Article Text

Abstract
Background—The efficacy of endoscopic biopsy surveillance of Barrett’s oesophagus in reducing mortality from oesophageal cancer has not been confirmed.
Aims—To investigate the impact of endoscopic biopsy surveillance on pathological stage and clinical outcome of Barrett’s carcinoma.
Methods—A clinicopathological comparison was made between patients who initially presented with oesophageal adenocarcinoma (n=54), and those in whom the cancer had been detected during surveillance of Barrett’s oesophagus (n=16).
Results—The surveyed patients were known to have Barrett’s oesophagus for a median period of 42 months (range 6–144 months). Prior to the detection of adenocarcinoma or high grade dysplasia, 13 of 16 patients (81%) were previously found to have low grade dysplasia. Surgical pathology showed that surveyed patients had significantly earlier stages than non-surveyed patients (p=0.0001). Only one surveyed patient (6%) versus 34 non-surveyed patients (63%) had nodal involvement (p=0.0001). Two year survival was 85.9% for surveyed patients and 43.3% for non-surveyed patients (p=0.0029).
Conclusions—The temporal course of histological progression in our surveyed patients supports the theory that adenocarcinoma in Barrett’s oesophagus develops through stages of increasing severity of dysplasia. Endoscopic biopsy surveillance of Barrett’s oesophagus permits detection of malignancy at an early and curable stage, thereby potentially reducing mortality from oesophageal adenocarcinoma.
- Barrett’s oesophagus
- endoscopic surveillance
- oesophageal adenocarcinoma
Statistics from Altmetric.com
In Barrett’s oesophagus the normal squamous mucosa has been replaced by metaplastic columnar epithelium. Barrett’s oesophagus is a well known premalignant condition and is found in 10–15% of patients who undergo endoscopy for symptoms of gastro-oesophageal reflux.1 ,2 The prevalence of Barrett’s oesophagus in the general population is not precisely known. From an autopsy study, it has been concluded that in most individuals with Barrett’s oesophagus this condition remains unrecognised.3 Consequently, the risk of developing adenocarcinoma in Barrett’s oesophagus may well be overestimated.4 Adenocarcinomas of the distal oesophagus and oesophagogastric junction have nevertheless shown a greater increase in incidence than any other cancer during the past two decades.5 ,6 Given the low five year survival rate of advanced oesophageal cancer, strategies for early detection have been explored. Implementation of an endoscopic surveillance programme for patients in whom Barrett’s oesophagus has been detected seems a reasonable option. However, since its efficacy in reducing mortality from oesophageal cancer has never been evaluated in a randomised study, surveillance of Barrett’s oesophagus is still a matter of debate.
To contribute to this ongoing discussion, we investigated the impact of endoscopic biopsy surveillance on pathological stage and clinical outcome of adenocarcinoma arising in Barrett’s oesophagus. The study population consisted of patients who underwent oesophageal resection for Barrett’s carcinoma. For the purpose of the study, a clinicopathological comparison was made between patients with carcinoma at initial presentation and patients in whom the cancer had been detected during surveillance. In addition, a careful documentation was made of all biopsy results in the surveillance period.
Methods
STUDY POPULATION
Between January 1993 and July 1996, 198 patients with cancer of the oesophagus or oesophagogastric junction underwent oesophageal resection with curative intent (locally resectable disease without distant metastases) at the surgical department of the Academic Medical Centre in Amsterdam, The Netherlands. The pathology reports of all 198 surgical resection specimens were reviewed in order to identify those patients who had been operated on for adenocarcinoma or high grade dysplasia arising in Barrett’s mucosa. In this study, Barrett’s carcinoma was defined as an adenocarcinoma arising in the oesophagus in the presence of adjacent Barrett’s mucosa. The diagnosis of Barrett’s mucosa required the pathological finding of a segment of intestinal metaplasia within the tubular oesophagus.7 ,8 Neoplastic lesions with infiltration through the epithelial basement membrane were identified as “invasive adenocarcinoma”. The term “carcinoma in situ” was avoided. A diagnosis of “high grade dysplasia” was restricted to lesions in which no infiltration through the basement membrane into the lamina propria was shown.9 ,10 In our hospital, unequivocal high grade dysplasia is regarded as an indication for oesophagectomy for patients in whom a major operation is feasible.11-13
Review of the surgical pathology records identified 70 consecutive patients with either adenocarcinoma or high grade dysplasia arising in a histologically proven Barrett’s oesophagus. This population of 70 patients was divided into two groups: the first group consisted of those patients who had Barrett’s carcinoma at initial presentation; the second group included those patients who had undergone endoscopic surveillance of Barrett’s oesophagus. As “endoscopic surveillance” is a widely used term, being applied to various follow up programmes for patients with Barrett’s oesophagus, criteria for inclusion in the surveillance group were defined. These included: (1) a histologically proven Barrett’s oesophagus diagnosed at least six months prior to surgery; and (2) subsequent endoscopic examination performed for the diagnosis of Barrett’s oesophagus.
Clinical and histopathological data were obtained from patient records and pathology reports. In our hospital, a surveillance endoscopy includes obtaining four biopsy specimens, one from each quadrant of the oesophagus, every 2 cm along the visible length of Barrett’s mucosa, with additional specimens from any abnormal appearing area.14 Each biopsy specimen is separately assessed, sectioned at three different levels, and routinely stained with haematoxylin and eosin (H&E). If endoscopic surveillance had taken place outside our hospital, the original reports on previous endoscopic and biopsy examinations were collected from the referring centres. All H&E stained sections of the biopsy specimens that had been obtained at other institutions and had resulted in referral for surgical intervention, were reviewed in our hospital. Post-surgical staging of tumours was done according to the pTNM (pathological tumour, node, metastases) classification of oesophageal carcinoma.15Tissue samples were routinely obtained from the primary tumour, the adjacent mucosa, and from all lymph nodes that were recognised as such. If no macroscopic tumour was visible in the resection specimen, the Barrett’s segment was processed in its entirety.
SURGICAL PROCEDURE
All patients in the study population underwent oesophageal resection for locally resectable disease without distant metastases. The resection was performed either by a transhiatal approach without thoracotomy or by a transthoracic approach combined with a two fields lymphadenectomy. The two operative techniques were equally distributed among patients in the non-surveillance group and patients in the surveillance group (p=0.45; χ2 test). If possible, gastrointestinal continuity was reestablished by constructing a gastric tube; only two patients had a colonic interposition.
FOLLOW UP
Patients were followed until death or December 1997. No patients were lost to follow up. The mean follow up period was 24 months in the non-surveillance group (range 1.5–44.6 months) and 48 months in the surveillance group (range 10.2–55.6 months).
STATISTICAL METHODS
Comparisons between groups were made using the Mann-Whitney U test, χ2 test, or Fisher’s exact test when appropriate. Survival was estimated according to the method of Kaplan and Meier, including all causes of death. The log rank test was used for comparison of survival curves. Probabilities are two tailed with statistical significance determined at a 95% confidence interval.
Results
CLINICAL FEATURES
Fifty four patients initially presented with Barrett’s carcinoma, and 16 met the criteria for inclusion in the surveillance group. The groups were similar with respect to age and sex (table 1). In the non-surveillance group, all patients were symptomatic at the time of presentation. In contrast, 10 of the 16 surveillance patients (63%) had no symptoms at the time adenocarcinoma or high grade dysplasia was diagnosed on routine endoscopy for surveillance of Barrett’s oesophagus. In four patients the development of symptoms resulted in earlier evaluation than would have occurred with their planned regular endoscopy; two other symptomatic patients had awaited their routine surveillance interval for endoscopic examination. A history of gastro-oesophageal reflux symptoms was reported more frequently in the surveillance group than in the non-surveillance group (table 1). Antireflux surgery had been performed in one non-surveillance patient; one surveillance patient had previously undergone a partial gastrectomy for peptic ulcer disease.
Patient characteristics, presenting symptoms and history of reflux symptoms
SURVEILLANCE
Ten patients had been surveyed at other institutions and were referred when adenocarcinoma or high grade dysplasia in Barrett’s oesophagus was diagnosed; six patients had been under surveillance for Barrett’s oesophagus at our own institution. Figure 1 shows the duration and frequency of endoscopic surveillance with the accompanying histological findings. The patients were known to have a histologically proven Barrett’s oesophagus for a median period of 42 months, ranging from six months to 12 years. During this period they had been endoscopically surveyed at intervals ranging from two months to 2.5 years (median 10 months). In this study population of 16 patients, three patients (19%) were found to have invasive carcinoma without ever having been diagnosed with low grade or high grade dysplasia (patients 3, 6, and 11). In the other 13 patients (81%), low grade dysplasia had been identified on at least one occasion prior to the detection of adenocarcinoma or high grade dysplasia. In eight of 11 patients (73%) who were diagnosed with adenocarcinoma, dysplastic epithelium had been detected on previous endoscopic biopsy specimens. In addition, all five patients who underwent surgery for high grade dysplasia were previously found to have low grade dysplasia.

Duration and frequency of endoscopic surveillance with the accompanying histological findings in 16 patients undergoing surveillance of Barrett’s oesophagus. Black dots represent endoscopic examinations at which no biopsy specimens were obtained.
PREOPERATIVE DIAGNOSIS
In the non-surveillance group, 53 of the 54 patients (98%) had a preoperative diagnosis of adenocarcinoma (table 2). The one non-surveillance patient (2%) in whom high grade dysplasia was diagnosed underwent endoscopic examination because of dyspeptic symptoms. Of the 16 patients who underwent surveillance, there were 11 patients (69%) with a preoperative diagnosis of adenocarcinoma and five patients (31%) with high grade dysplasia. Table 3 shows the macroscopic features at preoperative endoscopic examination, the length of the Barrett’s segment, and the accompanying diagnosis at biopsy. Interestingly, in three of these 16 patients (19%; patients 9, 10, and 11), there were no endoscopic findings suggestive of malignancy. However, the presence of invasive adenocarcinoma was identified by routine biopsy.
Preoperative diagnosis at endoscopic biopsy
Preoperative endoscopic examination in 16 patients who underwent surveillance of Barrett’s oesophagus
SURGICAL PATHOLOGY
All oesophagectomy specimens in the non-surveillance group revealed invasive adenocarinoma arising in Barrett’s mucosa. In contrast, 25% of the surveillance group (four of 16 patients) had a final diagnosis of high grade dysplasia (table 4). Remarkably, two of these patients (patients 14 and 15) had been diagnosed with adenocarcinoma preoperatively. Even though the entire Barrett’s segment had been blocked, no evidence of invasion was found in the resection specimen. With regard to this pathological inconsistency, it is important to recognise that special staining of biopsy specimens to clarify invasion through the basement membrane is not routinely applied in our hospital. Whatever the outcome of such staining, it would not alter subsequent management. The remaining 12 surveillance patients (75%) had invasive adenocarcinoma in the resected oesophagus. Three of them had been referred for surgery because of high grade dysplasia at biopsy. Six patients in the total study population (one non-surveillance and five surveillance) had a preoperative diagnosis of high grade dysplasia. In each patient, multiple biopsy specimens were obtained, with a median number of nine specimens (range 6–17) per patient, and a median number of 4.5 specimens (range 3.0–6.7) at 2 cm intervals of Barrett’s mucosa. However, in four of these six patients (67%) invasive adenocarcinoma was detected in the surgical specimen. Systematic endoscopic biopsy examination had failed to identify the presence of cancer.
Postoperative diagnosis and follow up in 16 patients who underwent surveillance of Barrett’s oesophagus
The surgical pathological stages differed significantly between the two groups (fig 2): 18% of the non-surveillance patients and 75% of the surveillance patients had stages 0 or I; 26% and 25%, respectively, had stage II; and 56% and 0% had stages III or IV (p=0.0001; Mann-Whitney U test). Thirty four patients in the non-surveillance-group (63%) had pathological lymph nodes, whereas only one patient in the surveillance group (6%) had lymph node involvement (p=0.0001). The groups were comparable with regard to the morphology of the tumours—that is, the various grades of differentiation were equally distributed among both groups (p=0.81; Mann-Whitney U test).

Distribution of pathological stage.
FOLLOW UP
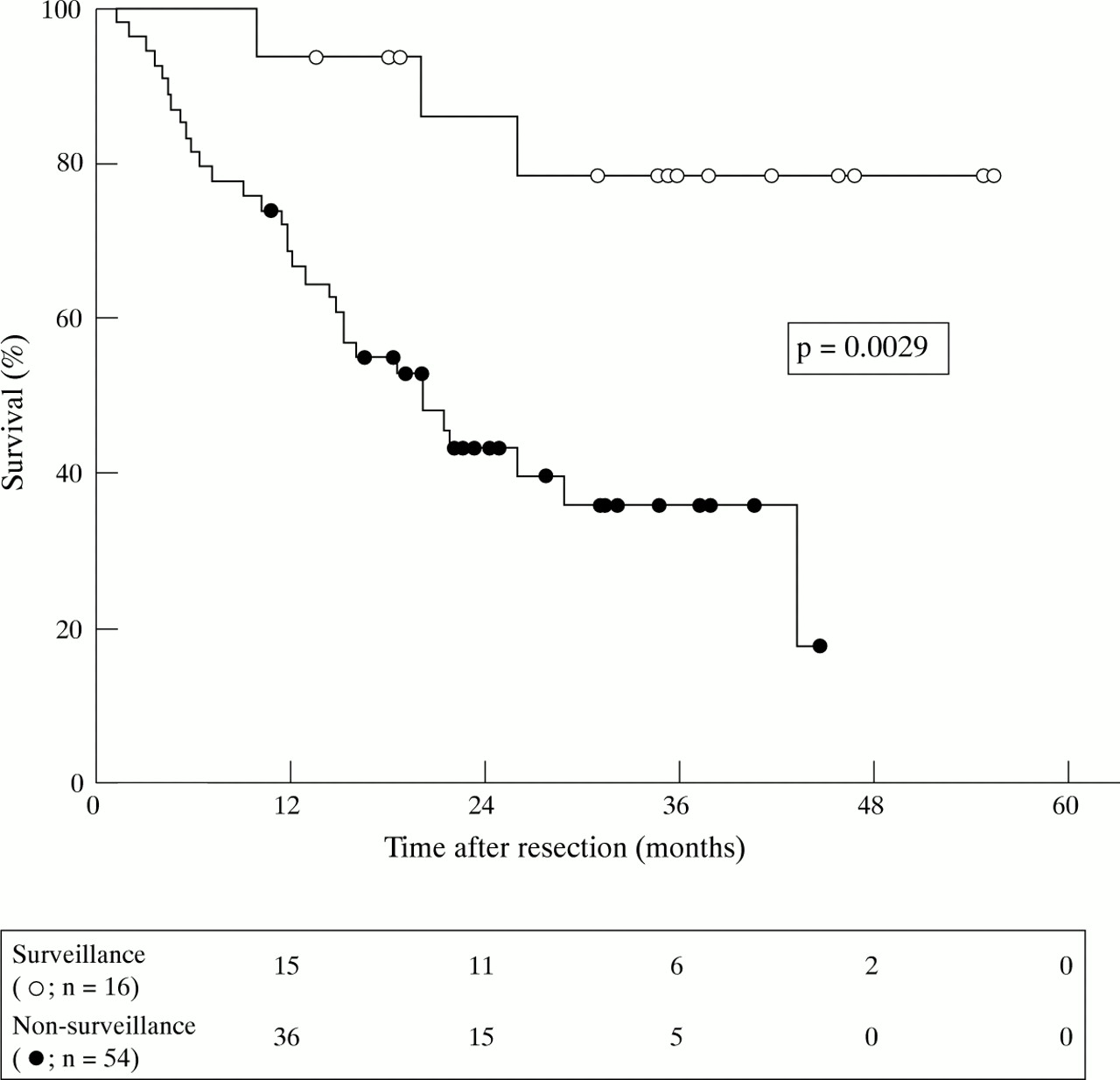
Figure 3 shows survival curves of both groups of patients after oesophageal resection. Survival of patients in the surveillance group was significantly better than that of patients in the non-surveillance group, with a two year survival of 85.9% and 43.3%, respectively (p=0.0029; log rank test). Three patients died in the surveillance group (table 4): two had radiologically verified distant metastases (patients 3 and 13); in one, who died cachectic, no diagnostic examinations had been undertaken to assess the tumour status (patient 8). In the non-surveillance group, 28 patients died from distant metastases and/or locoregional tumour recurrence. Four other deaths occurred in the non-surveillance group: two in the early postoperative course, one from lung cancer, and one from an unknown cause (19 months after operation, with no evidence of tumour recurrence). Excluding these four patients, survival in the non-surveillance group amounted to 47.1% at two years; the difference from survival in the surveillance group was still significant (p=0.0055). As high grade dysplasia is not universally regarded as an indication for oesophagectomy, survival was also analysed specifically within the group of patients who were shown to have invasive adenocarcinoma at biopsy (n=64; table 2), thereby excluding the patients with a preoperative diagnosis of high grade dysplasia alone (n=6). In this selective analysis also, postoperative survival in the surveillance group was significantly better than that in the non-surveillance group (80.0% versus 42.1% at two years; p=0.013).

{kind=link}
{kind=link}
{kind=link}
Postoperative survival. The numbers in the box refer to the number of patients at risk at 12 month intervals.
Discussion
Since the early 1970s adenocarcinomas of the distal oesophagus and oesophagogastric junction have shown a continuing increase in incidence, which surpasses that of any other type of cancer in the United States and in Europe.5 ,6 Although this may be partly due to changes in diagnostic methods or to an increased awareness, it probably also reflects a true increase. The single most important predisposing factor for development of adenocarcinoma in the oesophagus is the presence of a columnar lined oesophagus (Barrett’s oesophagus). The risk of cancer in patients with a Barrett’s oesophagus is increased 30 to 125-fold compared with the general population.4 ,16-19 Symptoms of oesophageal cancer generally correspond with the stage of the disease. Patients who initially present with dysphagia often have a dismal prognosis after surgery, as obstructive symptoms usually indicate the presence of advanced disease.20 On the other hand, patients who undergo surgery for Barrett’s carcinoma that is limited to the mucosa or submucosa (T1 tumour) have a favourable prognosis, with a 60–100% five year survival.21-23 Since early adenocarcinomas in Barrett’s oesophagus only rarely cause symptoms, detection of cancer at an early, curable stage can only be achieved by surveillance. The relatively high risk of carcinoma together with the poor prognosis of a symptomatic cancer seems sufficient to warrant a surveillance programme for patients with a Barrett’s oesophagus. Although its cost effectiveness has been questioned by some authors,24 ,25recent reports indicate that the cost of endoscopic surveillance in Barrett’s oesophagus compares favourably with the cost of endoscopic surveillance in other premalignant conditions of the gastrointestinal tract and with that of screening mammography to detect early breast cancer.26-28 The major concern is a lack of evidence that surveillance of Barrett’s oesophagus reduces mortality from oesophageal cancer. The ideal methodology for the evaluation of the efficacy of surveillance programmes is the randomised trial. Such a trial not only seems impractical in terms of the number of patients needed and the many years of follow up,8 but may also pose an ethical dilemma for the physician who is to withhold a potentially life saving procedure from the individual patient with a premalignant condition. Therefore, it is unlikely that a randomised study will ever be performed for cancer surveillance in Barrett’s oesophagus. The ongoing discussion will have to rely on more or less indirect evaluation of its effect on cancer mortality rate.
The present study suggests that endoscopic biopsy surveillance provides a beneficial effect on resectability and mortality from cancer in Barrett’s oesophagus. We found, in parallel with the findings of other authors,26 ,29 ,30 that patients who had undergone some form of endoscopic surveillance were operated on at significantly earlier stages of their disease, with a subsequent survival advantage over patients who had not been part of a surveillance programme. The method of evaluating cancer surveillance that we applied—comparing the outcome of surveillance detected cases with that of symptom diagnosed cases—is probably the most commonly used method. We acknowledge the fact that non-randomised types of evaluation harbour a number of pitfalls.31 ,32 Firstly, one must be aware of selection bias. Patients undergoing regular surveillance tend to be health conscious and may be the ones who would have presented with early stage cancer even if their disease were diagnosed because of symptoms. Secondly, lead time bias operates in all screening and surveillance programmes.33 An observed survival benefit may be due only to the advancement of the diagnosis of cancer in time, and not to the postponement of death. Finally, the evaluation of cancer screening is subject to length bias.34 This occurs because screening programmes are more likely to detect slow growing lesions with a good prognosis than lesions with a more aggressive nature and relatively unfavourable prognosis. Importantly, comparison of the histological type of tumours found in the two groups of our study population gave no support to different biology, as tumour differentiation was similar in both groups. Nevertheless, in ours and similar series, the stage distribution and duration of survival in the surveillance group may partly reflect the lead time and length bias for cancer in Barrett’s oesophagus. To acknowledge these factors, results should be analysed on an “intention to surveillance” basis,32 as was performed in our study.
Despite these problems of evaluating cancer surveillance in Barrett’s oesophagus, efforts to do so should be continued in order to clarify factors that affect its outcome and to assess current inconsistencies in clinical practice. During a consensus conference held in August 1995, guidelines for surveillance of Barrett’s oesophagus were established by the International Society for Diseases of the Esophagus.14 In search for dysplastic foci, the entire length of the Barrett’s mucosa should be sampled, with four quadrant biopsy specimens obtained at 2 cm intervals.35 It can be expected that in clinical practice surveillance programmes will be less than perfect. Most patients in our surveillance group had been followed up by regular endoscopy with multiple biopsies at intervals determined by the diagnosis at biopsy. In two patients (patients 3 and 6), repeated endoscopies were performed, but concurrent biopsy specimens were taken only when a suspicious lesion was recognised. In general, no specific endoscopic features permit a distinction between dysplastic and non-dysplastic mucosa.36 Even invasive cancer may not be visible at endoscopic examination, as is illustrated by our data (table 3). Three of the 16 patients (19%) who underwent surveillance had no suspicion of a malignant lesion at endoscopic examination. Invasive adenocarcinoma was however found at biopsy. If endoscopic evaluation alone had been performed, the opportunity of detecting cancer at an early stage would have been missed in these patients. Obviously, these observations are limited to a small number of patients; they nevertheless emphasise the importance of a systematic biopsy approach in Barrett’s oesophagus. We applied a relatively broad definition of surveillance, thereby including a variety of surveillance strategies performed at various institutions, albeit by well defined criteria. The study reflects endoscopic reality in general practice and, even though not resulting from a uniform surveillance protocol, its outcome provides arguments in favour of endoscopic surveillance for patients with Barrett’s oesophagus. These arguments need to be evaluated in a prospective study of a well defined surveillance programme.
In our study, the temporal course of histological progression in Barrett’s oesophagus was analysed. In a majority of patients (73%), the development of invasive adenocarcinoma was preceded by detection of dysplastic epithelium. In all patients who underwent surgery for high grade dysplasia, previous endoscopic biopsy specimens had shown low grade dysplasia (fig 1). These data support the theory that malignant progression in Barrett’s oesophagus occurs through stages of increasing severity of dysplasia.17 ,37-41 Although “regression” of low grade dysplasia seemed to occur, the subsequent development of adenocarcinoma or high grade dysplasia suggests that this observation was probably due to sampling error or histopathological misinterpretation.
Endoscopic surveillance of patients with Barrett’s oesophagus involves the critical question of how to manage the patient with high grade dysplasia. In some centres, as in our hospital, unequivocal high grade dysplasia is regarded as the end point of surveillance for patients who are likely to tolerate oesophageal resection.11-13 ,42 ,43 Others, however, reserve surgical intervention for proven invasive adenocarcinoma and perform continued surveillance for high grade dysplasia by strict endoscopic biopsy protocols.39 ,44 ,45 Because of the controversial role of oesophagectomy for a biopsy diagnosis of high grade dysplasia alone, we performed a separate analysis including only those patients who were operated on for invasive adenocarcinoma. It is of note that this selective analysis still showed a significant survival benefit for those patients in whom the cancer had been detected during surveillance as compared with those who initially presented with Barrett’s carcinoma.
The data presented indicate that endoscopic biopsy surveillance of patients with Barrett’s oesophagus permits detection of cancer at an early, curable stage. These findings, in line with those reported by other investigators,26 ,29 ,30 ,46 ,47 support the clinical practice of endoscopic surveillance in Barrett’s oesophagus. In our study, none of the patients in the surveillance group had advanced stages of adenocarcinoma, whereas 56% of patients in the non-surveillance group had stage III or IV tumours. Subsequently, comparison of survival after operative treatment showed a significant difference between the two groups. This striking difference strongly suggests a long term reduction in cancer mortality by widespread surveillance of Barrett’s oesophagus.
Acknowledgments
We wish to thank all referring specialists who contributed to this study by sending us the original reports on endoscopic and biopsy examinations which were performed at their institutions. Part of this work has previously been published in abstract form (Van Sandick JW, Van Lanschot JJB, Kuiken BW,et al. The effect of endoscopic biopsy surveillance on pathological stage of resected Barrett’s carcinoma and postoperative survival. Eur J Gastroenterol Hepatol 1996;8:A55; and Van Sandick JW, van Lanschot JJB, Tytgat GNJ, et al. The impact of endoscopic biopsy surveillance of Barrett’s esophagus on pathological stage and postoperative survival of Barrett’s carcinoma.Gastroenterology1997;112:A672).