Article Text

Abstract
Background—Many patients with idiopathic constipation do not respond to conventional medical treatments. Recently biofeedback has been proposed as an alternative treatment but the long term results, and which patients benefit, are unknown. Treatment has usually been restricted to patients with normal colonic transit and impaired pelvic floor coordination on straining.
Aims—To determine the efficacy and long term outcome of biofeedback treatment in idiopathic constipation.
Methods—One hundred consecutive contactable patients who had completed a course of biofeedback more than 12 months previously were identified. Pretreatment details of bowel function and symptoms, whole gut transit time, and anorectal physiological testing, which had been previously prospectively collected, were collated. Follow up consisted of structured interview. Sixty five per cent had slow transit and 59% had paradoxical pelvic floor contraction on straining.
Results—Median follow up was 23 months (range 12–44). On long term follow up 55% felt that biofeedback had helped and 57% felt their constipation was improved. There was a significant reduction in need to strain, abdominal pain, bloating, and oral laxative use. Spontaneous bowel frequency was significantly improved by treatment. Patients with slow and normal transit, males and females, and those with and without paradoxical contraction of the anal sphincter on straining, benefited equally from treatment. Anorectal testing did not predict outcome.
Conclusion—This study suggests that biofeedback is an effective long term treatment for the majority of patients with idiopathic constipation unresponsive to traditional treatments. Pelvic floor abnormalities and transit time should not form selection criteria for treatment.
- constipation
- biofeedback
- follow up
- laxatives
- transit time
Statistics from Altmetric.com
Many patients with the subjective complaint of constipation are resistant to laxatives and experience major physical, social, and psychological impairment from their condition. Inappropriate pelvic floor contraction in many of these patients during attempted defaecation1 ,2 has formed the original focus for behavioural therapies and biofeedback has become a well established technique, especially when patients have failed to respond to simple measures such as dietary modification and laxatives.3-9However the long term results and predictors of outcome are unknown.
Although most groups have restricted the use of biofeedback to patients with normal transit and paradoxical pelvic floor contraction during straining, we have been impressed that the technique has a wider therapeutic benefit. The process of focusing on the gut and pelvic floor seems also to help patients who do not show this physical abnormality, including some with slow transit and some in whom defaecation straining is excessive. We have therefore also applied behavioural techniques to patients with slow colonic transit, and patients who complain of constipation but do not show these classic pelvic floor abnormalities. Many of these patients normalise their bowel frequency and transit time,10 or overcome the need to strain.11
More recently we have observed that many of these same patients have a more profound disturbance of their sense of abdominal and pelvic coordination10 and attention to these aspects now also forms part of biofeedback retraining. In most studies a simple visual or auditory electromyogram (EMG) or pressure signal of sphincter activity is fed back to the patient so that they can make appropriate alterations to their behaviour. Most techniques also use a method of simulated evacuation, such as the expulsion of a balloon, to demonstrate to the patient normal coordination for successful expulsion. In addition to coordination training, with or without the biofeedback component,12-14 biofeedback also involves patient advice and education. A rapport between the patient and the therapist is essential.15
Most series report a success rate of between 50 and 90% using these techniques, but we are unaware of any large series in adults reporting long term follow up. The aim of this study was to determine the long term efficacy of biofeedback in a large group of adult patients with the subjective complaint of constipation, reflecting decreased bowel frequency or the excessive need to strain at stool. We also wished to determine which physiological or psychological factors might predict the outcome of this therapy.
Methods
Nearly all patients referred to our hospital with idiopathic constipation have long standing symptoms unresponsive to laxatives and dietary changes. About half are derived from primary care physicians and half come from other specialist gastroenterologists and colorectal surgeons. Our hospital is a specialist institution for the treatment of intestinal disorders. Patients can enter the biofeedback programme either by direct referral from the doctor outside the hospital, or by referral from one of the hospital consultant physicians or surgeons. The therapy is regarded as a first line treatment. Patients are unselected; the only criterion for treatment is the subjective complaint of constipation which is unresponsive to dietary or drug treatment. This is always associated with either an excessive need to strain or an abnormally decreased bowel frequency.
Patients are only given biofeedback treatment for idiopathic constipation. All have had a rectal examination to exclude megarectum, and radiological or endoscopic examination of the large bowel as appropriate. Patients with a dilated bowel or endocrine or other recognised causes of secondary constipation are not treated with biofeedback.
BIOFEEDBACK THERAPY
Each patient sees a biofeedback therapist as an outpatient every one to two weeks, usually for four or five sessions. They lie on a couch on their right side facing the therapist and the EMG display unit. A balloon is inserted into the rectum and inflated with 50 ml of air so that the patient has the sensation of a full rectum and thus the need to defaecate. Two adherent surface electrodes are placed adjacent to the anal opening to assess external anal sphincter function. The patient watches the trace of muscle activity and can see the pattern of electrical activity at rest and during voluntary contraction. The patient is then asked to observe the trace while attempting to expel the balloon. If there is an obvious increase, rather than the normal decrease in activity, the patient is encouraged to strain without increasing sphincter activity so that its appearance continues to resemble the resting trace.
Patients are also taught how to strain effectively by using a propulsive force through bracing with their abdominal muscles. They are advised on normal defaecatory behaviour and bowel habits. This includes restricting the number of visits to the toilet for patients who make frequent defaecatory attempts during the day, or increasing the number of visits to the toilet for those patients with infrequent defaecation. The amount of time spent, and posture, in the toilet are also specified.
At each biofeedback session the therapist tries to achieve a good rapport with the patient to facilitate good understanding and collaboration. This includes gaining an appreciation about the patient’s personal life and psychological factors which may be relevant.
An attempt is made to get patients off laxatives, enemas, and suppositories. Sometimes this is achieved early in the course of therapy, and sometimes progressively over a longer period. When the course of biofeedback is complete patients are encouraged to continue practising the techniques they have learnt.
REVIEW OF MEDICAL NOTES
We aimed to study 100 consecutive patients who had completed a course of biofeedback more than 12 months previously. This entailed attempting to contact approximately 110 consecutive patients. Ten were not contactable due to having moved house, leaving 100 contactable patients who form the basis of the results presented. When examining pretreatment details, the clinical details of the 10 patients who were not contactable were similar to those 100 who formed the definitive study.
Data which had been previously prospectively collected, prior to treatment, according to a standard proforma, were collated for details about bowel function and symptoms and non-gastrointestinal conditions. Psychological factors which are routinely enquired about during biofeedback treatment were also recorded. These were defined as previous sexual or physical abuse, previous contact with a psychiatrist, psychologist, or counsellor, and previous treatment for depression.
The results of physiological assessments prior to biofeedback were also noted. We wished to determine whether patients with slow or normal transit were more likely to be helped by this technique. We also wished to determine whether patients without paradoxical contraction, but with the same symptomatic complaints, might be helped to the same degree as those with abnormal contraction. Finally we wished to know whether rectal sensitivity might serve as a prognostic marker, because sensory function may serve as a marker of denervation.
Whole gut transit study
Patients ingested three sets of radiologically distinguishable radio-opaque markers over three days and then had a plain abdominal radiograph 120 hours after ingesting the first set. Patients who retained a number of markers beyond the previously established normal range for any of the three sets were regarded as having slow colonic transit.16 This test was not done routinely on every patient, but became a routine test prior to biofeedback during the period being studied and was performed on most subjects.
Anorectal physiological studies
Rectal sensory function to distension was assessed using an intrarectal balloon, according to previously published techniques.17 The volumes at which there was an initial sensation, a sensation of urgency, and the maximum tolerated volume were recorded. Rectal sensation to an electrical stimulus was also assessed, using a bipolar electrode placed in the rectum 6 cm above the upper limit of the anal canal. This technique has been previously validated.18
Pelvic floor coordination was also assessed using surface electrode EMG during simulated defaecation straining. Paradoxical contraction of the external anal sphincter during straining was noted. This test was also not done routinely on every patient, but became a routine test prior to biofeedback during the period being studied and was studied in most patients.
TELEPHONE INTERVIEW
Each patient was interviewed over the telephone by an investigator who had not been the patient’s biofeedback therapist. Data were obtained using a questionnaire containing the same questions as those recorded before treatment.
Using these pretreatment and post-treatment data, an assessment was made regarding the age of onset of the patient’s constipation, and whether there were any precipitating factors, including vaginal delivery, hysterectomy, or other surgery. Bowel function before biofeedback, immediately after biofeedback, and at the time of interview was assessed, including the use of bowel evacuants (oral laxatives, enemas, and suppositories), bowel frequency without laxatives, need to strain, need to digitate, and a sense of incomplete evacuation. Enquiries were also made about the presence and subjective severity of abdominal pain or bloating.
To establish the possible subjective benefits of the treatment as a whole, in addition to the effect on constipation, patients were asked whether they felt that biofeedback had helped them and whether or not their constipation had improved. They were also asked whether they routinely practise the biofeedback techniques they had learnt.
PROGNOSTIC FACTORS
To determine whether certain patient characteristics may predict a response to biofeedback treatment, patients who felt subjectively that biofeedback had helped them were compared with those who felt they had not been helped. Parameters used for comparison were the objective findings of slow or normal transit, the presence or absence of pelvic floor paradoxical contraction on straining, and the rectal sensory response to distension (threshold, urge, and maximum tolerated volume) and an electrical stimulus (threshold). A comparison was also made for gender, whether women had had a hysterectomy (regardless of whether it was thought to be the cause of the constipation), the presence of previous psychological factors, and whether the patient practised the biofeedback techniques at home after the treatment had finished.
Results
All 100 patients who were contactable agreed to participate in the study. Table 1 shows the patient characteristics. The vast majority of patients were female. Each patient had only one course of biofeedback. One third of the patients had experienced constipation since childhood. Half the patients believed they could identify a factor which precipitated their constipation. One fifth of patients were recorded as having psychological factors of possible relevance. Sixty eight patients reported constipation as their only health problem. The median length of follow up from completing the course of biofeedback to the time of interview was 23.4 months (range 12–44 months).
Patient characteristics and factors precipitating constipation
INVESTIGATIONS
Among the 81 patients who underwent a colonic transit study, 53 had slow colonic transit. Physiological studies were performed on 88 patients and 52 of these showed paradoxical external anal sphincter contraction. Of the 71 patients who had both a transit study and physiological studies, 18 had slow transit constipation but no paradoxical contraction, 29 had both slow transit and paradoxical contraction, 15 had normal transit with paradoxical contraction, and 11 had neither slow transit nor paradoxical contraction (see table 2). Not every patient underwent full investigations so that in 19 patients no transit results were available, with 12 patients having no physiological testing.
Results of the whole gut transit and anorectal physiological testing
BOWEL SYMPTOMS
The need to strain, rectal digitation, and a sense of incomplete evacuation were all significantly improved both immediately after biofeedback and after long term follow up. The proportion of patients who needed to vaginally digitate was also reduced, but this did not reach statistical significance, probably due to the small number of patients with this symptom. The proportion of patients with pain or bloating, and those with more severe pain or bloating, were all significantly reduced by the treatment (table 3). Comparisons between the “before biofeedback”, “after biofeedback”, and follow up” groups were made using the χ2 test. Comparing pain before and immediately after biofeedback showed a significant reduction (p=0.003) which was maintained at follow up (p=0.0004). The amount of abdominal bloating was also reduced after biofeedback (p<0.0001) and at follow up (p<0.0001).
Presence of the functional symptoms straining and digitation before and after biofeedback
The proportion of patients with a normal bowel frequency significantly increased after biofeedback and this was maintained on follow up (table4). All frequencies indicated in the table were for patients when not taking laxatives. Some patients were laxative dependent and were not included in the table. Using the 3 × χ2 test to compare groups there was a significant improvement in bowel frequency immediately after biofeedback (p=0.001) and at follow up (p<0.001).
Number of patients with low, normal and high bowel frequencies before and immediately after biofeedback and at follow up
USE OF ORAL LAXATIVES, ENEMAS, AND SUPPOSITORIES
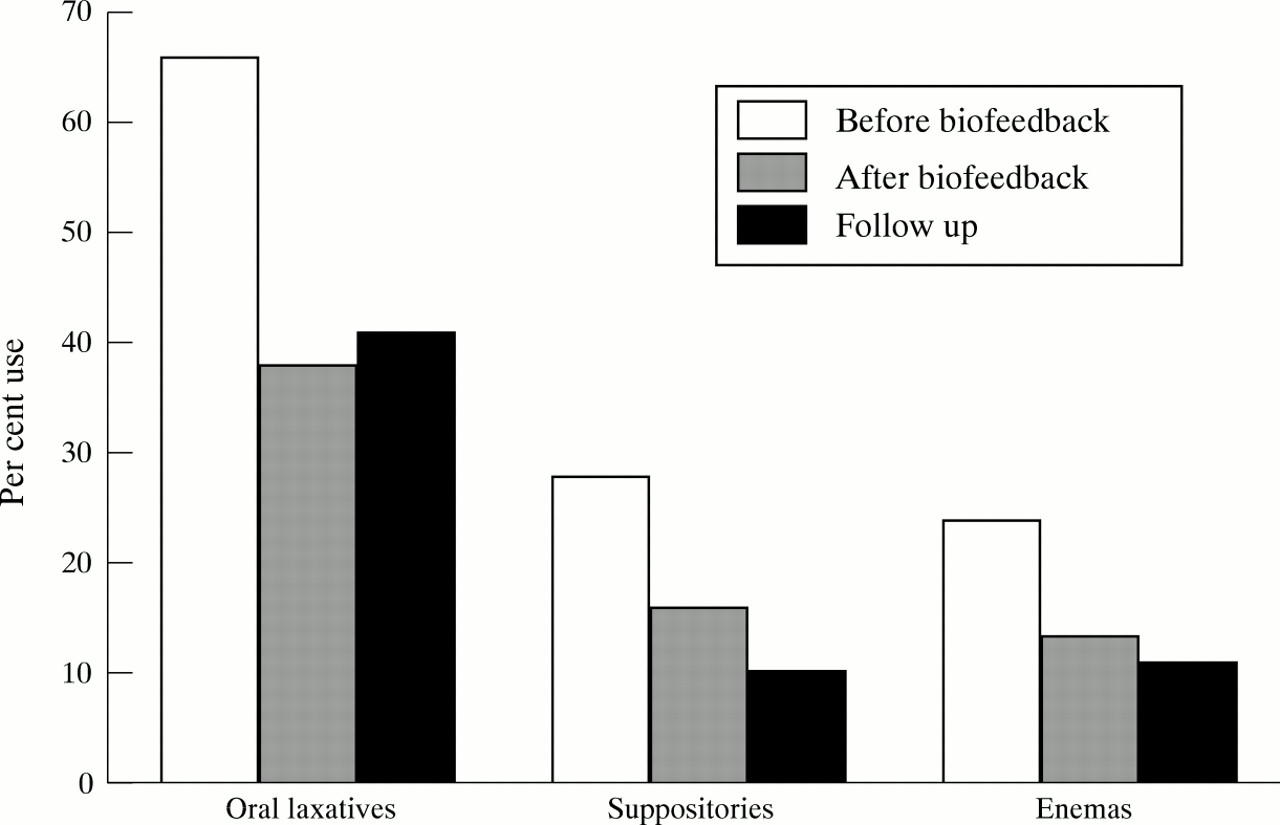
The use of all types of bowel evacuant was reduced immediately after biofeedback: oral laxatives 66% versus 38% (p<0.01), enemas 24% versus 13% (p<0.07), and suppositories 28% versus 16% (p=0.06) (fig 1). This reduction was maintained at follow up, with no significant differences for any of the three types of medication when comparing their use immediately after biofeedback and at long term follow up.
{kind=link}
Use of oral laxatives, enemas, and suppositories.
SUBJECTIVE IMPROVEMENT
Two thirds of patients felt that the biofeedback had helped them immediately after treatment, and on long term follow up this was maintained in more than half of all the patients (table 5). Half or more of all the patients felt that their constipation had improved both immediately after biofeedback and after long term follow up. There were no significant differences between immediate and long term improvement.
Subjective improvement in bowel symptoms for the patients immediately after biofeedback and at long term follow up
PROGNOSTIC FACTORS
The failure to practise the biofeedback techniques after the completion of the treatment course was significantly associated with a failed outcome immediately after biofeedback treatment (practised: 88% in the success group versus 67% in the failure group, p<0.01, χ2 test). This significant difference did not persist on long term follow up. The presence of previous psychological factors suggested that failure was more likely, although this did not reach statistical significance: psychological factors were present in 14% of the success group and 24% of the failure group (p=0.07; table 6). Men and women were equally likely to have been helped, as were patients who had or had not had a previous hysterectomy. Patients with slow transit were as likely to be helped as those with normal transit, and patients with abnormal pelvic floor contraction were as likely to be helped as those without this finding. Rectal sensory testing did not predict outcome.
Prognostic factors for biofeedback success after long term follow up
Discussion
This study has shown that biofeedback is a successful treatment for constipation which patients and their doctor judge to have been unresponsive to other treatments. More than half of these patients considered themselves to have benefited in the long term, and this was objectively supported by their decreased use of laxatives. Symptom improvement related not only to bowel frequency, but also to associated symptoms such as bloating, which patients often consider to be the most troublesome and which often are the least responsive to other treatments. Recent evidence from our group suggests that a successful response to biofeedback may be associated with an altered level of activity of the extrinsic nerves supplying the intestine19; a diminution in bloating may therefore relate to altered viscerosomatic reflexes or may merely be secondary to the improved bowel function.
For many patients who responded, symptoms were long standing; the median age of onset of constipation was 21 years, while the median age at biofeedback therapy was 40 years. In this study, as in the general population, constipation was a predominantly female problem.
To our knowledge only one other series has reported long term follow up. Five patients who completed a protocol of treatment improved their bowel frequency from a mean of 1.89 to 4.4 per week, and decreased their abdominal pain and bloating, after a follow up of 2–4.5 years.20
For such a labour intensive treatment it is important to try to determine which patients are likely to respond to treatment. Psychological factors were more common in those who failed treatment, although this did not reach statistical significance. This was a retrospective study in which psychological factors are likely to have been underestimated. Some details of a patient’s history, such as sexual abuse, are often not volunteered. Future use of prospective structured questionnaires relating to such psychological issues may be more helpful in selecting patients for this type of treatment, or focusing the treatment in a particular direction.
Physiological factors did not predict a response to treatment. Patients with slow transit subjectively improved and increased their bowel frequency. In a previous study we have shown that these patients can also normalise their measured transit time.10 The absence of paradoxical pelvic floor contraction during straining also did not preclude benefit. Therefore, contrary to the literature,4 ,5 ,11 ,21 ,22 neither of these factors should preclude patients from selection for this treatment.
Practising the techniques learnt during biofeedback therapy was a significant predictor of benefit immediately after treatment, but not on long term follow up. In the early phase of treatment this may reflect patient motivation as a prognostic factor, or alternatively a reinforcement to a patient who has already had benefit. Compliance with the technique is emphasised during treatment and patients are asked whether they have practised these techniques each day. Patients who have benefited, in addition to those who have failed, are unlikely to practice these techniques long term.
A small group of patients experienced initial benefit which was not sustained. We now offer patients the opportunity of a “refresher” session at a later date. Only a minority of patients require this and it seems to restore benefit.
In conclusion, this study has shown long term benefit from a behavioural treatment of resistant idiopathic constipation in a majority of patients. Further studies are required to determine whether this is reflected in improved quality of life and consulting behaviour.