Article Text

Abstract
Background—It has recently been shown that humoral antigastric autoreactivities occur in a substantial number ofHelicobacter pylori infected patients.
Aims—To analyse the relevance of such antigastric autoantibodies for histological and serological parameters of the infection as well as for the clinical course.
Methods—Gastric biopsy samples and sera from 126 patients with upper abdominal complaints were investigated for evidence of H pylori infection using histology and serology. Autoantibodies against epitopes in human gastric mucosa were detected by immunohistochemical techniques. Histological and clinical findings of all patients were then correlated with the detection of antigastric autoantibodies.
Results—H pylori infection was significantly associated with antigastric autoantibodies reactive with the luminal membrane of the foveolar epithelium and with canalicular structures within parietal cells. The presence of the latter autoantibodies was significantly correlated with the severity of body gastritis, gastric mucosa atrophy, elevated fasting gastrin concentrations, and a decreased ratio of serum pepsinogen I:II. Furthermore the presence of anticanalicular autoantibodies was associated with a greater than twofold reduced prevalence for duodenal ulcer.
Conclusion—The data indicate that antigastric autoantibodies play a role in the pathogenesis and outcome of H pylori gastritis, in particular in the development of gastric mucosal atrophy.
- gastritis
- Helicobacter pylori
- autoimmunity
- gastric atrophy
Statistics from Altmetric.com
It is now well accepted that colonisation of the gastric mucosa with Helicobacter pylori leads to chronic active gastritis not only in man but also in animal models.1-5 Moreover, the association of H pylori infection with further gastroduodenal diseases, such as duodenal and gastric ulcer,6 ,7 gastric atrophy,8 gastric mucosa associated lymphoid tissue (MALT) type lymphoma,9 ,10 and gastric carcinoma,11and the significant reduced risk for ulcer relapse after H pylori eradication,12 ,13 indicate that this bacterium plays an important role in the pathogenesis of gastroduodenal pathology.
At present it is not clear why H pylori infection leads to different diseases in different patients. It is possible that the diverse courses of H pylori infection might be due to distinct strains expressing certain bacterial virulence factors.14 ,15 However, the role of host factors inH pylori infection which also contribute to the final outcome of infectious diseases has been far less examined.16 In H pylori gastritis the most obvious host reaction is the acquisition of MALT in the gastric mucosa, which could meet the requirement for antigastric autoimmune reactions.
Our previous findings and the work of other groups have provided evidence for humoral antigastric autoimmune reactions existing in association with H pylori gastritis.17-19The aim of this study was to investigate the relevance of antigastric autoantibodies for histological and clinical parameters of H pylori infection.
Material and Methods
One hundred and twenty six consecutive patients (72 men, 54 women, median age 54 years, range 15–86 years), who underwent diagnostic oesophagogastroduodenal endoscopy for upper abdominal complaints, were included in our study.
From all patients four biopsy specimens, two from the gastric antrum and two from the corpus mucosa, were examined for the presence, severity, and distribution of gastritis, as well as for intestinal metaplasia and atrophy on staining with haematoxylin and eosin. Gastritis was classified according to the Sydney system20and to the ABC system.21 H pyloricolonisation was histologically detected in Warthin-Starry stains.
Serum samples were taken from all patients shortly before or soon after endoscopy and were screened for the presence of IgG antibodies reactive with H pylori in an enzyme linked immunosorbent assay (ELISA) as previously described.17 Correlation of serological and histological detection of H pylorirevealed a sensitivity of 84% and a specificity of 81% (data not shown). Forty two patients were taking proton pump inhibitors. Seven of the latter group were also taking amoxycillin for a maximum of one week. In three of these patients H pylori infection was only detectable by ELISA. This finding was considered when determining the performance criteria of the ELISA.
Antigastric autoantibodies reactive with human gastric mucosa were detected using an immunohistochemical method described previously.17 Briefly, heterologous formalin fixed gastric biopsy samples from antrum and corpus without pathological alterations were incubated overnight with the patient’s serum diluted 1/100. After washing, 1/10 diluted alkaline phosphatase conjugated rabbit antihuman IgG (Dako, Hamburg, Germany) was added. Colour was developed with fast red. In a negative control with omission of serum, immunohistochemical reactivity could not be detected in the antrum or corpus.
All serum samples were also tested by immunofluoresence for classic antiparietal cell antibodies using native rat tissues (HISS Diagnostics, Freiburg, Germany).
Fasting gastrin concentrations were measured by a gastrin radioimmunoassay kit (GASK-PR, CIS Biointernational, France). Normal values ranged between 28 and 115 μU/ml. The concentrations of pepsinogen I and II were determined using a radioimmunoasssay kit (Sorin Biomedica, Saluggia, Italy).
Statistical correlations of qualitative parameters were tested with the χ2 method. Statistical analysis of gastrin concentrations and of the pepsinogen I:II ratio was performed by means of the Mann-Whitney U test. A value of p⩽0.05 was considered significant. With regard to gastrin and pepsinogen concentrations, patients treated with proton pump inhibitors were excluded from the analysis, since it is known that these drugs lead to higher fasting gastrin and pepsinogen concentrations.22
The study protocol was examined by the ethics committee of the University of Erlangen-Nürnberg. All patients gave their informed consent prior to inclusion in the study.
Results
PATIENTS AND HISTOLOGY
Thirty two patients had normal gastric mucosal histology. Four patients had autoimmune gastritis (type A gastritis), three of which had pernicious anaemia. Five patients had gastric mucosal alterations diagnosed as chemically induced gastritis (type C gastritis). Eighty four patients had type B chronic gastritis, 79 of whom (94%) were histologically or serologically positive for H pylori. The age profile of H pylori infected patients did not differ from that of uninfected patients (mean age 54.5 years, range 25–85 years; and 53.7 years, range 15–86 years, respectively). One patient had coeliac sprue and showed moderate chronic gastritis in the antrum and lymphocytic gastritis in the antrum and body.
Twenty eight patients had intestinal metaplasia. Atrophic mucosal alterations—that is, complete or incomplete reduction of gastric glands, were detectable in 18 patients.
ENDOSCOPY
At endoscopy, 24 patients were shown to have duodenal ulcer, 16 of whom were positive for H pylori infection detected by serology or histology. Fifteen patients had gastric ulcer, 11 of whom were H pylori positive. Of the 42 patients treated with proton pump inhibitors, 28 had duodenal and/or gastric ulcers. The age profile of H pylori infected patients with duodenal and/or gastric ulceration was not significantly different from that of non-ulcer patients (mean age 55.9 years, range 15–86 years; and 52.7 years, range 21–78 years, respectively).
ANTIGASTRIC AUTOANTIBODIES
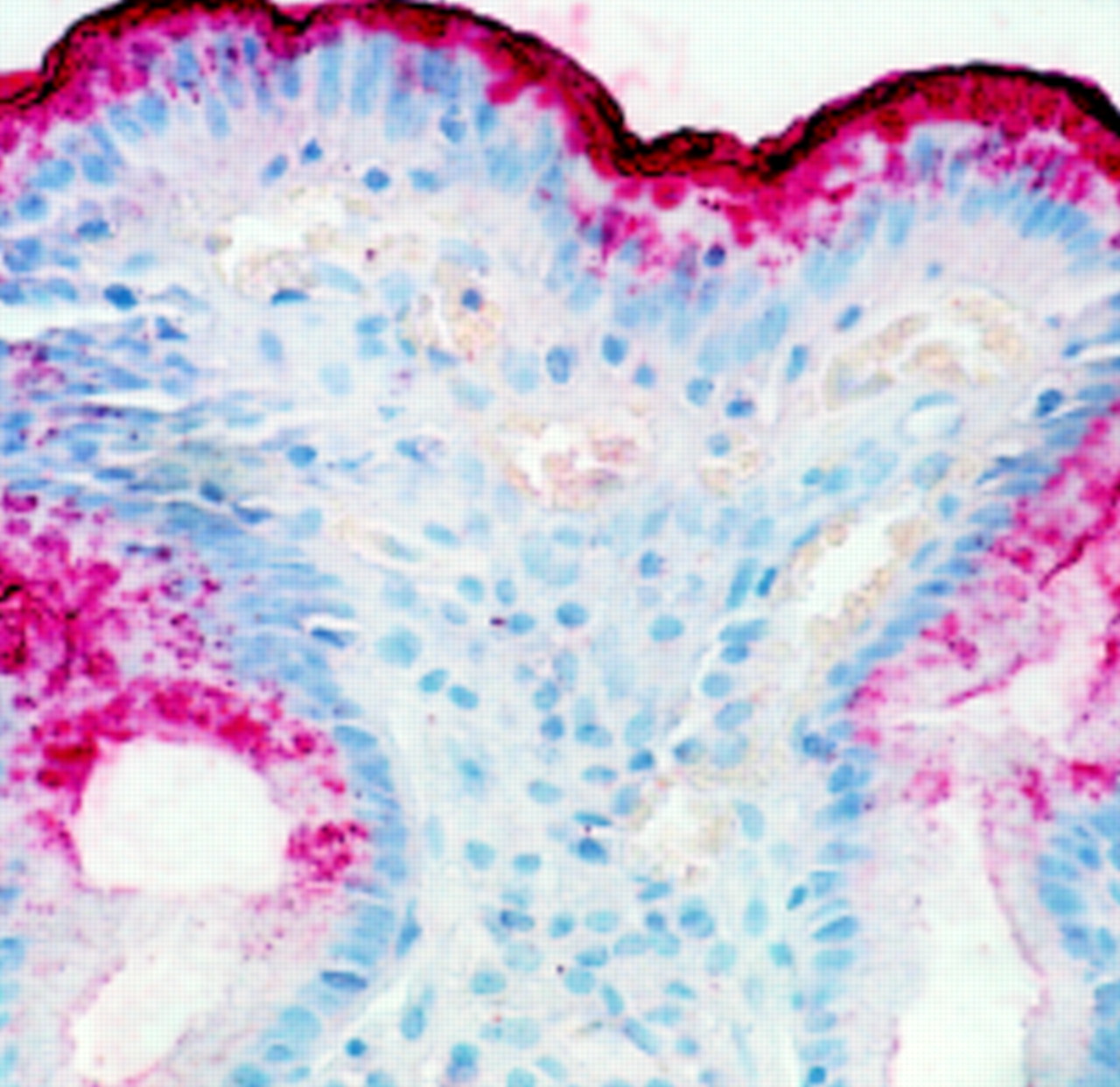
Antigastric autoantibodies could be detected by immunohistochemistry in 51/126 patients when tested on human gastric tissue. Seventeen patients showed only autoantibodies reactive with the luminal membrane of foveolar epithelial cells in the antrum and the body (fig 1), and 20 patients showed only a distinctive immunoreactivity with canalicular structures within the parietal cells in the body (fig 2). Fourteen patients showed both types of autoreactivity.

: Antiluminal antigastric reactivity against the apical membrane of foveolar epithelium cells in the human gastric antrum and body (original magnification ×40).

: Anticanalicular antigastric autoreactivity against canaliculi within parietal cells of the human gastric body (original magnification ×40).
Using immunofluoresence on rat tissue, antiparietal cell antibodies could be found in nine patients, three with classic autoimmune gastritis and six with H pylori gastritis. All of these nine patients were also positive for anticanalicular autoantibodies using human gastric tissue (table 1).
Type of gastritis, H pylori infection, and antigastric autoantibodies
H PYLORI INFECTION AND ANTIGASTRIC AUTOANTIBODIES
The presence of anticanalicular as well as antiluminal autoantibodies was significantly correlated with detection of H pylori by both ELISA and histology: of the 34 patients positive for anticanalicular autoantibodies, 27 were positive for H pylori by ELISA and 23 showed H pylori infection at histology (p<0.001 and p<0.05, respectively). Of the 31 patients positive for antiluminal autoantibodies, 22 were positive for H pylori by serology and 21 were positive by histology (p<0.05 for both). Of the 79 patients positive for H pylori by either serology or histology, 16 had anticanalicular autoantibodies, 12 had antiluminal autoantibodies, and 11 showed both types of autoreactivity. The age profile of H pylori infected patients with antigastric autoantibodies was not significantly different from that of those without these autoantibodies (mean age 54.9 years, range 25–83 years; and 53.2 years, range 15–86 years, respectively).
HISTOLOGICAL ALTERATIONS AND ANTIGASTRIC AUTOANTIBODIES
When the group of patients positive for H pylori by histology or serology was analysed, a significant association of either anticanalicular or antiluminal antigastric autoantibodies with the presence of moderate to severe corpus gastritis could be found (p<0.001 and p⩽0.05, respectively). Furthermore, a strong association between anticanalicular autoantibodies and atrophic changes in the gastric mucosa of the antrum or body was detectable (p<0.01). No significant correlation between the severity of antral gastritis and the presence of either type of antigastric autoantibodies could be found (table 2).
Correlation between antigastric autoantibodies and severity of H pylori gastritis and gastric atrophy
GASTRIN CONCENTRATIONS AND ANTIGASTRIC AUTOANTIBODIES
Fasting serum gastrin concentrations in patients with histologically or serologically proved H pylori infection with anticanalicular autoantibodies were significantly higher than both those in H pylori infected patients without these autoantibodies and in healthy controls (mean values 56.2, 43.1, and 39.6 μU/ml, respectively; p<0.05). No significant association between antiluminal autoantibodies and raised gastrin concentrations could be found. The four patients with type A gastritis had the highest gastrin concentrations (mean value 387 μU/ml) (fig3).

: Fasting serum gastrin concentrations in healthy controls, patients with H pylori gastritis with and without anticanalicular autoantibodies, and patients with type A gastritis.
PEPSINOGEN I:II RATIO AND ANTIGASTRIC AUTOANTIBODIES
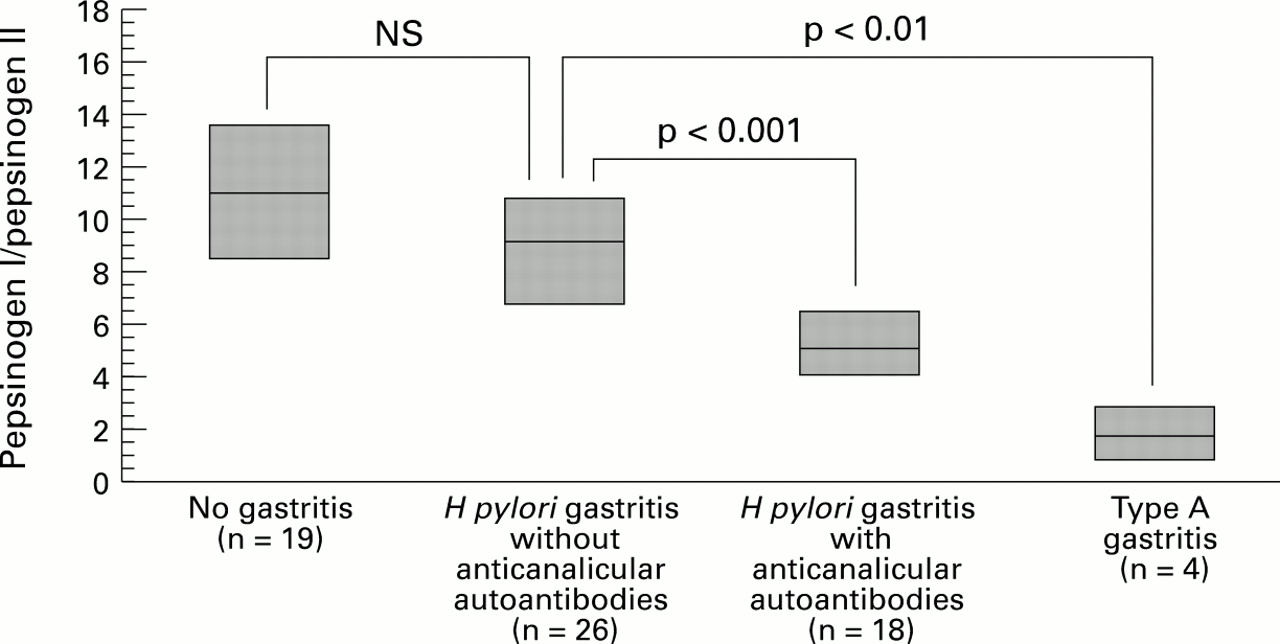
In the group of H pylori positive patients with anticanalicular autoantibodies the pepsinogen I:II ratio was significantly decreased compared with that in H pyloripositive patients without these autoantibodies or in the healthy controls (mean values 5.10, 9.01, and 10.61, respectively; p<0.001). Patients with classic autoimmune gastritis had the lowest pepsinogen I:II ratio (fig 4). Detection of antiluminal autoantibodies was not significantly associated with an altered pepsinogen I:II ratio.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
: Fasting pepsinogen I:II ratio in healthy controls, patients with H pylori gastritis with and without anticanalicular autoantibodies, and patients with type A gastritis.
ANTIGASTRIC AUTOANTIBODIES AND PREVALENCE OF DUODENAL ULCER
At endoscopy 16/79 H pylori positive patients were shown to have duodenal ulcer. In three, anticanalicular autoantibodies were present; 13 showed no anticanalicular autoreactivity. The prevalence of duodenal ulcers in the group of patients without anticanalicular autoantibodies was more than twice as high as that in the group with anticanalicular autoantibodies (25% v 11%). However, because the number of patients with duodenal ulcer was low, a significant correlation could not be shown. There was no association between the presence of antigastric autoantibodies of either type and gastric ulceration.
Discussion
This paper presents a systematic analysis of the relevance of antigastric autoantibodies in H pylori gastritis. We and others have previously shown that autoantibodies against gastric epitopes occur in about 50% of H pylori infected patients with upper gastrointestinal complaints. We have described two different in situ binding sites for these autoantibodies, one at the luminal membrane of the foveolar epithelium, the other at canalicular structures within parietal cells; the latter showed the highest correlation with H pylori infection.17 ,18This high prevalence of antigastric autoreactivity was confirmed in this study. Furthermore, according to our data, this type of autoantibody is correlated with histological and clinical manifestations of H pylori infection. Thus, the occurrence of anticanalicular autoantibodies correlates with the severity of body gastritis, and atrophic changes of the gastric mucosa, as well as with elevated basal serum gastrin concentrations and a decreased pepsinogen I:II ratio. Interestingly, the presence of anticanalicular autoantibodies is correlated with a greater than twofold reduced prevalence of duodenal ulcer. Although it is evident that the parameters mentioned are not independent of each other, they represent different facets of gastric mucosal atrophy. This indicates that autoantibodies to canaliculi are either responsible for the development of atrophy or are at least a marker for other pathogenic factors leading to atrophic changes in the mucosa.
Recently, Negrini et al also reported two different in situ binding sites for antigastric autoantibodies in H pylori gastritis.23 These autoreactivities were not simultaneously present in all patients positive for antigastric autoantibodies, indicating two different types of autoantibodies. In their study the presence of these autoantibodies seemed to be relevant for certain histological alterations such as the density of periglandular lymphocytic infiltrations and glandular atrophy, which is comparable with our results. However, in our study a more detailed evaluation for both types of autoreactivity—against mucous cells and against canaliculi of parietal cells—was performed. Furthermore, we also analysed certain clinical parameters, such as fasting gastrin concentrations and the pepsinogen I:II ratio, which support the histological diagnosis of gastric mucosal atrophy.
The mechanisms leading to the formation of antigastric autoantibodies in chronic H pylori infection and to atrophic gastritis are still under investigation. Negrini et al and Appelmelket al suggest molecular mimicry between epitopes onH pylori and Lewis blood group antigens expressed on gastric epithelial cells.18 ,19 ,23
It is possible however, that apart from this hypothesis other autoimmune mechanisms are responsible for the generation of antigastric autoantibodies. Since almost no immunological surveillance exists in the normal gastric mucosa, one can describe this region as an immunologically privileged site,24 which loses its virginal status by colonisation with H pylori, leading to expression of major histocompatibility complex class II antigens on gastric epithelial cells25-27 and aggregation of a dense lymphoplasmacellular infiltrate within the gastric mucosa.28 Thus, in immunological terms, H pylori gastritis represents chronic antigen presentation and immunostimulation in acquired MALT. It is possible that this unique condition leads to adequate immunological exposure of self epitopes to reactive immunocompetent cells. Cellular and/or humoral autoreactivity against autoantigens located on cells in the body mucosa could result in an increased rate of apoptosis and lead to atrophic alterations.29 Furthermore, autoantibodies against epitopes on canalicular structures within parietal cells, where the major autoantigen in classic autoimmune gastritis is located,30 could also inhibit parietal cell function in patients with H pylori gastritis.31 This could lead to the unchanged or even decreased basal acid secretion despite raised gastrin concentrations in H pylori infected subjects without duodenal ulcer32-36 —a possible explanation for the reduced rate of duodenal ulcers in the group with anticanalicular autoantibodies found in our study. However, these hypotheses need to be investigated further.
Our data provide evidence that autoimmune reactions play a role in the final outcome of H pylori gastritis. Therefore one might discuss whether a strict aetiological distinction between autoimmune gastritis and H pylori associated gastritis is still possible. One might even speculate that the H pyloriassociated multifocal atrophic gastritis proposed by Correa37 or the so called AB gastritis proposed by Glass and Pitchumoni38 corresponds to a special type of H pylori gastritis which develops anticanalicular autoreactivity and gastric atrophy. Further investigations into antigastric autoimmune reactivity in H pylori infection might lead to an understanding of the long term outcome of gastritis.
Acknowledgments
We thank Dr M Eck for kindly providing the H pylori lysate, Dr A Katalinic for his skilful help in statistical analysis, and S Hoppe, M Rembeck, and C Winkelmann for excellent technical assistance. Part of this work was presented in abstract form at the 8th International Workshop on Gastroduodenal Pathology and Helicobacter pylori, October 1996, Copenhagen, Denmark. This work was supported by the Interdisciplinary Center for Clinical Research at the University of Erlangen-Nürnberg.