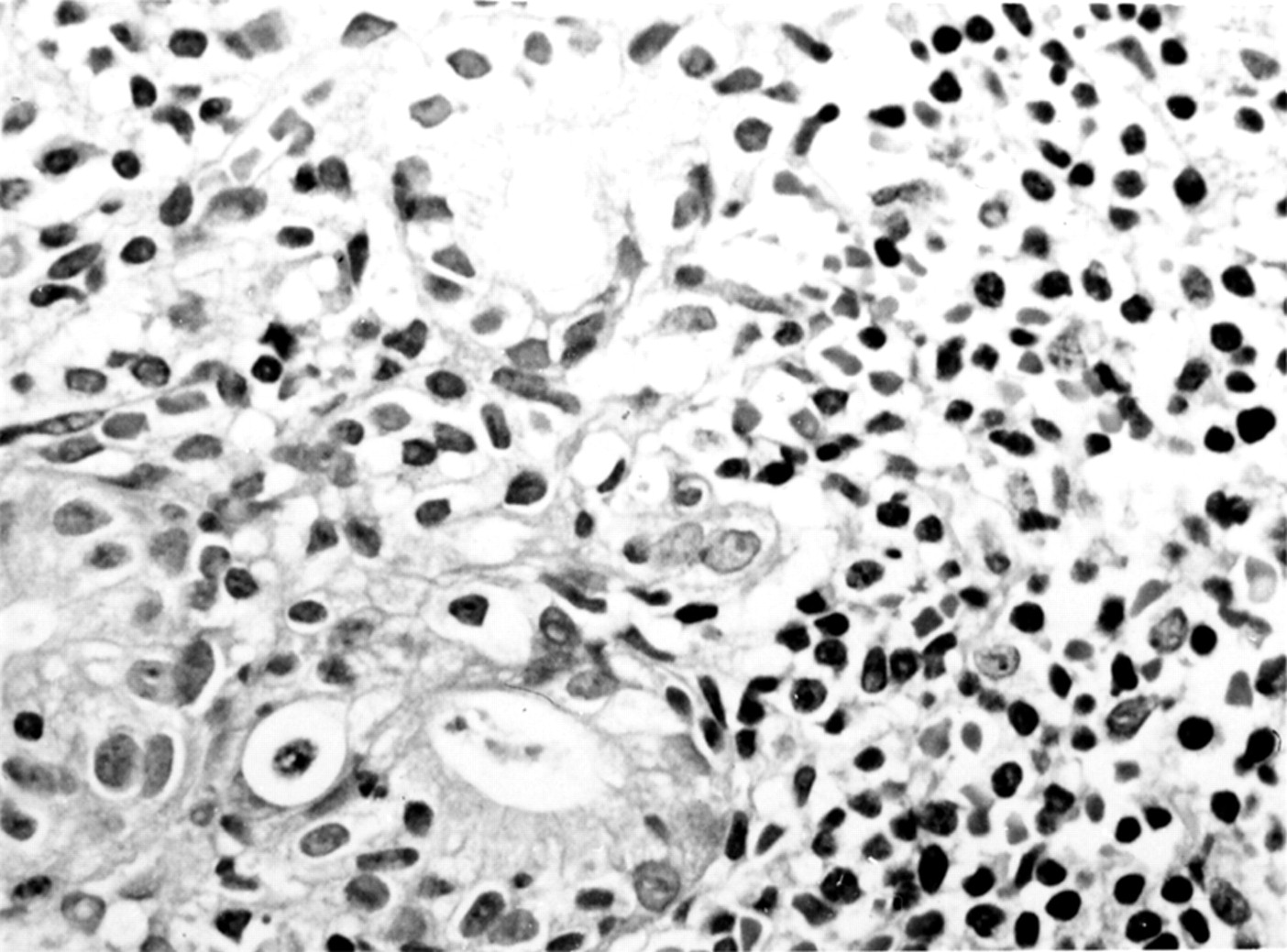
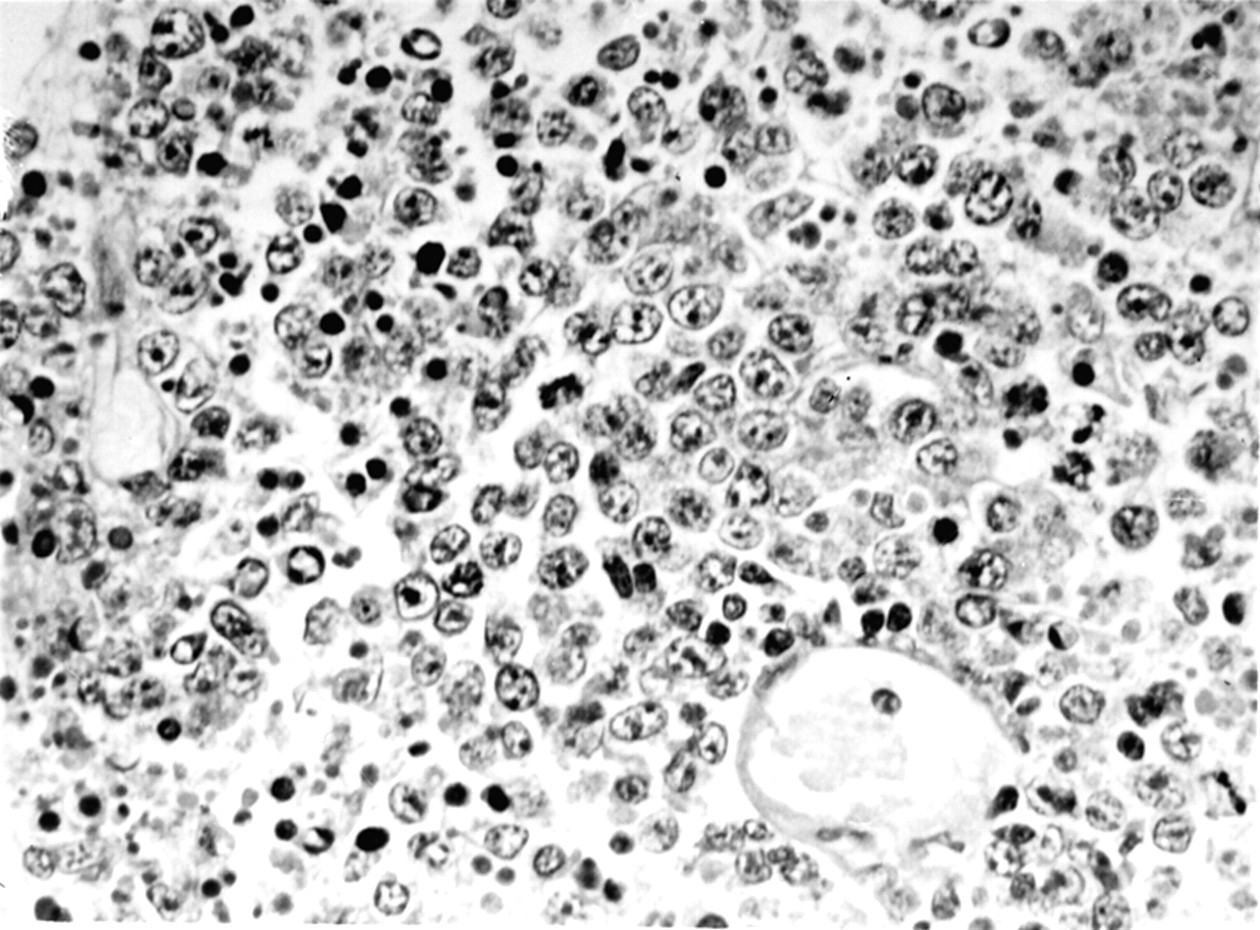
A 36 year old patient was referred from another hospital. In the previous 2–3 years he had epigastric burning pain, more intense in the last two months. A barium examination of the stomach showed enlarged mucosa folds throughout the whole stomach but especially prominent in the fundus. Endoscopy performed in April 1998 also showed diffuse enlarged gastric folds throughout the stomach, also more conspicuous in the fundus. A gastric biopsy from the fundus was diagnosed as low grade gastric MALT lymphoma; a urease test for H pylori was positive. He was then referred to our hospital where physical examination was normal. Blood and biochemical parameters, intestinal radiological series, computed tomography scan, bone marrow biopsy, and peripheral blood and bone marrow immunophenotype were normal. Human immunodeficiency virus serology was negative. Based on the above investigations, the patient was classified as stage I according to the Lugano system, although endoscopic ultrasonography was not performed as it was not available in our hospital. While waiting for the original biopsies to be reviewed he was treated forH pylori eradication (clarithromycin, amoxicillin, and omeprazole for 14 days) as the initial step of treatment and discharged home. When we received the biopsy samples obtained in the other hospital we were able to review only two haematoxylin-eosin stained slides from the initial biopsy of the gastric fundus. In both slides some sections showed infiltration of the lamina propria with large lymphoid cells with prominent nucleoli characteristic of immunoblastic lymphoma (fig 1) whereas in other sections there was a dense infiltrate with small centrocytoid lymphoid cells and gland infiltration and destruction (lymphoepithelial lesion), demonstrating low grade MALT lymphoma (fig 2). The combination of these findings was characteristic of high grade MALT lymphoma (alternatively, diffuse large B cell lymphoma with areas of MALT type lymphoma following the WHO classification6). H pylori was not histologically identified in either of the two slides.

Infiltration of the lamina propria with large lymphoid cells: immunoblastic lymphoma (haematoxylin-eosin).
Diffuse infiltrate of small centrocytoid lymphocytes in the lamina propria with gland destruction (lymphoepithelial lesion): low grade mucosa associated lymphoid tissue lymphoma in other sections of the same biopsy (haematoxylin-eosin).
As the patient was asymptomatic after eradication treatment, he received no further treatment and was scheduled for close follow up. In all subsequent sequential endoscopies performed in our hospital, multiple biopsies were obtained from the fundus, body of the stomach, antrum, and duodenum. Biopsy samples were routinely processed for histological study and stained with haematoxylin-eosin and Giemsa. Histological findings in the follow up biopsies were evaluated according to the scoring system described by Wotherspoon and colleagues.1 Fresh biopsy samples were also obtained from each area for culture of H pylori and molecular studies. H pylori was cultured in a non-selective (agar Columbia) and in a selective medium (agar Columbia with polymyxin, amphotericin, trimethoprim, vancomycin, and nalidixic acid in a microaerophilic atmosphere). Polymerase chain reaction (PCR) analysis of the IgH gene was performed as previously described.2 ,7 High molecular weight DNA was prepared from frozen biopsy material using standard phenol/chloroform extraction. Control DNA samples were extracted from the Raji B cell line (clonal control) and from reactive lymphoid tissue (polyclonal control). Amplification of the IgH gene was performed on all samples using semi nested procedures with consensus primers for the VH region (Fr3A or Fr2A) in conjunction with nested primers directed to the JH region (LJH and VLJH). PCR product (10 μl) was electrophoresed on 5% (Fr2A) or 10% (Fr3A) polyacrylamide mini gels which were stained with ethidium bromide and viewed under UV light.
In the first control endoscopy, three months afterH pylori eradication treatment, only slightly prominent gastric folds were present. Gastric biopsies showed no lymphoma. In sequential endoscopies over 32 months, biopsies showed no lymphoma (table 1) but PCR analysis detected a monoclonal rearrangement of the IgH gene that has persisted for 32 months (table1). H pylori has not been identified in sequential histological samples or in biopsy cultures, and breath test urea 13C has been persistently negative.
Sequential follow up after diagnosis and Helicobacter pylori eradication treatment. Endoscopic, histological, and molecular findings
Discussion
Our patient had been referred from another hospital with a diagnosis of low grade gastric MALT lymphoma. After clinical evaluation, he was considered to have stage I disease with diffuse extension of the lymphoma throughout the surface of the stomach. However, the depth of the involvement of the gastric wall and perigastric lymph nodes might have been underestimated as endosonography was not performed. He received H pylori eradication treatment assuming that he had a low grade MALT lymphoma. When the histological slides were reviewed, a high grade gastric lymphoma with areas of low grade MALT lymphoma were found instead. The eradication treatment was accepted as the initial step of treatment of the high grade gastric MALT lymphoma as it is essential to prevent a later low grade relapse8 ,9 but when he was re-evaluated and a complete response was evident, he received no further therapy. He has remained in histological remission for 32 months, although monoclonal IgH gene rearrangement (with occasional polyclonal rearrangement) has persisted. We need a longer follow up to evaluate the final fate of this patient but the histological findings indicate that he seems to be histologically cured. The long term significance of persistent monoclonal IgH gene rearrangement is not known, as is also the case in patients with low grade gastric MALT lymphoma who have persistent monoclonal IgH gene rearrangement after achieving histological remission.2-5
In experimental studies, H pylori cultures cannot induce proliferative responses in the lymphocytes of high grade gastric MALT lymphoma.10 Also, in clinical practice, it is a common finding that failure to achieve a response in low grade gastric MALT lymphoma after eradication therapy is due to the presence of high grade lymphoma or to involvement of deeper layers of the gastric wall.4 ,11 It is assumed that in such a situation the antigen dependence of H pylori seems to have been lost and the growth of the tumour has become autonomous. However, isolated cases of gastric high grade MALT lymphoma responding to H pylori eradication have been reported. Seymour and colleagues12 reported a case with a gastric (but not systemic) response of a disseminated high grade gastric MALT lymphoma associated with H pylori. Chen and colleagues13 described eight patients from Taiwan in stage IE that had been treated only with H pylori eradication: five of the seven patients who had successful eradication also had regression of the high grade lymphoma that persisted for up to 24 months. Roggero and colleagues14 reported four cases with localised disease (stage I) who had a complete response after eradication therapy that was maintained after a median follow up of 16 months. Ng and colleagues15 reported a complete response lasting 18 months in a high grade gastric MALT lymphoma presenting as a solitary large gastric ulcer in the antrum. Morgner and colleagues16 described the histological regression of gastric high grade MALT lymphoma in six of seven patients initially treated only with H pylori eradication, and that in four of them the remission persisted for 6–66 months without further treatment.
The findings in our patient, as well as those in other reported cases, indicate that at least some cases of high grade gastric MALT lymphoma may histologically regress with H pylori eradication as the sole therapy. It is obvious that these cases are still dependent on the antigenic drive ofH pylori yet they lack specific features to predict this response. We believe that several factors may influence a better chance of response. One factor may be limited extension of the disease, affecting only superficial layers of the stomach, as is the case in low grade cases,5 ,11 and also a relative low proportion of high grade components since it has been shown that an increasing number of blast cells and clusters of blast cells are associated with poor survival.17 ,18 Other factors may be the specific gastric localisation (with improved chances for gastric distal localisation) or the strain of H pylori. Molecular abnormalities may also be important, as is the case in low grade MALT lymphoma where absence of expression of the fusion transcript API2-MLT of the translocation t(11;18) seems to favourably influence the response to H pylori eradication19 whereas its expression20 and the presence of BCL10 mutations21 appear to be associated with failure to respond to antibiotics and the latter with a more aggressive behaviour.21
The favourable response to H pylorieradication of the present patient, and of the other cases reported, is rather exceptional and does not mean that all patients with localised (stage I) high grade gastric MALT lymphoma should be treated exclusively with eradication treatment. Rather it suggests that after eradication therapy as the initial treatment8 ,9 in patients with limited superficial disease, no infiltration of deeper layers of the gastric wall, and limited areas of high grade lymphoma, and most of all, when these patients can be closely monitored, chemotherapy may be postponed until follow up indicates whether or not further treatment is necessary. A prospective study of larger numbers of such patients may help to detect the factors that may predict a good response to H pylori eradication to avoid the use of an unnecessary and toxic treatment such as chemotherapy in patients that may already have been cured.
References

{kind=link}
{kind=link}
{kind=link}
Abbreviations used in this paper
- MALT
- mucosa associated lymphoid tissue
- PCR
- polymerase chain reaction