Article Text

Abstract
Background—Patients who complain of constipation can be divided into those who have lost the natural call to stool, but develop abdominal discomfort after several days without a bowel movement (no urge); and those who experience a constant sensation of incomplete evacuation (urge).
Aims—To determine whether the two groups differ in symptoms, colonic transit, and perceptual responses to controlled rectal distension.
Methods—Forty four patients with constipation were evaluated with a bowel symptom questionnaire, colonic transit (radiopaque markers), and rectal balloon distension. Stool (S) and discomfort (D) thresholds to slow ramp (40 ml/min) and rapid phasic distension (870 ml/min) were determined with an electronic distension device. Fifteen healthy controls were also studied.
Results—All patients had Rome positive irritable bowel syndrome (IBS); 17 were no urge and 27 urge. Mean D threshold to phasic rectal distensions was 28 (3) mm Hg in no urge, 27 (3) mm Hg in urge (NS), but higher in the control group (46 (2) mm Hg; p<0.01). Sixty seven per cent of no urge and 69% of urge were hypersensitive for D. Slow ramp distension thresholds were higher in no urge (S: 26 (3); D: 45 (4) mm Hg) compared with urge (S: 16 (2); D: 31 (3) mm Hg; p<0.01), or with controls (S: 15 (1); D: 30 (3); p<0.01).
Conclusions—Hyposensitivity to slow rectal distension is found in patients with IBS who complain of constipation and have lost the call to stool even though their sensitivity to phasic distension is increased.
- visceral sensation
- colonic transit
Statistics from Altmetric.com
Patients who complain of constipation may base their self assessment on specific symptoms such as straining during defecation, passage of hard stools, a sensation of incomplete evacuation, or a decreased frequency of bowel habits.1 2 Patients may also use additional subjective criteria for normalcy in judgements of defecation patterns. For example, the perception of an adult patient of being constipated may be influenced by parents’ expectations of bowel habit frequency during the patient’s childhood, by cosmetic criteria (abdominal distension), or by psychological traits (for example, obsessive-compulsive).3 The term constipation is ambiguous and often misleading and this is supported in part by a poor correlation between the subjective definition and whole gut transit time.4 Regardless of the criteria used to make a self diagnosis, the altered perception of visceral sensations may play an important role in the patient’s self assessment. For example, a patient may feel constipated because she or he has a constant sensation of abdominal fullness or gas, or an urge to have a bowel movement, but is unable to eliminate this sensation by going to the toilet. The same holds true for the sensations of incomplete rectal evacuation following a bowel movement. Alternatively, a patient may feel constipated because he or she never experiences a normal call to stool or urge to have a bowel movement, but develops symptoms of abdominal discomfort after several days without evacuation.
It has been estimated that a large number of patients complaining of constipation meet diagnostic criteria for irritable bowel syndrome (IBS).4 5 Using an ascending series of phasic distensions, we have previously shown the presence of hypersensitivity to rapid rectal balloon distension in about half of all patients with IBS.6 Similar to findings by Oettle and Heaton,7 this hypersensitivity did not correlate with symptoms of rectal hypersensitivity, such as sensation of incomplete evacuation. It has been suggested that patients who have lost the ability to perceive normal rectal sensations may be characterised by the opposite sensory alteration, the “hyposensitive rectum”.8 A number of investigators have reported the presence of rectal hyposensitivity in patients with constipation.3 9-11 However, the methods used in these studies to assess perception of rectal stimuli make it difficult to determine whether patients had IBS, and whether the observed perceptual alterations were due to alterations in rectal compliance or due to response bias.12
Perception of rectal sensations requires the transmission of sensory signals via primary afferents to the spinal cord and to cortical brain regions. While patients with pelvic nerve or sacral spinal cord lesions lose completely the ability to perceive physiological rectal sensations,13 they may still perceive the discomfort associated with rapid rectal distension.14 The differentiation between different rectal sensations such as stool, urgency, gas, and the association of aversive descriptors to any or all of these sensations almost certainly involves learning processes in early childhood.15 For example, children suffering from pathological faecal retention lose the normal call to evacuate their bowels, even though their rectum becomes severely overdistended (megarectum).15
In the current study, we wanted to characterise perceptual alterations in response to rectal balloon distension in patients with the primary complaint of constipation. By using a computerised distension device, we sought to answer the following specific questions:
(1) What is the predominant perceptual abnormality during rectal distension in patients with a primary complaint of constipation?
(2) Do perceptual responses to rectal distension correlate with predominant symptoms (sensations of incomplete rectal evacuation versus lack of call to stool)?
(3) What is the correlation of perceptual response to slow and rapid rectal distension? Parts of the results have previously been published in abstract form.16
Methods
subjects
Normal controls
Fifteen healthy subjects (seven females and eight males; mean age 37 years, range 28–50) were recruited by advertisement. None had any evidence (by history or physical examination) of an acute or chronic illness. In particular, there was no evidence for a chronic pain syndrome or for abdominal symptoms either by bowel symptom questionnaire or by personal history. Results from these subjects were used to establish 95% confidence intervals for perception thresholds.
Patients with IBS
Anorectal sensory and motor functions were evaluated in 44 consecutive patients (31 females and 13 males) who presented to the UCLA Center for Functional Bowel Disorders and Abdominal Pain during 1994 with a primary complaint of constipation. All eligible patients had to meet the following criteria:
(1) their primary reason for consultation was chronic constipation;
(2) they met the Rome criteria17 for a diagnosis of IBS and had no evidence for organic disease; and
(3) constipation was defined by the presence of at least two of the following: straining more than 25% of the time; hard, dry, pebble-like stools more than 25% of the time; less than three bowel movements in a week, plus the absence of loose stools.17
Based on the predominant symptom, patients with constipation were divided into two categories: those who have lost the natural call to stool, but develop abdominal discomfort after several days without a bowel movement (no urge constipation), and those who experience a constant sensation of rectal fullness which fails to disappear with bowel movements or incomplete evacuation (urge constipation). The mean age of all constipated patients was 48 years (range 22–88). Table 1summarises the clinical characteristics of patients, including symptom severity and number of bowel movements. Informed consent was obtained from each subject.
Clinical characteristics, prevalence of severity, symptom criteria, and colonic transit time in the IBS constipation predominant subgroups
assessment of colonic transit time
Total and segmental colonic transit times were assessed as previously described.18 Twenty radiopaque markers were ingested at the same time on days 1–3. Abdominalx rays were obtained on days 4 and 7 at the same time as the pellets were ingested, and the markers were readily identified and counted on the abdominal xray films.
questionnaires
Bowel symptom questionnaire
At the time of their first encounter at the UCLA functional bowel clinic, patients completed a detailed questionnaire regarding their bowel habits, abdominal symptoms, and quality of life.6The questionnaire is the Talley bowel symptom questionnaire19 with nine additional measures of bowel function and abdominal pain. We analysed 41 questions that included six on type of IBS symptoms (Manning criteria), one on symptom severity, nine indicating various types of abdominal discomfort, three describing bowel habit, and five characterising constipation. To categorise the patients into either one of our two study groups (no urge and urge), patients who assessed their bowel habit as constipation were asked to chose the statement that best characterised their situation:
(1) I never experience any urge to have a bowel habit; or
(2) the main reason I keep going to the toilet is to get rid of the fullness in my rectum, but most of the time I am not successful.
Psychological symptom questionnaire
Patients completed the SCL-90 psychological symptom questionnaire,20 which assesses symptom severity in the following areas: anxiety, depression, hostility, interpersonal sensitivity, obsessive-compulsive behaviour, paranoia, phobic behaviour, psychosis, and somatisation. Scale scores are reported as T scores based on a non-psychiatric patient normative sample. Scales with T scores above 63 (0–100 scale) indicate the presence of psychological symptoms.
equipment
Stimulation device
A computer driven volume displacement device was used to inflate a balloon continuously at a constant volume rate of 40 ml/min (ramp distension) or rapidly to a constant pressure plateau (phasic distension). The distension device, which records pressures and volumes simultaneously (sampling rate of one per second), was connected to a subject operated marker device that logs the sensation of stool or discomfort onto the data file as balloon inflation occurs. When a subject triggered the marker for discomfort during phasic or ramp distension, the balloon was instantaneously deflated. There was a fixed pressure limit that automatically triggered balloon deflation for pressures above 70 mm Hg or volumes above 500 ml.
Rectal balloon
A latex balloon was attached to a silicone elastomer tube (outer diameter, 18F) and tied at both proximal and distal ends (MAK-LA, Los Angeles, California). The distance between the two attachment sites was 11 cm. Distension to a maximal volume of 500 ml resulted in a spherical balloon shape. The balloon was inflated repeatedly before use to rule out leaks and to measure its intrinsic compliance. In preliminary studies, it was found that during the initial three balloon inflations, the maximally reached balloon pressure decreased by 10%. After this initial decrease, the volume-pressure relation of the balloon remained constant during subsequent inflations. For determining sensory thresholds to ramp distensions, balloon pressures at each volume were automatically subtracted from rectal pressures by the Barostat software. The balloons were tested again after completion of each experiment to ensure that there were no leaks or changes in compliance with repeated inflation. The lubricated balloon was inserted into the rectum so that the distal attachment site was 4 cm from the anal verge. The tube was then secured in its proper position with tape.
experimental procedure
The subjects were placed in a lateral decubitus position on a padded table. The examiner was always present but did not interact with the subjects after the initial explanation of the respective task. Patients were not instructed about the nature of the distension protocols—that is, continuous ramp distension versus intermittent phasic distension. It was emphasised to the subjects that they had full control over the protocol by being able to deflate the balloon instantaneously at any time of significant discomfort. Subjects had no visual or auditory cues to anticipate the type or the time course of distensions. All experiments were performed after a 12 hour fast following the application of two Fleet’s enemas containing 19 g of monobasic sodium phosphate and 7 g of dibasic sodium phosphate (CB Fleet Co., Inc., Lynchburg, Virginia).
Continuous ramp distension
All subjects had balloon inflation at a constant volume rate of 40 ml/min to a maximum of 500 ml or a maximum pressure of 70 mm Hg. Patients were given a hand held button box (labelled as “no sensation”, “gas”, “stool”, and “discomfort”). Subjects were asked to record their sensations continuously by pressing and holding down the respective button for as long as they experienced a particular sensation. If the discomfort button was pressed, or the volume or pressure limit was reached, the balloon was automatically deflated.
Ascending series of stimuli
A modified ascending series of 30 second rapid phasic pressure stimuli (15, 10, 25, 20, 35, 30, 45, 40, and 50 mm Hg) were separated by 30 second interstimulus rest at 5 mm Hg. Following each pressure stimulus of the nine trial sequence, the participant labelled the sensation during the inflation using one or more words from a list of qualitative descriptors of rectal sensation (no sensation, gas, stool, discomfort). The volume required to maintain baseline pressure remained constant during the phasic distension procedure.
evaluation of outcome parameters
Perceptual response to ramp distension
Subjective thresholds for sensation of stool and discomfort were determined from the lowest pressure at which the stool and discomfort buttons were pressed. At each threshold, pressure and volume were recorded and used to calculate wall tension.
Perceptual response to ascending series phasic distension
Perceptual thresholds were determined from the lowest pressure at which a subject used a particular descriptor. For example, if discomfort was first reported at 30 mm Hg, 30 mm Hg was taken as the discomfort threshold for this subject.
Wall tension
Wall tension was estimated as previously described.6 14 Radius at each pressure stimulus was derived from the volume of the cylinder (V = πr2L, in which L=11 cm). Using La Place’s law (cylinder, T=2pr), wall tension (T) was calculated from the estimated balloon radius and the delivered pressure (p).
statistics
Data are expressed as mean (SEM). The ttest statistic was used to evaluate group differences for continuous variables. Significance was set at the p<0.05 level.
Results
clinical characteristics
Table 1 and fig 1 show the clinical characteristics of the two groups. Mean age of all patients was 48 years (range 22–85) with 2–3 times more female patients than males. Three per cent of all patients rated their symptoms as mild, 35% as moderate, 32% as severe, and 29% as very severe. There were no group differences in age and sex distribution and overall severity ratings, except for a greater proportion of patients in the urge group (44%) who rated their symptoms as “severe” (p<0.05; table 1). The majority of patients in both groups had less than three bowel movements per week, and reported straining and dry, hard, pebble-like stools. Twenty seven per cent in the no urge group and 41% in the urge group reported more than five bowel movements per week. No group differences were found regarding the characterisation of pain/discomfort; presence of straining or hard stool; defecatory habits or frequency; or use of bran or laxatives.
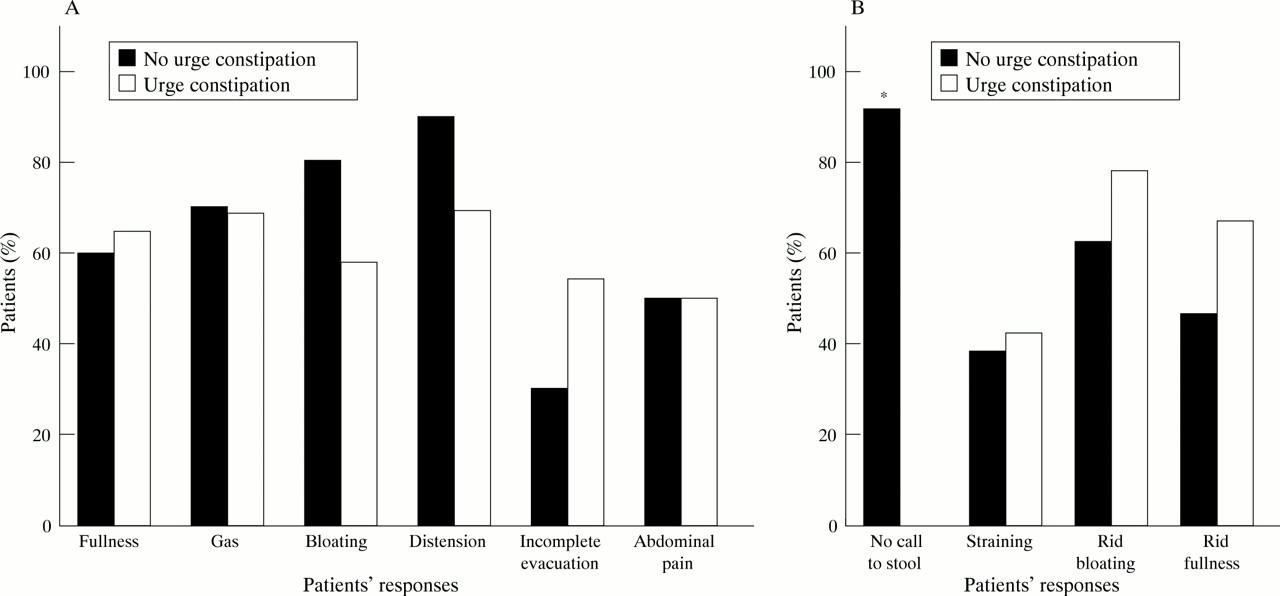
(A) Prevalence of abdominal symptoms. (B) Prevalence of defecation related symptoms. *p<0.01.
There were no constipation group differences in the mean T score of any of the SCL-90 psychological symptom scores (table 2). Using a symptom presence cut off score of T>63, the most common abnormalities in the no urge group were obsessive-compulsive (42%) and interpersonal sensitivity (42%), while in the urge group, depression (75%) and somatisation (67%) were most common.
Mean (SEM ) T score of psychological symptoms in patients with constipation predominant IBS
perceptual responses
Thresholds during ascending series of phasic pressure stimuli
Figure 2 shows thresholds for stool and discomfort obtained in the three groups. The mean stool thresholds in response to phasic rectal distension were not significantly different between the three groups (25.3 (3.1) mm Hg in no urge; 20.7 (2.1) mm Hg in urge; and 23.1 (1.9) mm Hg in controls). In contrast, while the mean discomfort thresholds were not significantly different between the two patient groups (no urge: 28.1 (3.4) mm Hg; urge: 26.7 (3.0) mm Hg), they were significantly higher in the controls (45.8 (2.2) mm Hg; p<0.01 compared with both patient groups). In the controls, threshold pressures for discomfort were higher than those for stool sensation (45.8 (2.2) mm Hg versus 23.1 (1.9) mm Hg, p<0.01), but this was not so in the patients (27.4 (2.2) mm Hg versus 22.5 (1.8) mm Hg, NS). Most of the patients (69% and 67% respectively of the urge and no urge groups) felt discomfort at pressures lower than the normal range as defined by the 95% confidence limits of the normal controls. Also, there were no significant group differences in the perceived intensity of rectal stimuli at the discomfort threshold (2.7 (0.6) in no urge; 3.6 (0.7) in urge).

Perceptual responses to phasic distension.**p<0.01.
Ramp thresholds
Figure 3 shows mean perception thresholds in the three groups during slow ramp distension of the rectum. The mean stool (S) and discomfort (D) pressure thresholds were significantly higher in the no urge group (S: 25.8 (3.4); D: 44.9 (4.0) mm Hg) when compared with the urge group (S: 15.6 (1.8); D: 31.4 (2.9) mm Hg; both p<0.01), or compared with controls (S:15.4 (1.3); D: 29.7 (2.7) mm Hg; both p<0.01). When reported with reference to wall tension, perception thresholds in the no urge group for stool and discomfort were significantly higher (S: 52.8 (11.8); D: 120.0 (14.5) mm Hg × cm) when compared with perceptual thresholds in the urge group (S: 28.7 (4.2); D: 80.8 (10.5) mm Hg × cm; both p<0.05), or when compared with control subjects (S: 29.3 (3.7); D: 82.0 (7.7) mm Hg × cm; both p<0.05).

{kind=link}
{kind=link}
{kind=link}
Perceptual responses to slow ramp distension. Shown are mean values for intrarectal pressure (A) and rectal wall tension (B) at which subjects first reported the sensation of stool and discomfort. Both stool and discomfort thresholds were significantly higher in the no urge group when compared with the urge group or control subjects. *αp<0.01, *βp<0.03, *γp<0.04.
Perception thresholds for stool and discomfort during ramp distension were highly correlated in patients (r=0.58; p<0.01 for no urge and urge combined;r=0.51; p=0.61 for no urge;r=0.48; p=0.02 for urge) but not in controls (r=0.20; p<0.95).
Colonic transit time
The mean colonic transit times for both groups were within the normal range and did not differ between the no urge (total = 66.6 (11.4); right colon = 17.2 (3.8); left colon = 22.4 (4.8); and rectosigmoid = 26.9 (7.2) hours) and the urge group (total = 60.2 (10.7); right colon = 17.8 (4.2); left colon = 26.4 (4.4); and rectosigmoid = 16.0 (4.5) hours).
Discussion
In the current study, we have identified two subgroups of patients with IBS with a primary complaint of constipation, which can be distinguished on the basis of distinct patterns of perceptual responses to rectal distension in addition to specific symptoms. The majority of patients within both groups shared the finding of a lowered discomfort threshold during an ascending series of rapid phasic distensions that we have previously shown in patients with IBS regardless of predominant bowel habit.6 In addition, one group exhibited evidence for a coexisting hyposensitivity to slow distension.
In the healthy individual, the vast majority of afferent information arising from the gastrointestinal tract is not consciously perceived. The conditioning of the defecation response occurs early in life during toilet training when the child learns to focus attention on sensations arising from the rectum and experiences that the discomfort associated with rectal fullness can be relieved by passing a bowel movement in a socially acceptable context. Conversely, and in analogy to sensations related to the urinary bladder, a healthy individual can learn to withdraw attention from rectal sensations if the call to stool occurs at an inappropriate time.
subtypes of constipation based on symptoms
In the current study, the chronic perception of discomfort in the form of bloating type symptoms was the most common symptom listed by patients in both constipation groups. This finding is in agreement with our recent report on predominant symptoms in a large population of patients with IBS, which identified bloating type symptoms as significantly more common than abdominal pain.21 However, the type of alteration in visceral sensation differed between the two groups: one subset of patients had a persistent sensation of rectal fullness, which they were not able to relieve by defecation; the other subset had lost the normal call to stool or urgency associated with rectal filling, but was afraid of the expected development of bloating type symptoms if no regular defecation was induced. Many patients with no urge constipation will take laxatives or enemas before such expected discomfort occurs, resulting in an unexpected high frequency of bowel movements.
There are several possibilities which could explain these different symptom patterns. In the no urge group, a notably increased rectal compliance may increase the amount of stool required to stimulate a perceptual response, a finding common in children with faecal retention syndrome.22 In addition, slow transit and/or small volume stool may result in an inadequate stimulation of rectal mechanoreceptors. However, the same number of patients in both groups reported the presence of hard, dry, pebble-like stools. Similarly, while total colonic transit time was at the upper limit of normal in the no urge group, it was not different from mean transit times in patients who reported a constant sensation of urge. In the urge group, altered visceral sensations could result from an inability to empty the rectum completely secondary to functional anorectal outlet obstruction, or from structural anorectal abnormalities, such as rectal prolapse. However, left colonic transit times and rectal compliance in the urge group were not different from those in the no urge group, and patients with organic anorectal disease had been excluded from our study. Thus, it is unlikely that motor or structural alterations were responsible for the different types of predominant symptoms in the two constipation groups.
altered perceptual responses to rectal distension
We found that perceptual responses during distension of the rectum at rates comparable to physiological distension, clearly distinguished the two patient groups. Regardless of the pressure or wall tension at which patients first indicated discomfort during an ascending series of phasic pressure stimuli, patients with no urge constipation had significantly higher perception thresholds during slow ramp distension, both for the physiological sensation of stool, and for the aversive sensation of discomfort.
The findings of differential perceptual responses to phasic and slow ramp distension of the rectum, the first one distinguishing patients from controls but not separating urge from non-urge patients, and the later one separating the two patient groups but not differentiating between urge and controls, support concepts previously proposed by our group. Lembo et al reported that the tendency of patients with IBS to rate rectal sensations induced by balloon distension as discomfort at a lower stimulus intensity than control subjects, is specific for phasic distensions and may involve specific afferent pathways.14 Recent evidence from Naliboff et al strongly supports the concept that the perceptual alteration observed during ascending series of phasic rectal distension is more related to a hypervigilance towards aversive and potentially noxious visceral stimuli.23 This hypervigilance may be related to an exaggerated activation of attentional systems towards aversive visceral sensations manifested as a learned tendency of patients with IBS to use the aversive discomfort at lower stimulus intensities than control subjects, and to tolerate smaller distension pressures.
The abolished perceptual responses to slow rectal distension in the presence of pelvic nerve damage13 or lesion in the lower spinal cord,14 suggests the concept that slow ramp (but not phasic) distension mimics the stimulation of pelvic nerve afferents that occurs during physiological rectal filling. In principle, the observed rectal hyposensitivity in response to physiological rates of rectal distension could be secondary to alterations in compliance or to idiopathic or laxative induced rectal afferent nerve damage. Differences in compliance are unlikely to explain our findings since hyposensitivity was observed both in reference to rectal pressure and wall tension. Similarly, there are no prospective data to support the concept of laxative induced nerve damage, and we did not find differences in laxative use between the patient groups. Even though the patient group as a whole was somewhat older than the normal control subjects, there was no age difference between the two constipation groups. An alternative explanation is related to possible alterations in central processing of visceral afferent information arising from the rectum, such as activation of pain inhibitory systems or attenuation of central arousal systems.
Bernstein et al have shown that patients with Crohn’s disease limited to the small bowel also exhibit rectal hyposensitivity which is only seen during slow ramp distension.24 Based on experimental results in animals, we hypothesised that the chronic noxious afferent input to the central nervous system, arising from the inflamed small intestine, activates pain inhibitory mechanisms which decrease the perception of visceral stimuli arising from non-inflamed gut. In an analogous fashion, a tonic increase in the activity of such antinociceptive systems could explain the hyposensitivity observed in the current study. Alternatively, the observed hyposensitivity may result from a failure to activate central attentional systems in response to physiological rectal filling.25
In summary, this is the first report of a subset of patients with a primary complaint of constipation which is characterised by distinct patterns of visceroperceptual alterations, and which can be identified by specific symptoms. It may be hypothesised that different alterations in attentional systems may be responsible both for the hypervigilance towards potentially aversive stimuli and the hyposensitivity for physiological rectal stimuli. The hyposensitive subset of patients with constipation predominant IBS may not benefit from current therapeutic strategies with visceral analgesics.
Acknowledgments
This work was supported in part by funds from the Veterans Administration and by NIH grant DK 48351.