Article Text

Abstract
Background—Many individuals have serum antibodies against Clostridium difficile toxins. Those with an impaired antitoxin response may be susceptible to recurrent, prolonged, or severe C difficile diarrhoea and colitis.
Aims—To examine whether treatment with intravenous immunoglobulin might be effective in patients with severe pseudomembranous colitis unresponsive to standard antimicrobial therapy.
Patients—Two patients with pseudomembranous colitis not responding to metronidazole and vancomycin were given normal pooled human immunoglobulin intravenously (200–300 mg/kg).
Methods—Antibodies against C difficile toxins were measured in nine immunoglobulin preparations by ELISA and by cytotoxin neutralisation assay.
Results—Both patients responded quickly as shown by resolution of diarrhoea, abdominal tenderness, and distension. All immunoglobulin preparations tested contained IgG against C difficile toxins A and B by ELISA and neutralised the cytotoxic activity of C difficile toxins in vitro at IgG concentrations of 0.4–1.6 mg/ml.
Conclusion—Passive immunotherapy with intravenous immunoglobulin may be a useful addition to antibiotic therapy for severe, refractory C difficile colitis. IgG antitoxin is present in standard immunoglobulin preparations andC difficile toxin neutralising activity is evident at IgG concentrations which are readily achieved in the serum by intravenous immunoglobulin administration.
- Clostridium difficile
- toxin
- diarrhoea
- IgG
- immunotherapy
- antibiotic
Statistics from Altmetric.com
Clostridium difficile antibiotic associated colitis is an important cause of morbidity in hospital and nursing home patients.1 As many as 26% of hospital patients are colonised by C difficile and up to one third of these develop diarrhoea.2 There is a wide spectrum of host response to C difficile infection ranging from asymptomatic carriage to fulminant colitis with toxic megacolon.1 C difficile colitis is mediated by two large protein exotoxins released by pathogenic strains of the bacterium.1 ,3-7 Toxin A is a 308 kDa protein which is both a cytotoxin and a potent inflammatory enterotoxin.8-10 Toxin B, a 280 kDa protein, is a more potent cytotoxin than toxin A but is not enterotoxic for rodent intestine.7 ,11 However, toxin B may be even more harmful to human colon than toxin A.6 Both toxins share the same intracellular mechanism of cytotoxicity. They act as enzymes to glucosylate a threonine residue on small GTP binding rho proteins.12 ,13 This leads to the disaggregation of actin filaments, collapse of the cytoskeleton, and cell rounding.
The presence or absence of an adequate antibody response to C difficile toxins may play an important role in determining the severity of diarrhoea and colitis.14 Serum antibodies to toxins A and B are evident in two thirds of healthy adults.15-17 Patients with low antitoxin antibody levels are reported to have more severe, more prolonged, or recurrent C difficile diarrhoea whereas asymptomatic carriers have higher antitoxin levels.18-23 We previously reported that children with recurrent C difficile diarrhoea had low levels of serum IgG against C difficile toxin A.21 When these children were treated with intravenous immunoglobulin their serum antitoxin levels increased and their diarrhoea resolved. We now report the use of intravenous immunoglobulin therapy in two adults with severe pseudomembranous colitis which failed to respond to standard antibiotic treatment with metronidazole and vancomycin. We also demonstrate that normal human pooled immunoglobulin contains antibodies against C difficile toxins A and B which can neutralise the cytotoxic effects of these toxins.
Methods
MEASUREMENT OF ANTI-C DIFFICILE IgG IN IMMUNOGLOBULIN PREPARATIONS
Nine human immunoglobulin preparations intended for intravenous administration were studied. Three batches of immunoglobulin were obtained from each of the following producers: Alpha Therapeutic Corporation (Los Angeles, California, USA), Armour Pharmaceutical Company (Kankakee, Illinois, USA), and Baxter Healthcare Corporation (Glendale, California, USA). All were highly purified preparations of intact unmodified IgG isolated from large pools of human plasma by cold alcohol fractionation.
Human IgG levels to C difficile antigens were measured by enzyme linked immunosorbent assay (ELISA) as previously described.15 ,21 ,24 IgG directed against highly purifiedC difficile toxins A and B and against a culture filtrate of toxigenic C difficile (strain VPI 10463) were measured separately. The C difficile culture filtrate contains toxins A and B as well as non-toxin C difficile antigens. ELISA results are expressed as optical density readings at 450 nm.15 ,21 ,24
MEASUREMENT OF C DIFFICILE TOXIN NEUTRALISING ACTIVITY IN IMMUNOGLOBULIN PREPARATIONS
Cytotoxicity was determined by rounding of fibroblasts (R9AB, American Type Culture Collection, Rockville, Maryland, USA) in monolayer culture after exposure to C difficiletoxins.5 ,24 ,25 The minimum 50% cytotoxic dose for each toxin preparation, defined as the minimum dose resulting in 50% cell rounding at 24 hours, was 0.1 ng/ml for toxin A, 0.003 ng/ml for toxin B, and 0.5 ng/ml for culture filtrate in these experiments. Inhibition of cytotoxicity was quantified by adding serial twofold dilutions of the immunoglobulin preparations to four times the minimum 50% cytotoxic dose of each toxin preparation. After 20 minutes the toxin/immunoglobulin mixture was added to fibroblast monolayer cultures and cell rounding was assessed after 24 hours. Controls included human serum albumin diluted to the same protein concentration as the IgG and serum from a healthy volunteer who lacked specific antibodies againstC difficile toxin A or toxin B as determined by ELISA.15 ,23 Results are expressed as the lowest concentration of human IgG required to prevent rounding of 50% of the fibroblasts.24
Case reports and Results
PATIENT 1
A 63 year old woman developed diarrhoea, cramping abdominal pain, and abdominal distension five days after laparotomy for staging of non-Hodgkin’s lymphoma. She received intravenous ceftazidime perioperatively but had not been treated with cytotoxic chemotherapy. She had a peripheral blood leucocytosis of 22 000 cells/μl with 6% band forms. Flexible sigmoidoscopy and biopsy demonstrated pseudomembranous colitis of the rectum and sigmoid colon. Treatment was begun with both intravenous metronidazole (500 mg, six hourly) and oral vancomycin (250 mg, six hourly). After five days she continued to suffer from profuse diarrhoea and had a persistent leucocytosis of 21 000 cells/μl. The patient’s abdomen became distended and diffusely tender. A plain abdominal radiograph showed an ileus pattern with both small intestinal and colonic dilatation. A computed tomogram showed dilatation of the colon and the presence of ascites (fig 1). Intravenous immunoglobulin was administered (300 mg/kg). The diarrhoea improved rapidly. After 36 hours her abdominal pain and distension had resolved and her white blood cell count was normal at 9800 cells/μl. Treatment with metronidazole and vancomycin was continued for a further 10 days. One month later she suffered a recurrence of diarrhoea and had a positive stool cytotoxin assay. On this occasion she responded to treatment with oral metronidazole.
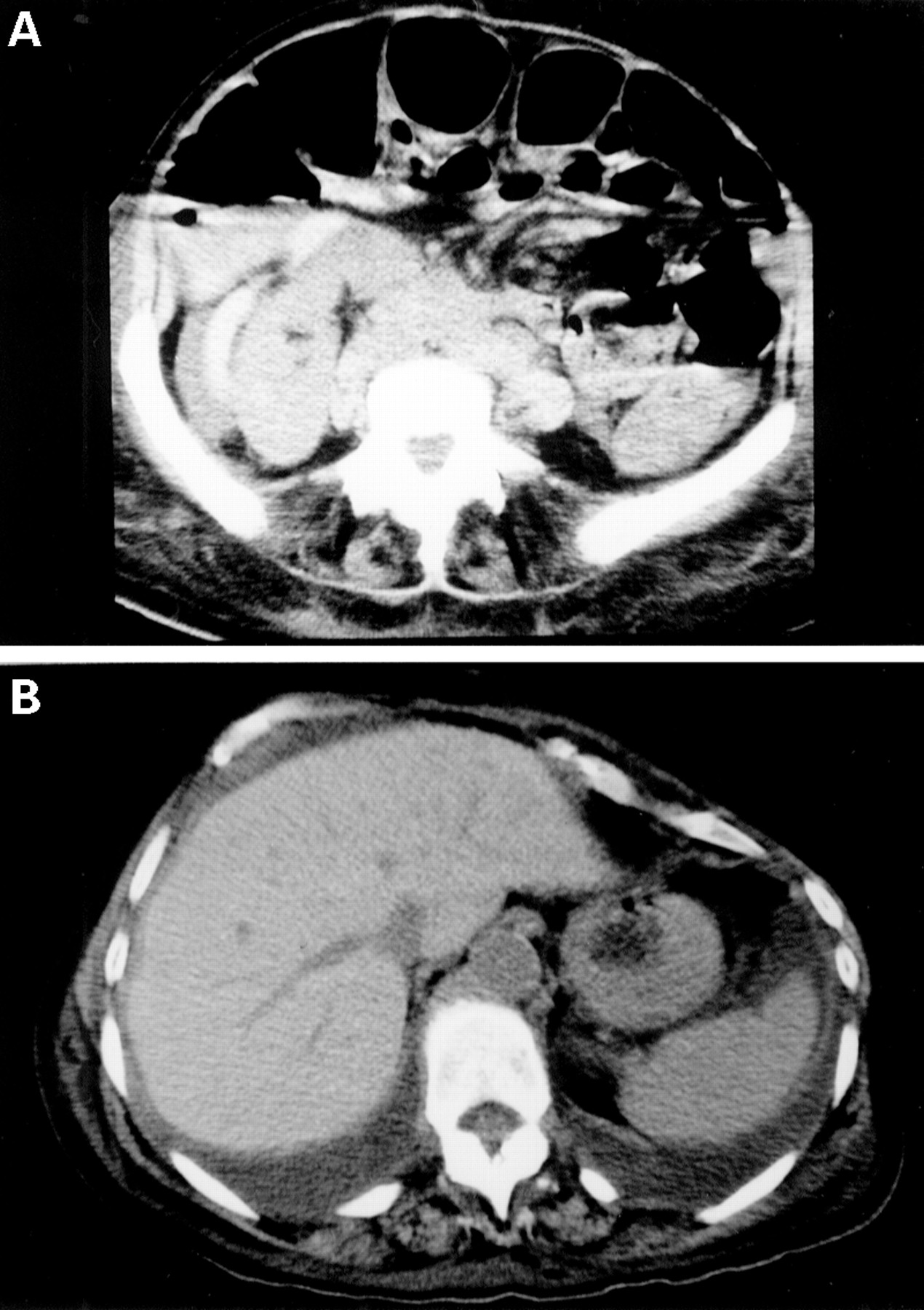
: Computed tomogram of the abdomen of patient 1 showing dilated loops of colon (A) and the presence of ascitic fluid (B).
PATIENT 2
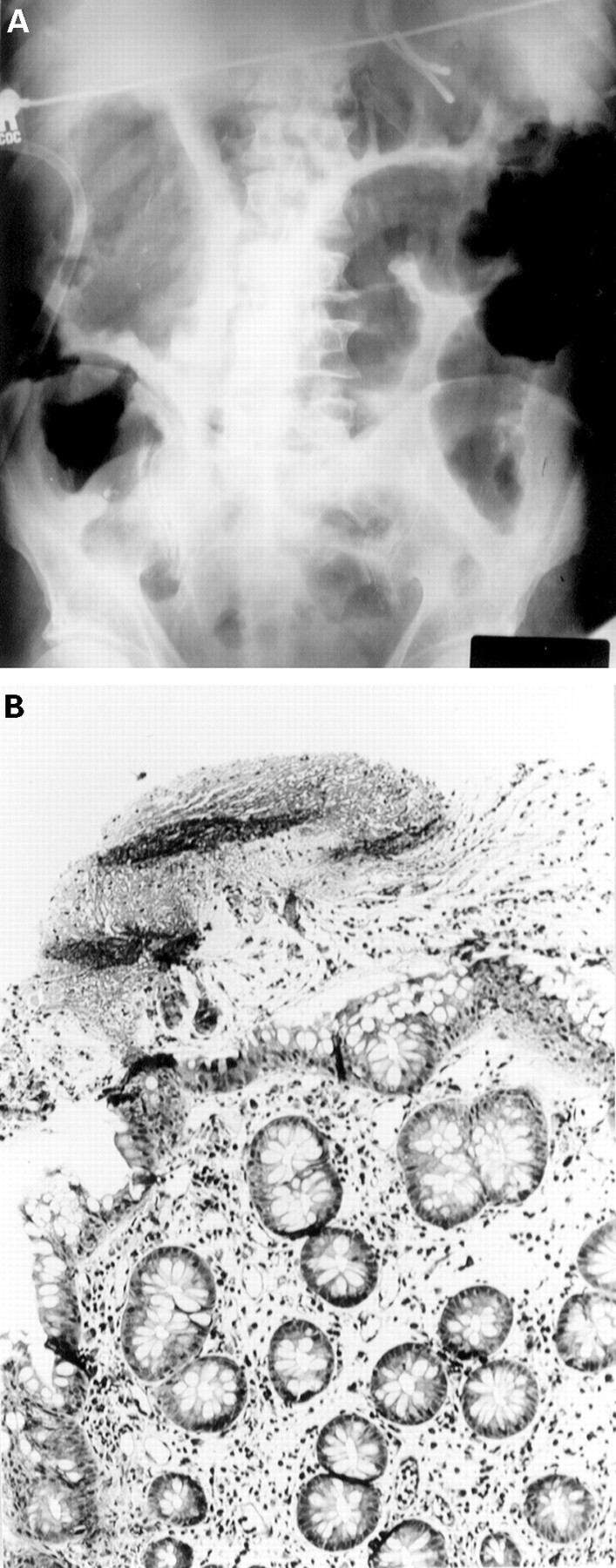
A 64 year old man underwent left upper lobectomy for large cell lung cancer. Intravenous vancomycin and ceftazidime were administered postoperatively for the treatment of pneumonia. Six days after surgery he developed diarrhoea, cramping abdominal pain, a fever of 102°F (38.9°C), diffuse abdominal tenderness, and abdominal distension. A stool test for C difficile cytotoxin was positive and he was treated with oral metronidazole (500 mg, six hourly). An abdominal radiograph showed thickening of the wall of the colon with thumbprinting (fig 2A). Flexible sigmoidoscopy was performed three days later because of increasing abdominal pain and distension, and showed pseudomembranous colitis (fig 2B). Oral vancomycin (250 mg, six hourly) was initiated. Nine days later he showed no improvement and had continuing diarrhoea, abdominal discomfort, and intermittent fevers. Intravenous immunoglobulin (200 mg/kg) was administered. Within 24 hours his diarrhoea and fever resolved and did not recur.
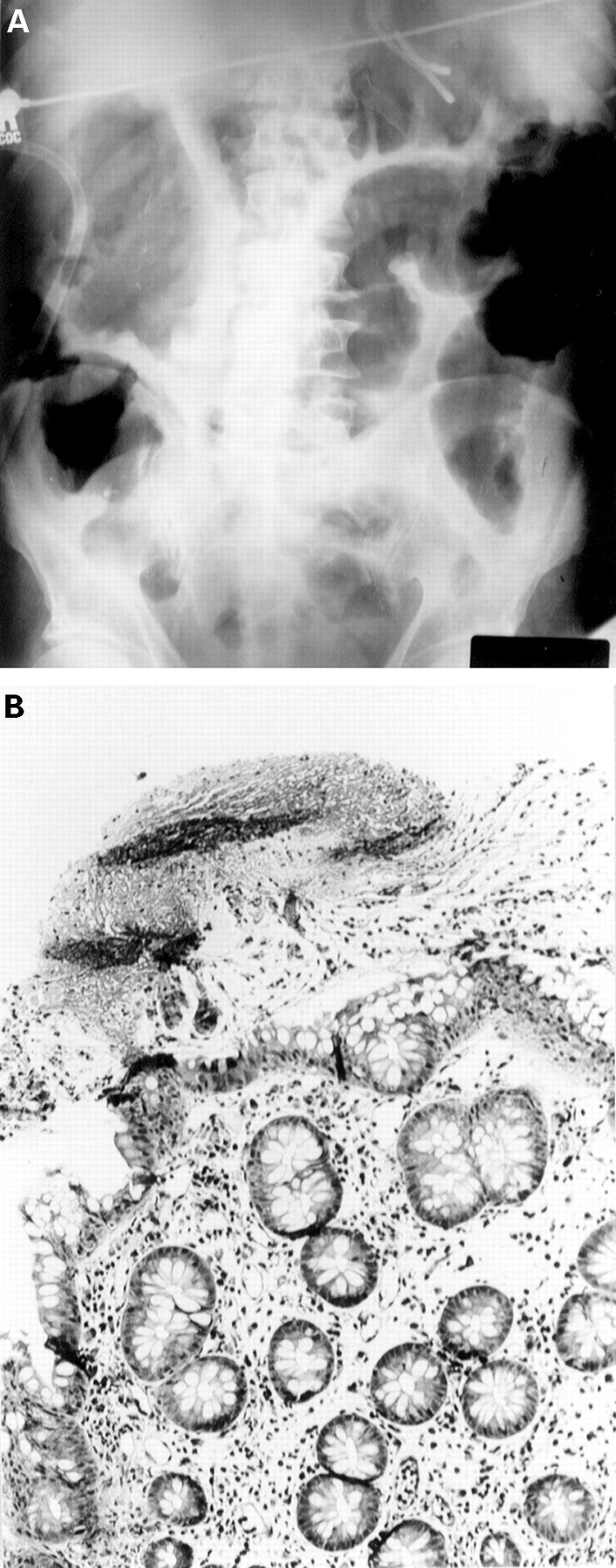
: Plain abdominal radiograph of patient 2 showing colonic dilatation and thickening of the colonic wall consistent with notable mucosal oedema (A). Photomicrograph of sigmoidoscopic biopsy specimen showing acutely inflamed colonic mucosa and an overlying pseudomembrane (B).
C DIFFICILE ANTITOXIN ACTIVITY IN HUMAN IMMUNOGLOBULIN PREPARATIONS
The rapid clinical response of these two patients to intravenous administration of normal pooled human serum immunoglobulin led us to test a variety of human IgG preparations for neutralising antibodies against C difficile toxins A and B.
All nine of the human immunoglobulin preparations tested contained IgG against C difficile culture filtrate (fig 3A). Antibody levels varied slightly with an approximately fourfold difference in antibody titre between the preparations with the highest and lowest antibody levels. We also measured IgG levels against purified C difficile toxin A and toxin B. A representative result for an immunoglobulin preparation with mid-range anti-C difficileIgG levels is presented in fig 3B (this particular preparation is identified by an arrow in fig 3A). All preparations contained IgG against both C difficile toxin A and toxin B as measured by ELISA.

{kind=link}
{kind=link}
{kind=link}
: C difficile antitoxin activity in human immunoglobulin preparations. (A) Anti-C difficile culture filtrate IgG levels measured by ELISA in commercially available pooled normal human immunoglobulin preparations. Three lots from each of three suppliers were studied (Alpha Therapeutic Corporation (open triangle), Armour Pharmaceutical Company (open square), and Baxter Healthcare Corporation (open circle). (B) IgG levels against C difficile culture filtrate (open circle), toxin A (open triangle), and toxin B (open square) in a representative immunoglobulin preparation (denoted by the arrow in A).
Finally, we determined whether pooled human immunoglobulin was capable of neutralising the cytotoxic effects of C difficiletoxins. All nine preparations neutralised C difficileculture filtrate cytotoxicity at IgG concentrations of 0.4–1.6 mg/ml. Control serum from a healthy volunteer who lacked specific antibodies against C difficile toxin A or toxin B failed to neutralise the cytotoxicity of C difficile culture filtrate in this assay.
Discussion
Most patients who develop C difficile diarrhoea respond promptly to either oral metronidazole or vancomycin.1 ,26 Diarrhoea may recur when these agents are discontinued but even then almost always resolves quickly when antimicrobial therapy is resumed. Persisting diarrhoea despite appropriate treatment with metronidazole and vancomycin, as occurred in both patients in this report, is unusual. Both patients also had severe colitis as evidenced by pseudomembrane formation, thickening of the colonic wall, abdominal tenderness, and abdominal distension. Severe, unresponsive pseudomembranous colitis may result in colonic perforation, septicaemia, and death.1 ,27-30 Colectomy may be life saving in these circumstances. However, many patients are considered unfit for colectomy because of advanced age and severe coexisting medical problems. Even those who are considered fit to undergo colectomy for severe pseudomembranous colitis have a mortality rate of approximately 50%.27-30 Thus it was felt that intravenous immunoglobulin treatment for unresponsive pseudomembranous colitis was justified for the two patients presented in this report. In both instances there was rapid clinical improvement immediately following immunoglobulin administration.
Both patients in this report had recognised risk factors for C difficile colitis including antibiotic treatment, admission to hospital, advanced age, malignancy, and recent major surgery.1 ,2 ,27 ,31 ,32 The elderly and those who experience major surgery or trauma are known to have impaired antibody responses against a range of antigens and this may include reducedC difficile antitoxin production.14 ,16 ,33 ,34 Neither patient had received cytotoxic chemotherapy at the time of onset of diarrhoea but the first patient had a lymphoma which may also be associated with diminished antibody production in response to antigenic challenge.
A number of previous studies have reported low serum antibody levels against C difficile toxins in patients with severe and prolonged C difficile colitis.14 ,18-23Elderly individuals, who are most likely to develop C difficile diarrhoea, may also have lower levels of neutralising antitoxin in their serum.16 If inadequate antibody production does indeed contribute to more severe or more prolonged disease, intravenous administration of preformed antitoxin may be beneficial. Passive immunotherapy, either oral or parenteral, is effective in preventing C difficile enterocolitis in animals but little information is available for humans.14 ,24 ,35-37 The largest study to date is our report of intravenous immunoglobulin administration to children with recurrent C difficile diarrhoea.21 ,38 ,39 In that study we demonstrated a notable increase in serum antitoxin A levels following immunoglobulin administration. In this study both patients were treated urgently with immunoglobulin and, unfortunately, serum was not saved to allow measurement of their serum antitoxin antibody levels.
As C difficile colitis is toxin mediated we assume that the immunoglobulin acts by binding and neutralising C difficile toxins. The intravenous administration of 150 mg/kg of immunoglobulin results in serum IgG levels of greater than 5 mg/ml whereas toxin neutralising activity is evident in vitro at IgG concentrations of approximately 1 mg/ml.40 Thus neutralising levels of IgG against C difficile toxins are readily achieved in the blood following immunoglobulin infusion. However, the precise mechanism of action of intravenous immunoglobulin is still not entirely clear since, to be effective, IgG antitoxin must leave the circulation and bind to toxins A and B within the colonic lamina propria or intestinal lumen.9 ,14 ,41 This may occur as a result of the exudation of serum proteins across an inflamed colonic mucosa.
Our first patient had a recurrence of C difficilediarrhoea four weeks after immunoglobulin infusion. This may simply be the result of discontinuing metronidazole and vancomycin three weeks earlier. However, the timing of her relapse is also consistent with the expected time course of degradation of intravenously administered human IgG.40
The animal and human studies discussed earlier indicate that normal pooled human immunoglobulin is a rational therapy for severe C difficile colitis particularly in cases where standard antimicrobial agents prove ineffective. Immunoglobulin treatment carries some risks but these are relatively small in the context of acutely ill patients with severe colitis who are often elderly and debilitated and already receiving multiple medications. A controlled prospective study would be needed to examine properly the efficacy of immunoglobulin in these circumstances. However, the uncommon and urgent nature of this condition makes such a study logistically difficult. The two cases reported here suggest that passive immunotherapy with pooled normal human immunoglobulin may be a useful addition to metronidazole and vancomycin and may hasten recovery or avert colectomy in patients with severe, refractory pseudomembranous colitis.