Article Text

Abstract
Background—Diverticulitis and Crohn’s disease affecting the colon occur at similar sites in older individuals, and in combination are said to carry a worse prognosis than either disease in isolation. It is possible that diverticulitis may initiate inflammatory changes which resemble Crohn’s disease histologically, but do not carry the clinical implications of chronic inflammatory bowel disease.
Aims—To evaluate histological features and clinical outcome in individuals initially diagnosed histologically as having both Crohn’s colitis and diverticulitis.
Patients—Eleven consecutive individuals having a colonic resection showing histological features of both Crohn’s disease and diverticulitis.
Methods—Retrospective review of histological specimens, case notes, and discharge letters.
Results—In nine patients, the Crohn’s-like reaction was confined to the segment bearing diverticula. They had no clinical evidence of Crohn’s disease.
Conclusion—A Crohn’s-like inflammatory response can be a localised reaction to diverticulitis and does not necessarily indicate chronic inflammatory bowel disease.
- Crohn’s disease
- diverticulitis
- colitis
- histology
Statistics from Altmetric.com
Diverticulosis is a common condition in the Western world, affecting 35–50% of people over 60.1 ,2 Few of those affected are symptomatic, possibly only about 5%. Of those with symptoms, most can be treated medically, and only 7% of symptomatic individuals ultimately require surgery. Mortality from the disease is in the order of 2%, death usually following emergency surgery.3
Crohn’s disease of the colon has an estimated incidence of about 1.5–3.6 per 100 000.4 The sigmoid colon is involved in about 70% of these cases,3 with involvement of the distal colon and anorectum being more common in older age groups.5 Both Crohn’s colitis and diverticulitis are seen with sufficient frequency that unless one disease protects from the other, one would occasionally expect to see coincident disease. Early reports suggested that combined disease carried a worse prognosis than either disease in isolation, and advocated more aggressive treatment.6 ,7 However, it is increasingly apparent that diverticulosis may be accompanied by inflammatory changes that mimic inflammatory bowel disease,8 ,9 and that caution should be exercised in making a diagnosis of Crohn’s disease in the presence of diverticulosis. We have reviewed all individuals coming to surgery in one hospital over a 20 year period, in whom there was a histopathological diagnosis of both Crohn’s disease and diverticulitis.
Study group
The files of the Department of Histopathology of the General Infirmary at Leeds were searched for specimens coded for both Crohn’s disease and diverticulosis or diverticulitis. Over a 20 year period (1968–1988), 11 cases were identified in which histological features of both Crohn’s disease and diverticulosis were confirmed. The case notes of these patients were reviewed, with further follow up obtained from general practitioners in some cases.
Table 1 summarises the clinical details. The age of patients ranged from 45 to 82 years. There was a preponderance of older individuals and of women, both characteristic of diverticular disease rather than Crohn’s disease. All presented with diarrhoea, most also complaining of pain and rectal bleeding. The time interval between presentation and surgery was variable, the longest being four years (median one year). Patient 1 had a 16 year history of ulcerative colitis, treated with steroids, but presented with new symptoms. Patient 2 had a three year history of large bowel problems. Radiologically, this was always thought to be diverticular disease, but a mucosal biopsy investigation at the time showed inflammation and crypt abscesses, leading to a diagnosis of ulcerative colitis. Steroid therapy was commenced, but symptoms persisted, and eventually a colonic resection was undertaken. Patient 5 had a previous history of peptic ulceration. Patient 6 had a previous limited resection for diverticular disease. The remainder had no previous history of bowel problems.
Clinical details
Pathological findings
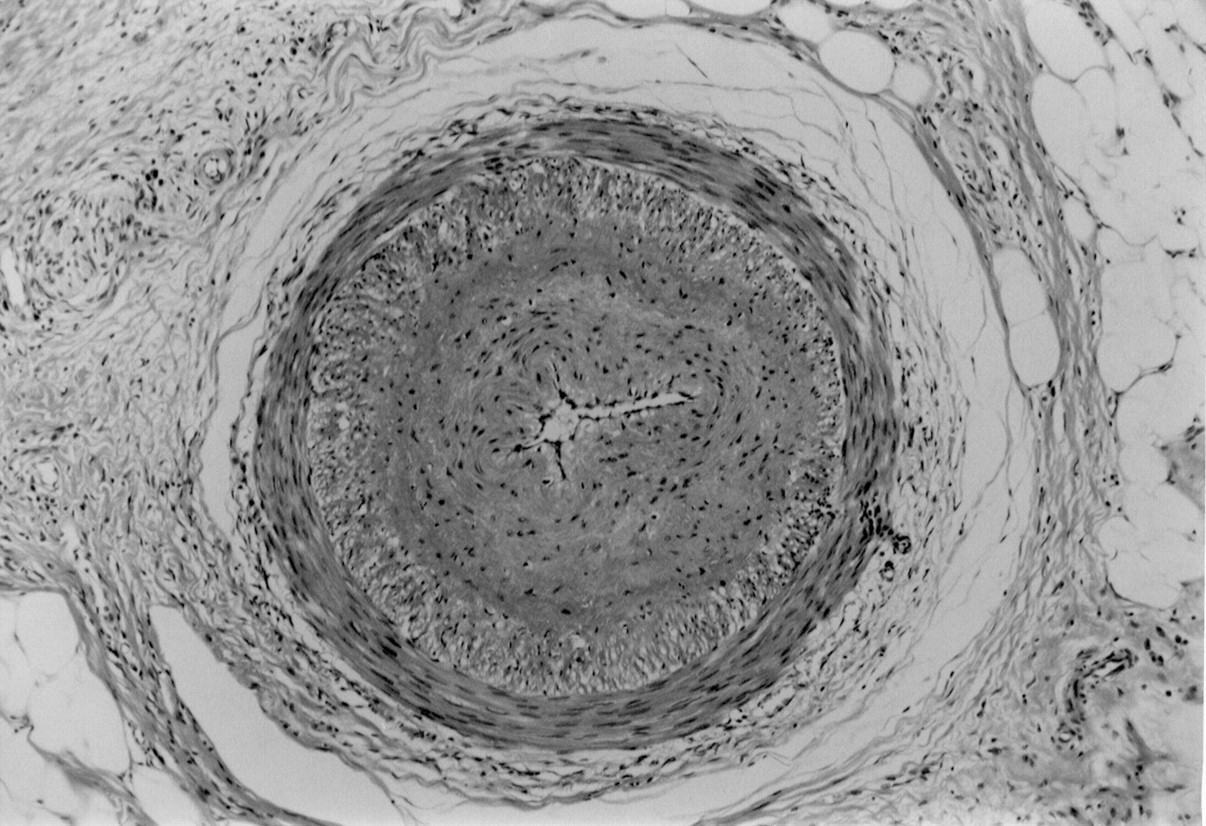
In all cases, the gross description included mural thickening; “creepage” of fat was mentioned in some, but not all. In all cases there was hypertrophy of the muscularis propria, with diverticula and peridiverticular abscesses typical of diverticular disease. Some had “under-running” abscesses, long thin tracts running between inflamed diverticula. The mucosa was frequently described as oedematous or cobblestone in appearance (fig 1). In all cases, microscopy revealed transmural granulomatous inflammation and ulceration typical of Crohn’s disease, with crypt abscess formation and fissuring ulceration in most cases (fig 2). The fissures tended to be within diverticula, but the inflammation also involved interdiverticular mucosa. The granulomas were present throughout the wall and in serosal fat. They appeared to be “true” granulomas, as opposed to foreign body reaction to faecal material (fig 3). Intimal hyperplasia in submucosal blood vessels was a striking feature in nearly all specimens, causing severe arterial narrowing (fig 4). The inflammatory changes were confined to the segment of bowel containing diverticula in all but two cases. In patient 1, inflammatory changes extended beyond the diverticula and were maximal at the hepatic flexure. In patient 2, features of Crohn’s disease were present in the terminal ileum.

Gross appearance, showing the “cobblestone” mucosa and hypertrophy of the muscularis propria.

Mucosal inflammation, with crypt abscesses and granuloma formation.

Higher power view of mucosal granuloma.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A frequent finding was marked narrowing of large extramural and submucosal vessels by intimal hyperplasia (original magnification ×100).
Clinical outcome
Table 2 summarises treatment and outcome in all patients. Three patients underwent proctocolectomy. The remainder were treated by sigmoid colectomy, with or without temporary colostomy. Follow up varied from one to 15 years. Two patients were lost to follow up after one year.
Treatment and outcome
In the study group, there were two perioperative deaths, patients 1 and 3. Patient 1 had a 16 year history of ulcerative colitis treated with steroids. Because of her history, she was treated by panproctocolectomy. The histological changes in the resection specimen were those of Crohn’s disease. The changes extended beyond the segment bearing diverticula, and were maximal at the hepatic flexure. Postoperatively, she developed peritonitis due to jejunal perforation, and died of a pulmonary embolus. Patient 3, who had also been on long term steroids, also underwent panproctocolectomy. Inflammatory changes were confined to the segment bearing diverticula. The postoperative course was complicated by sepsis and ultimately abdominal wound dehiscence, followed by death 60 days after surgery. It is probable that the long term steroid therapy was a factor in both these deaths.
The remaining nine individuals were discharged well. Only one patient (patient 2) has had recurrent problems. He had a long history of vague ill health prior to the acute episode. On presentation, he was thought clinically to have Crohn’s disease, but a barium enema suggested diverticular disease. At laparotomy he was found to have Crohn’s disease of the terminal ileum, adherent to the sigmoid colon. The terminal ileum and part of the sigmoid were removed. Since then he has had two further episodes of abdominal pain and rectal bleeding, ascribed to his Crohn’s disease, but has not required further surgery.
Discussion
A diagnosis of chronic idiopathic inflammatory bowel disease should be based on the combination of clinical, radiological, and histological findings. A diagnosis based purely on histological appearance is liable to error. In these 11 patients, Crohn’s disease was diagnosed on the basis of the “classic” histological features of transmural granulomatous inflammation and ulceration. In only two of these was the overall clinical picture suggestive of Crohn’s disease. In the remaining nine, the clinical presentation was diverticular disease. We suggest that the histological changes may represent a “Crohn’s type” response to diverticulosis, rather than Crohn’s disease per se.
In patients 1 and 2, histological features of Crohn’s disease extended beyond the area of diverticular disease. Both these individuals had clinical symptoms suggestive of inflammatory bowel disease prior to surgery. One died postoperatively. The other has had further symptoms consistent with inflammatory bowel disease. These two appear to be genuine instances of individuals with Crohn’s disease also developing diverticulitis.
Patient 3 had a three year history of large bowel problems originally thought to be ulcerative colitis. However, the resection specimen showed a Crohn’s type reaction limited to the segment of diverticular disease, with no evidence of inflammatory bowel disease elsewhere in the large bowel. The inflammatory changes seen in the initial mucosal biopsy specimen which led to an erroneous diagnosis of ulcerative colitis may well have been secondary to diverticular disease all along.
In the remaining patients, the histological features of Crohn’s disease were an incidental finding in a clinical setting otherwise typical of diverticular disease. Anatomically, the changes were confined to the segment affected by diverticular disease. Three individuals were noted to have perianal skin tags, but in an elderly, constipated population the significance of this is likely to be low. There was neither active perianal nor small bowel disease. While Crohn’s colitis is most likely to affect the sigmoid colon, the absence of any other disease sites would be unusual. The clinical course pursued in these cases is also more suggestive of diverticular disease than Crohn’s disease. In all nine, the illness leading to colonic resection was an isolated incident, albeit protracted in some cases. There had been no previous episodes of inflammatory bowel disease, and no recurrence. Diverticulosis is usually cured by surgery,10 but further episodes of disease might be anticipated if this were Crohn’s disease, recurrence rates for colonic disease treated by resection ranging from 31–75% over a 10 year period.11
It has been suggested that late onset Crohn’s colitis may precipitate diverticulitis in previously asymptomatic diverticular disease.12 Both the strict localisation of the inflammatory changes to the segment bearing diverticula, and the absence of recurrence in this study argue against this suggestion. There have been previous reports of non-specific segmental colitis in association with diverticulitis,13 ,14 with the suggestion that an underlying motor disorder might be responsible for both the diverticular disease and the inflammation. We believe that the granulomatous inflammatory response seen in these patients is a similar, diverticulosis associated phenomenon. Faecal stasis is postulated to be an aetiological factor in idiopathic inflammatory bowel disease, both due to changes in bacterial flora and to bacterial enzyme activity.15 Stasis within sigmoid diverticula may lead to similar changes. In addition, in the present study, a striking feature in many patients was the degree of arterial narrowing. This may well be secondary to inflammation, but whatever the cause of the intimal proliferation, the effect would be to impair blood flow. The mucosa would then receive a double insult of relative ischaemia and a change in bacterial flora due to diverticulosis, which may be responsible for the Crohn’s type inflammatory response. A localised “Crohn’s type” reaction is a rare but well recognised finding in the neighbourhood of carcinoma of the colon.16 It has also been suggested that granulomatous inflammation of the appendix may be seen as an isolated phenomenon, unrelated to Crohn’s disease.17 This may be yet another example.
In summary, an incidental finding of the histological features of a Crohn’s type reaction in a segment of bowel affected by diverticulitis should not automatically lead to a diagnosis of Crohn’s disease. Such a diagnosis must be based on a combination of clinical, radiological, and pathological findings, and in the context of diverticulitis, histological appearances suggestive of Crohn’s disease should not be given undue weight.