Article Text

Abstract
Background—Endoscopic sphincterotomy has been shown to inhibit stone formation in the gall bladder of experimental animals.
Aims—To investigate the alterations in bile composition and gall bladder motility after endoscopic sphincterotomy.
Patients—A study was performed of gall bladder bile composition and gall bladder motility in patients with gallstone disease ((n = 20; age 40–60 years, median age 55 years: seven men), with gall bladder calculi (n = 12) and with diseased gall bladder (chronic inflammation) without gall bladder calculi (n = 8)), who had received endoscopic sphincterotomy for common bile duct stones. Age and sex matched disease controls comprised 20 patients with gallstone disease but without stones and an intact sphincter of Oddi (with gall bladder calculi (n = 10) and diseased gall bladder without gall bladder calculi (n = 10)).
Methods—Gall bladder motility was assessed by ultrasound. Duodenal bile collected by nasoduodenal tube after stimulation of gall bladder by intravenous ceruletid infusion was analysed for cholesterol, phospholipid, and bile acid concentrations, cholesterol saturation index, and nucleation time.
Results—There was a significant reduction in mean (SEM) fasting volume (12.5 (1.7) ml v 26.4 (2.5) ml; p<0.001) and mean (SEM) residual volume (4.34 (0.9) ml v14.7 (0.98) ml; p<0.001), and increase in mean (SEM) ejection fraction (65.7 (4.2)% v 43.6 (5.52)%; p<0.001) and mean (SEM) rate constant of gall bladder emptying (−0.031/min v−0.020/min; p<0.01) in patients who had been subjected to endoscopic sphincterotomy. Median nucleation time was significantly longer (17 days v 6 days; p<0.006) in treated patients. There was a reduction in total mean (SEM) lipid concentrations (6.73 (0.32) g/dlv 7.72 (0.84) g/dl; p<0.05), cholesterol (5.6 (1.5) mmol/l v 10.3 (2.23) mmol/l; p<0.001) and CSI (0.72 (0.15) v 1.32 (0.31); p<0.001). There was no significant change in mean (SEM) phospholipid (25.6 (3.5) mmol/l v23.4 (6.28) mmol/l) and bile acid (93.7 (7.31) mmol/l v105.07 (16.6) mmol/l) concentrations.
Conclusions—After endoscopic sphincterotomy there was enhanced contractility of the gall bladder, accompanied by a prolongation of nucleation time and reduction in cholesterol saturation index.
- gall bladder emptying
- gall bladder contractility
- nucleation time
- cholesterol saturation index
- gallstones
- endoscopic papillotomy
Statistics from Altmetric.com
- gall bladder emptying
- gall bladder contractility
- nucleation time
- cholesterol saturation index
- gallstones
- endoscopic papillotomy
Endoscopic sphincterotomy (ES) is widely used for the extraction of common bile duct (CBD) stones in both cholecystectomised patients and those with an intact gall bladder. Hutton et al 1 ,2 were the first to show in a prairie dog model that ablation of the sphincter of Oddi inhibited gallstone formation despite continued supersaturation of bile. It was further shown that ablation of the sphincter both facilitates passage of glass beads of varying sizes implanted in the canine gall bladder and improves gall bladder emptying.5 Long term follow up studies of patients with gall bladders in situ after endoscopic clearance of CBD stones showed that the incidence of new stone formation was almost negligible.3 ,4 Isolated clinical observations suggested that ES may enhance gall bladder emptying in humans.6 ,7 Studies performed by Liet al 8 suggested that sphincterotomy may reduce stone formation by inhibiting the effects of lithogenic bile on gall bladder muscle contractility and enhancing the ability of muscle to empty the lithogenic bile. Alterations in bile composition have been reported both in hepatic and gall bladder bile after sphincter ablation.9-13 These experimental data suggest significant alterations in gall bladder motility and bile composition after sphincter ablation9 and emphasise the need for a case control study on the effect of ES on gall bladder bile composition, nucleation time, and motility in man. We therefore studied these parameters in patients who had had ES for CBD stones while having their gall bladders in situ.
Materials and methods
We studied 20 patients with intact gall bladders, who had received ES for CBD stones and had a clear CBD as shown by endoscopic retrograde cholangiopancreaticography three months before inclusion in the study. Patients with small shrunken gall bladders (fasting volume less than 5 ml) were excluded. These patients were classified into two groups: (a) those with gall bladder calculi (GS+) (n = 12; age 40–60, median age 55; eight women and four men) and (b) those with diseased (chronically inflamed) gall bladders without gall bladder calculi (GS−) (n = 8; age 45–55, median age 54; five women and three men). These patients had a single cholesterol stone extracted from the CBD after ES. Stones collected after stool sieving were subjected to chemical analysis14 in 15 patients (eight in the GS+ group and seven in the GS− group) and had cholesterol contents greater than 50% of total dry weight. Age and sex matched (table 1) disease controls with intact papillary sphincters included: (a) 10 patients with gall bladder calculi but without CBD stones (CGS+) and (b) those who had diseased gall bladders without gall bladder calculi and CBD stones (CGS−, n = 10). These patients had received successful extracorporeal shock wave lithotripsy (n = 3) or bile acid therapy (n = 7) for gall bladder calculi three months before this study. Every patient was subjected to detailed clinical and biochemical examination. Oral cholecystography was carried out in both study and control patients to assess gall bladder function. Gall bladder wall thickness was measured by ultrasound in all the patients.
Patient characteristics
MEASUREMENT OF GALL BLADDER EMPTYING BY ULTRASOUND
Gall bladder volume and emptying were measured by real time ultrasonography, using a 3.5 MHz transducer. Patients were scanned supine in the right anterior oblique position by an experienced sonologist (SSB). The gall bladder was visualised in the longitudinal and transverse planes, and measurements of maximum length, width, and height were taken in triplicate. The volume of the gall bladder was subsequently calculated using the ellipsoid method (volume = 0.52 × length × width × height).15
All patients were studied at 09.00 hours after an overnight 12 hour fast. Fasting volume of the gall bladder (FV) represented the mean of three volume measurements taken five minutes apart immediately before the start of the ceruletid infusion (Takus “R”; Farmitalia Carlo Erba Gmbh, Germany; dose 50 ng/kg per hour) for 30 minutes. During the infusion the gall bladder volume was measured every five minutes for 30 minutes. The smallest gall bladder volume observed at any time during ceruletid infusion was termed the residual volume (RV). The gall bladder ejection fraction (EF%) was calculated from the equation EF% = 1 − (RV/FV) × 100. The rate constant of gall bladder emptying was calculated by log linear regression of gall bladder volume versus time.16
DUODENAL BILE
After a 12 hour overnight fast, patients were subjected to nasoduodenal intubation with a Bilbao-Dotter tube which was positioned using fluoroscopy. Dark thick viscous duodenal bile17was collected after intravenous infusion of ceruletid for 30 minutes, thoroughly mixed, and divided into four aliquots. One aliquot was examined within 30 minutes under a polarising microscope, the second was stored at 37°C for repeat microscopic examination if required, the third was processed immediately for estimation of nucleation time, and the fourth was stored in a sealed glass vial at −20°C for chemical examination.
BILE MICROSCOPY
A 2.5 ml sample of bile was centrifuged at 2000 rpm for 10 minutes; the supernatant was discarded and the sediment examined on a glass slide under the polarising microscope. The number of cholesterol crystals under the coverslip area (22 × 50 mm) was counted at 10× magnification and recorded as the number of crystals per cover slip area. If no microcrystal was seen on the first examination, the sample of bile stored at 37°C in the incubator was examined after 24 hours.
NUCLEATION TIME OF BILE
Nucleation time was determined by the method of Holan et al 18 ,19 with minor modifications. After collection, 5 ml of bile was placed in a sterile ultracentrifuge tube and spun at 100 000 g for two hours. The clear middle isotropic phase was transferred to a sterile plastic vial. Immediately after ultracentrifugation, this sample was examined under a polarising microscope to confirm that no crystal was present. The isotropic phase was then incubated anaerobically at 37°C in the dark. Thereafter a drop of bile was examined daily for the appearance of cholesterol crystals. The nucleation time was defined as the number of days from the day of collection of bile to the first day that cholesterol crystals were seen.
CHEMICAL ANALYSIS OF BILE AND CALCULATION OF CHOLESTEROL SATURATION INDEX (CSI)
Both duodenal and gall bladder bile samples were subjected to chemical analysis for cholesterol,14phospholipids,20 and total bile acid21 . Total lipid concentration, defined as the sum of the cholesterol, phospholipids, and bile acid concentrations, was used as an indicator of bile concentration. CSI was calculated from Carey’s table.22 Bile samples with a CSI of greater than one were considered supersaturated.
Data in different groups were compared using the Wilcoxon rank sum test.
Results
GALL BLADDER MOTILITY
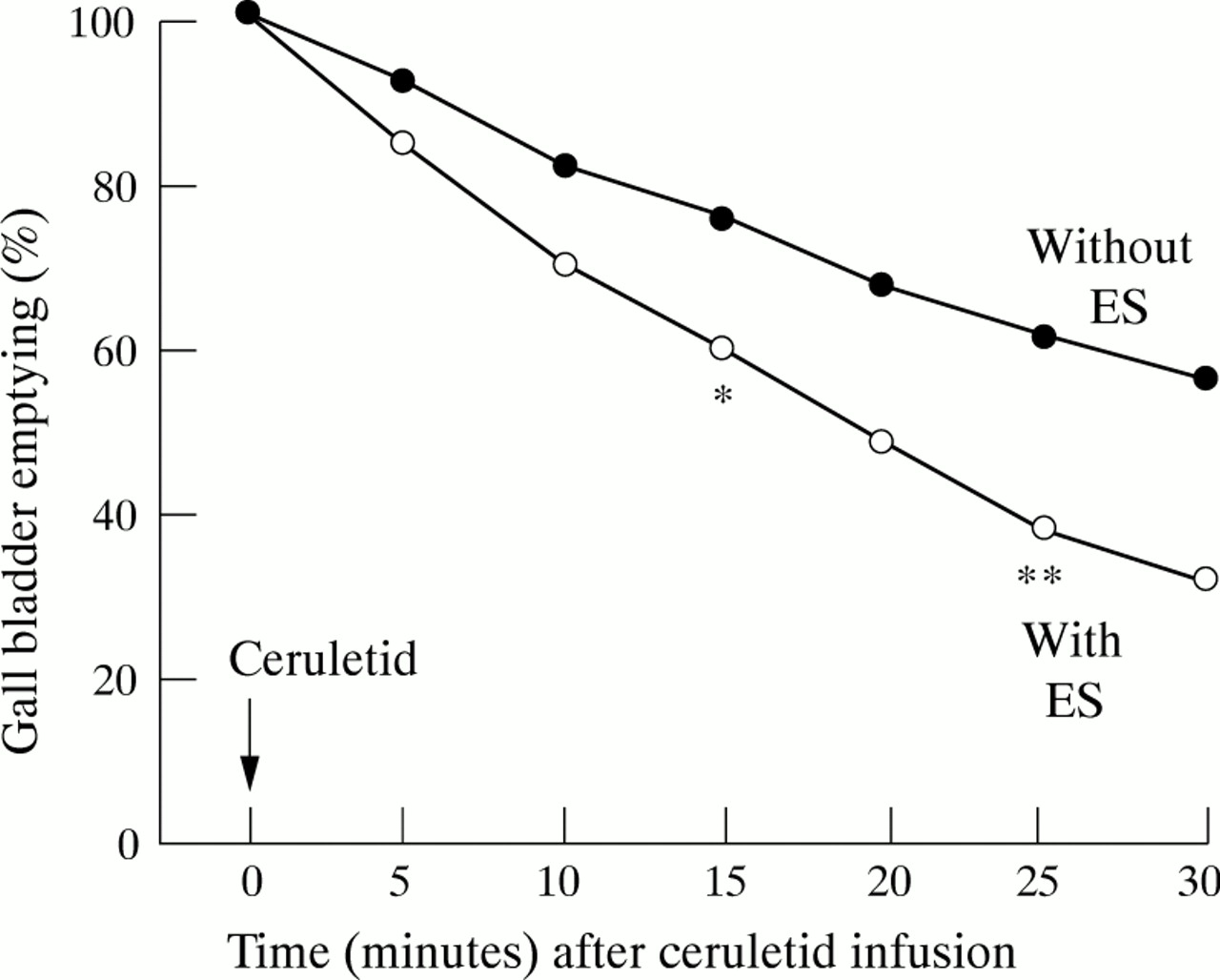
Table 2 shows that sphincterotomised patients had significantly smaller fasting and ceruletid stimulated residual gall bladder volumes than disease controls. They also had significantly higher gall bladder ejection fractions and rate constants of gall bladder emptying compared with disease controls. Figures 1 and 2 show the effect of sphincterotomy on the time course of gall bladder emptying after ceruletid infusion; the amount emptied is expressed as a percentage of the control scan fasting volume. The difference in gall bladder volume emptied was significantly higher after ES for each measurement taken at five minute intervals after the start of ceruletid infusion (figs 1 and 2). The rate constant of gall bladder emptying was significantly higher in post-sphincterotomy patients compared with disease controls in both the GS+ and GS− groups (−0.030/minv − 0.018/min, p<0.01; −0.032/min v−0.022/min, p<0.01 respectively).
Gall bladder fasting volume, residual volume, and ejection fraction in patients with or without sphincterotomy

Time course of percentage gall bladder emptying in patients with gallstones with and without sphincterotomy. *p<0.001, **p<0.001.

Time course of percentage gall bladder emptying in patients without gallstones with and without sphincterotomy. *p<0.001, **p<0.001.
BILE EXAMINATION
Bile microscopy
Bile from patients in the GS+ and GS− groups did not contain cholesterol crystals. In contrast the CGS+ and CGS− groups had cholesterol crystals on bile microscopy.
Nucleation time
Nucleation time was significantly longer (17 days v 6 days; p<0.006) in patients who had received ES. In GS+ patients, median nucleation time was 16 (range 13–21) days in post-sphincterotomy patients compared with five (3–10) days in disease controls (fig 3). In GS− patients median nucleation time was 18 (range 15–20) days in post-sphincterotomy patients compared with seven (range 5–10) days in disease controls (fig3).

{kind=link}
{kind=link}
{kind=link}
Nucleation time in patients with and without sphincterotomy. *p<0.006, **p<0.006.
Total lipid concentration and CSI
There was significantly lower total lipid concentration (6.73 (0.32) g/dl v 7.72 (0.84) g/dl; p<0.05), cholesterol (5.6 (1.54) mmol/l v 10.3 (2.23) mmol/l; p<0.001), and CSI (0.72 (0.15) v 1.32 (0.31); p<0.001) in patients who had been subjected to ES, while there were no differences in phospholipid (25.6 (3.5) mmol/l v 23.4 (6.28) mmol/l) and bile acid concentration (93.7 (7.31) mmol/l v 105.07 (16.6) mmol/l). Similar results were seen on comparing the two groups separately (table3).
Gall bladder bile composition and cholesterol saturation index in patients with or without sphincterotomy
Discussion
We have shown that patients who have had ES have greater gall bladder motility as reflected by decreased fasting and residual volumes and an increased ejection fraction and rate constant of gall bladder emptying. Also they have lower lithogenicity, cholesterol, and total lipid concentration in gall bladder bile without any reduction in bile acid and phospholipid concentrations.
Gall bladder emptying was abnormal in patients with gallstones. Impaired gall bladder emptying and reduced turn over of bile have been described previously in patients with gallstones.23 ,24 Our findings of enhanced gall bladder motility after ES are consistent with results of earlier studies.25 ,26 Sugiyama and Atomi25conclusively proved that ES causes significant improvement in gall bladder motility in humans and this effect lasts for more than five years. The improvement in gall bladder motility could be due to impaired gall bladder filling or enhanced emptying. Reduction in CBD pressure after sphincter destruction27 ,28 facilitates gall bladder emptying. Earlier studies showed that eliminating sphincter resistance decreases gall bladder filling.29 ,30
Our findings of altered bile composition after ES differs from those reported in earlier studies. No significant changes in hepatic bile composition were found in two different studies performed in dogs.11 ,12 Sauerbruch et al 10showed a reduction in total bile acid pool size after sphincterotomy in patients with intact gall bladders, but there was no difference in molar percentages of bile acids, cholesterol, and phospholipid or in mean CSI. Cohn et al 13showed reduction in lithogenicity with increase in lecithin and bile salts after sphincter of Oddi ablation. All these studies analysed hepatic bile while we studied duodenal bile. The only study analysing gall bladder bile after sphincter ablation was conducted in dogs, and showed unchanged biliary cholesterol levels but a decrease in the concentration of lecithin and bile salts, leading to an increased CSI.13 In the present study, there was a significant fall in cholesterol concentration after ES without any rise in bile acids and phospholipids; further, there was a significant reduction in total lipid concentration and CSI. The canine model used in this study may not faithfully reflect human biliary pathophysiology since the relative concentrations of cholesterol, bile salt, and phospholipid in canine bile differ from those of man.31 ,32 Also Cohn et al 13 studied healthy dogs with normal gall bladders whereas we studied humans with diseased gall bladders. The only human study analysing gall bladder bile after ES did not compare bile composition in patients with and without ES.33 Gall bladder bile composition may alter after ES either because of a change in gall bladder wall permeability as the result of regurgitation cholecystitis or rapid gall bladder bile turn over.1 ,2 ,13 ,34 At present, determination of biliary nucleation time is the best predictor for cholesterol gallstone formation.35 Our study has shown that after ES, biliary nucleation time was significantly prolonged compared with disease controls. The prolonged nucleation time in gall bladder bile in our study may be ascribed to (a) decreased total biliary lipids, (b) alteration in concentrations of pronucleating and antinucleating factors, and/or (c) improved gall bladder motility. It is reported that gall bladder mucosa is either impermeable to lecithin, bile salts, and cholesterol or absorbs a small fraction of biliary lipids. Permeability may be increased in the presence of bacterial contamination, which is commonly found after biliary sphincterotomy.13 ,36 This may cause selective reabsorption of bile constituents by the gall bladder mucosa.13 However, there is no direct evidence for selective reabsorption of bile constituents; therefore the idea of alterations in gall bladder content being due to selective reabsorption of bile constituents remains speculative. Sauerbruch et al 10 reported diminution of bile acid pool after ES in patients with an intact gall bladder. However, there were no alterations in bile acid pool in patients with cholecystectomy who already have smaller total bile acid pools.10 It is possible that duodenal and gall bladder bile have different lipid contents, although dilution cannot explain isolated low cholesterol concentration without significant difference in phospholipid and bile acid concentrations. Furthermore a dilution phenomenon is an unlikely explanation for the low cholesterol in patients who have had ES since in both groups (with ES and without ES) duodenal bile was analysed.
Experimental animal studies have shown reduced gallstone formation after sphincter- otomy.1 ,2 Similar observations have been made in long term follow up studies in patients with gall bladders in situ after ES.4 ,5 Our study further supports the possibility that sphincterotomy induces changes in bile composition and gall bladder motility which would reduce the risk of recurrent cholelithiasis.
In conclusion, ES significantly prolongs nucleation time, decreases cholesterol and total lipid concentration, and does not affect phospholipid and bile acid concentrations. It also enhances gall bladder motility in patients with diseased gall bladders. These results may explain the reduced recurrence of gall bladder calculi after ES.