Article Text

Abstract
Background and aims: Irritable bowel syndrome (IBS) is a disorder of intestinal hypersensitivity and altered motility, exacerbated by stress. Functional magnetic resonance imaging (fMRI) during painful rectal distension in IBS has demonstrated greater activation of the anterior cingulate cortex (ACC), an area relevant to pain and emotions. Tricyclic antidepressants are effective for IBS. The aim of this study was to determine if low dose amitriptyline reduces ACC activation during painful rectal distension in IBS to confer clinical benefits. Secondary aims were to identify other brain regions altered by amitriptyline, and to determine if reductions in cerebral activation are greater during mental stress.
Methods: Nineteen women with painful IBS were randomised to amitriptyline 50 mg or placebo for one month and then crossed over to the alternate treatment after washout. Cerebral activation during rectal distension was compared between placebo and amitriptyline groups by fMRI. Distensions were performed alternately during auditory stress and relaxing music.
Results: Rectal pain induced significant activation of the perigenual ACC, right insula, and right prefrontal cortex. Amitriptyline was associated with reduced pain related cerebral activations in the perigenual ACC and the left posterior parietal cortex, but only during stress.
Conclusions: The tricyclic antidepressant amitriptyline reduces brain activation during pain in the perigenual (limbic) anterior cingulated cortex and parietal association cortex. These reductions are only seen during stress. Amitriptyline is likely to work in the central nervous system rather than peripherally to blunt pain and other symptoms exacerbated by stress in IBS.
- IBS, irritable bowel syndrome
- CNS, central nervous system
- fMRI, functional magnetic resonance imaging
- ACC, anterior cingulate cortex
- TCAs, tricyclic antidepressants
- SSRIs, selective serotonin reuptake inhibitors
- PET, positron emission tomography
- amitriptyline
- rectal pain
- anterior cingulate cortex
- irritable bowel syndrome
- tricyclic antidepressants
- functional magnetic resonance imaging
Statistics from Altmetric.com
- IBS, irritable bowel syndrome
- CNS, central nervous system
- fMRI, functional magnetic resonance imaging
- ACC, anterior cingulate cortex
- TCAs, tricyclic antidepressants
- SSRIs, selective serotonin reuptake inhibitors
- PET, positron emission tomography
- amitriptyline
- rectal pain
- anterior cingulate cortex
- irritable bowel syndrome
- tricyclic antidepressants
- functional magnetic resonance imaging
Irritable bowel syndrome (IBS) is a common disorder characterised by symptoms of altered bowel habits and abdominal pain or discomfort. Symptoms of IBS are thought to be due to a combination of abnormal intestinal motility and intestinal hypersensitivity to stimulation.1–5 Central nervous system (CNS) upregulation of motility and sensation, in part due to psychosocial stressors, is also thought to be involved in IBS.6,7 Tricyclic antidepressants (TCAs) are widely used for chronic painful conditions, including irritable bowel syndrome (IBS). Several controlled trials have demonstrated benefits of this class of drug for IBS, especially when pain is a prominent symptom.8,9 The benefits of TCAs have recently been summarised in the American Gastroenterology Association technical review on IBS.10 The mechanism of this benefit is unclear but is unlikely due to an antidepressant effect since: (1) benefits occur in non-depressed patients; (2) doses effective for IBS are generally below the effective antidepressant dose; (3) and treatment responses for IBS occur earlier than the antidepressant effect. Potential mechanisms for TCAs to benefit IBS include a reduction in intestinal pain sensitivity, mediated either in peripheral nerves or the CNS, and reduction in CNS upregulation of sensation and motility by psychosocial stressors. An anticholinergic effect of TCAs on the gut to reduce motility is a less likely mechanism as anticholinergic agents give less benefit.11
TCAs block transporters of the neurotransmitters norepinephrine and serotonin. These transporter proteins are responsible for uptake of neurotransmitters after release at the nerve endings. The antidepressant effect is thought to occur in the CNS where levels of norepinephrine and serotonin at the nerve ending are initially increased with therapy. Firing of the primary source of CNS norepinephrine, the locus coeruleus, is inhibited which may mediate the antianxiety effects of TCAs.12,13 Subsequently, norepinephrine and serotonin receptors on neurones are downregulated, which temporally correlates with the antidepressant effect.14 In the treatment of depression, selective serotonin reuptake inhibitors (SSRIs) are likely to interact with areas of the brain involved in emotions, including the anterior cingulate cortex (ACC). Baseline metabolic activity in this brain region determined by positron emission tomography (PET) correlates with success of therapy for depression with SSRIs.15 The experience of negative emotions such as sadness is also associated with metabolic activity in the ACC, as measured by PET.16,17 The ACC is also involved in CNS processing of pain, particularly the affective component.18–20 Several functional brain imaging studies have indicated that anterior cingulate activity correlates with subjective pain reports in response to noxious stimuli, including gastrointestinal ones.20–23 Previously, we have demonstrated increased activation of the ACC during painful rectal distension in IBS patients compared with controls. Rectal balloon distension is used as a laboratory model to study IBS as it demonstrates visceral hypersensitivity and generally reproduces IBS symptoms.3 Subsequent studies suggest this increase is restricted to the caudal portion of the anterior cingulate.24 This portion of the anterior cingulate has been termed the cognitive division (ACC-CD) given its prominent activation by decision making and pre-motor activities, in addition to pain intensity.25–27
As the anterior cingulate is a brain region involved in emotions and pain, and has been predictive of antidepressant responses, our hypothesis was that TCAs would reduce pain related activation of this region in IBS. Our aim was to determine whether the TCA amitriptyline reduces ACC activation in response to rectal pain in IBS patients with recurrent abdominal pain. Other brain areas with reduced pain related activation with amitriptyline were also sought. Secondary aims were to determine if amitriptyline reduces pain ratings in response to rectal distension and if the effects are more prominent during stressful conditions as stress appears to be an important IBS trigger and increases pain sensitivity to rectal distension in IBS.6
MATERIALS AND METHODS
Subjects
Twenty two women with IBS and significant pain related to it were enrolled in the study. Mean age was 39 years (range 24–57). Eleven had diarrhoea predominant symptoms, seven had constipation predominant symptoms, and four had alternating bowel habits. All patients satisfied Rome II criteria for IBS. Prior to enrolment each had a complete history and physical examination, complete blood count, and colonoscopy to exclude other diseases that might simulate IBS. Patients with diagnosed psychiatric or CNS disorders, those taking central nervous system acting medications, those with major cardiopulmonary disease, or those with disorders which might effect visceral sensitivity (for example, diabetes) were excluded from participation. Although no IBS patient had clinically overt depression or anxiety disorders, psychological survey (SCL-90) indicated prevalent psychological symptoms in IBS patients. Of study completers, 10/19 IBS patients had depression symptoms (⩾2 SDs above established norms), 6/19 had anxiety symptoms, and 8/19 had increased general psychological symptoms (general psychological index). Beta-HCG was analysed to exclude pregnancy prior to enrolment, and subjects practised contraception or abstinence to prevent pregnancy during the study.
Nineteen patients completed the study: one dropped out for unknown reasons, one due to an unexpected pregnancy, and one due to a bowel obstruction. None dropped out due to side effects of the medication. Based on preliminary data, a sample size of 19 was determined to give adequate statistical power (0.8) to identify a 33% reduction in ACC blood flow during painful rectal distension with sensitivity of 0.05 by paired t test.
Drug administration
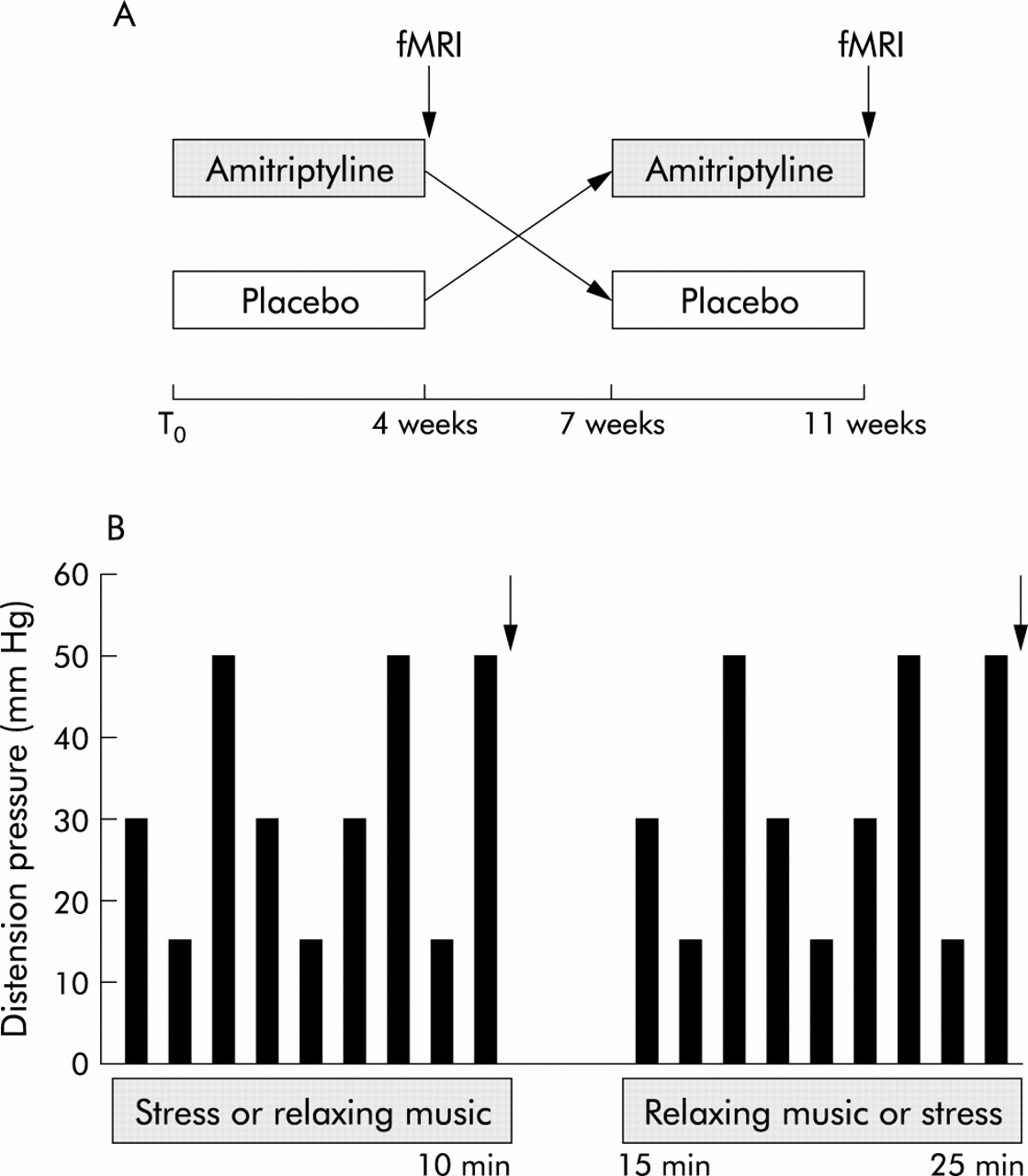
The study was a randomised, placebo controlled, double blind, crossover design. Patients took amitriptyline 25 mg at bedtime for one week, then 50 mg at bedtime during weeks 2–4 or matching placebo. There was a three week washout period after which patients crossed over to the alternate treatment (fig 1A). The order of treatment was randomly determined by the Vanderbilt investigational pharmacy. This study was designed to assess drug effects, so a placebo arm was used rather than a pre- and post-treatment design. In this way, order effects such as habituation to rectal distension and fMRI procedure, and expectancy due to drug treatment were minimised. The investigators and patients were blinded to treatment. The protocol was approved by the Vanderbilt institutional review board.

Study protocol. (A) Patients were randomly allocated to placebo or amitriptyline treatment for four weeks. At the end of the month there was a three week washout, followed by crossover for four weeks of the alternate treatment. Assessment of symptoms, and rectal distension with functional magnetic resonance imaging (fMRI) was performed at the end of each treatment phase (arrows). (B) Rectal distension and fMRI were performed as indicated. A series of nine distensions (three at each pressure) were administered for 40 seconds each, followed by a 30 second baseline at 4 mm Hg during either stressful sounds of babies crying or relaxing music, the order determined randomly. Distensions were repeated with the alternate stress condition. Subjects rated the intensity of the most intense stimuli at the end of each series of stimuli (arrows).
Symptom rating
Patients completed a psychological symptom survey prior to beginning treatment that assessed symptoms in the previous week (SCL-90).28 At the end of each treatment phase, patients rated their IBS symptoms during the last two weeks of each treatment using a hand held rater (IBS rater, ADHF).29 Abdominal pain, diarrhoea, constipation, bowel movement distress, and bloating were each rated separately on 0–10 visual analogue scales anchored by the descriptors none (0) and very severe (10).
Distension protocol
At the end of each treatment period, patients underwent rectal distension testing during fMRI to measure cerebral activation associated with rectal pain. Patients were tested under fasting conditions at 7:00 am, 40 minutes after a cleansing Fleet enema (CB Fleet, Lynchburg, Virginia, USA). An infinitely compliant bag, maximal volume 475 ml, 9 cm diameter when fully inflated (MUI scientific, Mississauga, Ontario, Canada), was attached to a rectal tube, 6 mm outer diameter. The tube and balloon were inserted into the rectum after lubrication, with the distal bag margin 5 cm beyond the anal verge. Intravenous tubing (3 m) connected the rectal tube to a barostat distending device (maximal inflation rate 38 ml/s; Medtronic/Synectics, Shoreview, Minnesota, USA) outside the MRI suite. Subjects reclined supine on the MRI scanning table. Headphones were placed to reduce sound from the MRI scanner and to administer auditory conditions, either stressful or relaxing. Padding and a chin strap held the head to prevent motion. A pulse oximeter probe was placed on the right index finger and a blood pressure cuff on the left arm for autonomic measurements. The barostat was programmed to administer nine distensions lasting 40 seconds each, separated by 30 second rest periods at a pressure of 4 mm Hg. Based on previous data from our group, it was established that the fMRI signal returned to baseline within 10 seconds of cessation of a distending stimulus.22 Distensions included three stimuli at 15 mm Hg, three stimuli at 30 mm Hg, and three stimuli at 50 mm Hg in an unpredictable order to reduce the effects of anticipation (fig 1B). These pressures were selected based on previous data to elicit sensations of gas or light pressure (15 mm Hg), stool or moderate pressure (30 mm Hg), or pain (50 mm Hg). Patients underwent the series of nine distensions during either relaxing music (“Stressbusters”, Beechwood Music LTD, Middlesex, UK) or a mixed tape of babies crying. Pilot studies indicated the crying babies tape was stressful to female volunteers, and was associated with reduced tolerance for ice water hand immersion whereas “Stressbusters” was not. The order of the auditory stress conditions was determined randomly but was maintained in the patient’s second study on the alternate drug condition.
Rectal pain sensitivity and stress during distension
At the end of each set of nine stimuli, the sounds were discontinued, and subjects were asked to verbally rate the most intense stimuli (50 mm Hg) during the balloon distensions on a 0–10 scale where 0 was non-painful and 10 was the worst pain imaginable.
Patients also verbally rated stress using the SSR questionnaire, composed of 13 rating scales anchored by opposing 0–10 adjectives related to stress, arousal, and attention.30 The alternate sound condition was then started, and the patient underwent a second series of nine distensions.
MRI scanning
BOLD (blood oxygen level dependent) imaging was performed on a 1.5 T General Electric Signa Horizon MRI system with echospeed gradients. Each study consisted of a three plane localiser (30 second scan time) followed by a three dimensional high resolution T1 weighted full brain sagittal anatomical data set with thin slices for normalisation purposes. A full brain axial two dimensional anatomical data set was then obtained for functional to anatomical image co-registration purposes. The functional scans were then performed during rectal distension. These were gradient echo EPI (echo planar imaging) images in the same location as the two dimensional axial anatomical set described above. Scan parameters were: field of view 24 cm, 64×64 voxels, TE 40 ms, TR 4000 ms, 153 acquisitions per slice, approximately 18 slices, 5 mm thick, 1 mm gap, flip angle 90°, band width 62.5 kHz, scan time 10 minutes 12 seconds. The functional scan was repeated during a second series of rectal distensions and the alternate auditory stress condition.
Data analysis
All images were transferred to an offline workstation for analysis using SPM99 image processing software (http://www.fil.ion.ucl.ac.uk/spm/spm99). After discarding the first four volumes to allow the system to reach equilibrium, all of the functional images were realigned to the first volume of the first functional data set to correct for any head motion during scanning. To compare data between subjects and groups of subjects, each data set was registered to a common template. This was done in SPM99 in four steps. (1) The two dimensional anatomical scan data set was co-registered to the three dimensional anatomical data set. (2) The functional dataset was co-registered to the two dimensional anatomical data set. This automatically co-registered the functional data set to the three dimensional anatomical data set. (3) The three dimensional anatomical data set was registered to the common template. (4) Transformation of the three dimensional anatomical data set to the template was applied to the functional data.
Once the functional data were co-registered to a common template, it was spatially smoothed to 8 mm full width half maximum. To determine activation of each voxel, the general linear model was used in SPM99 to determine the relationship between the input rectal distension pressure and the output signal variations. This resulted in three activation maps for each subject during stressful sounds and during relaxation music: low pressure (15 mm Hg) >baseline (4 mm Hg), medium pressure (30 mm Hg) >baseline, high pressure (50 mm Hg) >baseline. The primary outcome parameter was high pressure (50 mm Hg) >baseline.
Amitriptyline effects on global brain activation
To determine significant group differences in all patients between activation with placebo and activation with amitriptyline, a random effects approach was implemented in SPM99 using a paired t test. Model coefficients of the 50 mm Hg >baseline contrast were compared. Differences in pain related activation between amitriptyline and placebo were defined by p<0.01 to identify regions with decreased stimulus related activation on amitriptyline. For display purposes (see figs 2, 4), cluster connectivity of 5 voxels was applied to highlight physiologically relevant clusters. To quantify an overall effect of amitriptyline on stimulus related brain activation, the total numbers of activated voxels in each of these maps was determined. Global brain activation changes associated with amitriptyline use were compared between distension levels and stress conditions by χ2 analysis (p<0.05).

Brain activation by rectal pain during stress: reductions by amitriptyline. Orange and yellow pixels indicate brain regions with reduced pain related activation by amitriptyline (p<0.01 connectivity 5). The perigenual anterior cingulate cortex (white circles) and the left posterior parietal cortex (blue circles) had significant reductions by amitriptyline after correction for multiple comparisons by small volume correction. The numbers in white at the lower left of each axial brain slice indicate the distance in mm from the anterior commissure. The colour key (bottom right) indicates the T score for the pixels displayed, comparing activation during rectal pain and stress on placebo versus amitriptyline treatment. (A) Axial brain images. (B) Sagittal brain image.
Amitriptyline effects on regions of interest
To determine specific locations of amitriptyline effects on brain activation, regions of interest were selected on the template brain using software written in IDL (Research Systems, Inc., Boulder, Colorado, USA). Regions of interest were identified with the guidance of a senior neuroradiologist (RK). Regions of interest were selected to include areas of the brain thought to be important in pain processing and “limbic” areas involved in affective states. Pain related areas included the caudal anterior cingulate (ACC-CD), parietal lobe posterior to the central sulcus, the insular cortex, the thalamus, and the prefrontal cortex. Limbic areas included the amygdala, the hippocampus/parahippocampal gyrus, and the perigenual anterior cingulate. For each region of interest, the per cent of the region with differential activation by amitriptyline was determined, using p<0.01 as the activation threshold. SPM99 small volume correction analysis was used to determine whether the regions were significantly altered by amitriptyline after correction for multiple comparisons.
Brain activation with rectal pain and stress after placebo
In order to interpret the activation caused by amitriptyline, we investigated the changes in activation due to pain and auditory stress after placebo. To quantify these effects, each individual’s 50 mm Hg >baseline activation map was entered into a one sample t test. This random effects model performed with SPM99 yields an activation map showing regions with significant signal increases during the high distensions over baseline across the population of IBS subjects on placebo. A region of interest and small volume correction analysis was performed as above.
RESULTS
Symptom rating
Thirteen patients indicated that their IBS symptoms were better on amitriptyline, five reported better symptoms on placebo, and one reported no change on either treatment (p = 0.06 for preference of amitriptyline). Patient ratings of pain during the last two weeks of treatment by 0–10 visual analogue scale were 4.2 (0.5) on amitriptyline versus 5.3 (0.6) on placebo (lower scores indicate less severe symptoms, p = 0.2).
Rectal pain sensitivity and stress during distension
Rectal pain during distension and auditory stress was rated by the patients as 6.4 (0.4) during amitriptyline and 7.2 (0.4) on placebo (p = 0.1). During relaxing music, pain was rated as 5.7 (0.5) on amitriptyline and 6.0 (0.4) on placebo (p = 0.5). Eighteen of 20 patients reported that the discomfort or pain induced by rectal distension was similar to their IBS symptoms. Baseline anxiety and depression scores did not correlate with reductions in pain during amitriptyline.
Subjects rated stress symptoms during rectal distension and the two stress conditions by SSR questionnaire (0–10 visual analogue scales, 13 questions). During acoustic stress (babies crying), there were significant increases in the domains of stress (5.7 (0.5) v 7.5 (0.5)), anxiety (5.4 (0.5) v 6.7 (0.5)), and anger (5.3 (0.5) v 7.2 (0.6)) compared with relaxing music (p<0.01 for all comparisons). During amitriptyline, stress ratings were also increased by the auditory stressor. There were no reductions in stress ratings associated with amitriptyline use (compared with placebo) during either relaxing or stressful listening and rectal distension.
Autonomic measurements
Blood pressure and heart rate were measured during each distending stimulus and at baseline. Blood pressure and heart rate were similar with amitriptyline and placebo during all stimuli and baseline.
Amitriptyline effects on global brain activation
Amitriptyline use was associated with reduced cerebral activation during stress and rectal pain in IBS patients in 2.3% of brain voxels (fig 2). Conversely, only 0.08% of voxels had greater activity during amitriptyline use. Significant deactivations were not seen. The effects of amitriptyline on brain activation by rectal pain were greater during stressful listening compared with relaxing music. Only 0.9% of all brain voxels had reduced activation during amitriptyline and relaxing music, significantly fewer than during stress (p = 0.01). The inhibitory effect of amitriptyline was relatively specific for pain, rather than non-painful stimuli (fig 3).
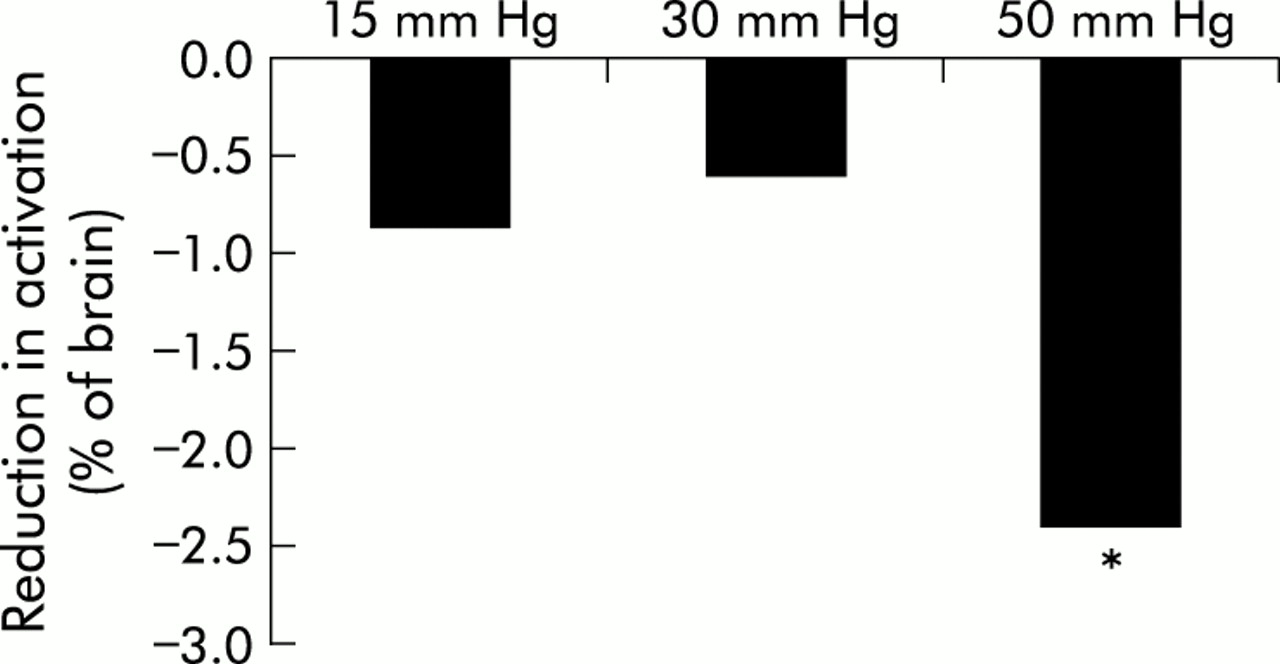
Rectal distension intensity and reduction in total brain activation by amitriptyline. Amitriptyline use was associated with reduced total brain activation during auditory stress and rectal distension. The reduction was substantially greater for painful level distension (50 mm Hg) than for lower levels of distension (p<0.05 v 15 and 30 mm Hg distension).
Amitriptyline effects on regions of interest
During rectal pain and stress, 4.5% of the voxels in both the perigenual cingulate and left posterior parietal regions had reduced activation with amitriptyline (table 1).
Reductions in regional brain activation during stress and rectal pain with amitriptyline
Small volume correction revealed that amitriptyline use was associated with significantly less activation in the perigenual anterior cingulate cortex (ACC-AD) and the left posterior parietal cortex (p<0.05 for each, corrected for multiple comparisons). No other regions investigated had significant alterations in activation associated with amitriptyline use. In the absence of auditory stress, no region had reduced pain related activation during amitriptyline. There was no correlation between reduction in brain activity during amitriptyline and anxiety or depression (by SCL-90 symptom survey).
Brain activation with rectal pain and stress after placebo
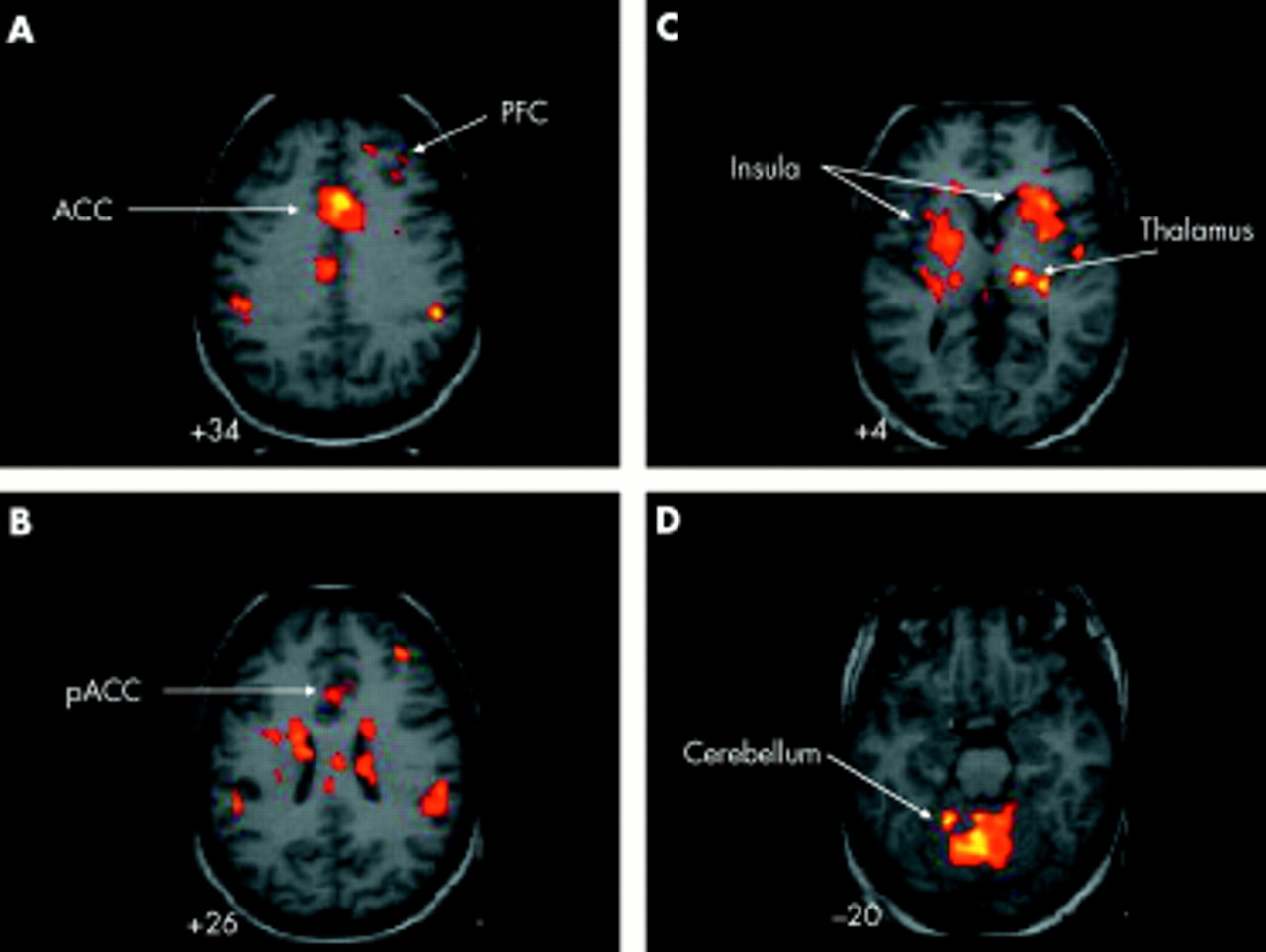
During painful rectal distension after placebo, prominent brain activation was observed in the perigenual (ACC-AD) and caudal anterior cingulate cortex (ACC-CD), bilateral insular cortices, thalamus, right prefrontal cortex, cerebellum, and anterior caudate nuclei. These activations were most prominent during stressful listening (fig 4). After correction for multiple comparisons in regions of interest, significant activation sets were identified in the perigenual anterior cingulate (Z max 3.82, −x,y,z 14, 16, 24; n = 220 voxels in the set, p = 0.0001), the right insular cortex (Z max 5.63, x,y,z −38, 4, −2; n = 362 voxels in the set, p = 0.001), and the right prefrontal cortex (Z max 3.94, x,y,z −32, 28, 8; n = 216 voxels in the set, p = 0.0001) during rectal pain and stress. There was no correlation between anxiety and depression (by SCL-90 survey) and brain activation during rectal pain.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Brain activation by rectal pain during stress after placebo. Orange and yellow pixels indicate brain regions with pain related activation during stress (p<0.001 connectivity 5). Prominent activations during pain and stress include the caudal anterior cingulate (ACC) (A), right prefrontal cortex (PFC) (A, B), perigenual anterior cingulate (pACC) (B), and bilateral insular cortices verging on the anterior caudate (C), thalamus (C), and cerebellum (D).
DISCUSSION
Low dose amitriptyline and other TCAs are widely prescribed for pain related to IBS and other painful conditions. Meta-analyses reveal improvement in pain conditions associated with their use.8,31 The mechanism of this benefit is unknown but a CNS action is suspected. Pain is a complex sensation combining sensory and affective components. Amitriptyline could improve pain by reductions of either the sensory or affective component. However, previous human studies of sensory effects of TCAs have not demonstrated convincing effects on pain thresholds or moderate pain sensation in the rectum or oesophagus in healthy controls.32,33 In subjects with functional bowel disease, gastric pain thresholds did not increase with one month of amitriptyline use (50 mg/day) despite clinical improvement.34 Treatment of IBS patients with amitriptyline (25 mg/day) has been associated with increased rectal pain thresholds, however the study was uncontrolled.35 No study has carefully evaluated the effect of TCAs on the affective component of pain.
The results of the current study indicate: (1) amitriptyline reduces global brain activation during rectal pain in IBS patients during mental stress. Effects during relaxing music and pain are much less; (2) significant reductions in pain related activation by amitriptyline occurred in the perigenual portion of the ACC and the left posterior parietal cortex. These brain regions are association cortices, thought to be related to emotional and cognitive function, respectively, rather than purely sensory areas36; and (3) reductions in brain activation were not definitely linked to reduced sensitivity to rectal pain or to clinical benefit although the study was not powered to identify such changes.
This study utilised a crossover design of drug administration and placebo control. While this may not be optimal for a clinical study of drug efficacy, it has the advantage of allowing each subject to serve as her own brain imaging control as there is evidence that individual variance in brain activation is substantial.37,38 Given changes in brain activation induced by anticipation of pain, it is likely that there would be changes in perception of rectal distension and brain activity after placebo ingestion. To focus purely on the effects of amitriptyline, we subtracted brain activation during amitriptyline from placebo. To reduce the effects of habituation with the protocol, we randomised the order of the placebo and amitriptyline administration. While carryover effects from amitriptyline use could still be a factor during subsequent placebo use, rectal distension fMRI testing would in this instance be seven weeks after amitriptyline, long enough for its effects to have been reversed.
Current theories of pain invoke a lateral pathway involved in sensory discrimination and a medial pathway which codes pain affect. Noxious stimuli from the periphery are thought to stimulate second order neurones in the dorsal horn of the spinal cord. The lateral system is accessed by spinothalamic pathways terminating in the ventral posterior thalamus.39 Neural relays forward the pain signals to the sensory cortex which prominently includes the insular cortex for intestinal sensations.40–42 Through the lateral system, information regarding the character, timing, and intensity of the stimuli is brought to conscious awareness.43,44 The medial system receives inputs from the dorsal horn to the intralaminar thalamus, in part via relays through the brainstem reticular formation. From the intralaminar thalamus, neural relays access the ACC, part of the limbic system, which mediates affective states. The ACC in humans has several divisions. The perigenual ACC appears to relate most closely to affective functions, including affective pain responses. Following surgical anterior cingulotomy, humans still feel pain “but it isn’t bothersome”.18 Self induced sad thoughts also activate the perigenual ACC.16,17 Pain affect may be assigned by the perigenual cingulate (the affective division of the ACC). Conversely, the caudal (posterior-dorsal) portion of the ACC (the cognitive division of the ACC) may serve more of a pure nociceptive function. Multiple studies of pain in humans have indicated the cognitive division of the ACC is activated proportional to pain intensity,20,43,45 and is involved in response selection.
The effects of stress on the brain are complex. Mental stress must first be interpreted by higher cortical centres. Ultimately, emotional, autonomic, and endocrine responses are coordinated by the locus coeruleus, amygdala, and hypothalamus.46,47 The amygdala is a medial temporal lobe region integral to conditioned fear, stress, and arousal.48,49 It is closely linked by neural processes to the hypothalamus and the locus coeruleus where CNS stress responses are integrated with endocrine and autonomic responses, respectively. The reduction of brain activation by amitriptyline during stress and visceral pain is consistent with a CNS effect of TCAs to inhibit stress responses.50,51 Located in the pons, the locus coeruleus is the major source of norepinephrine for the brain and spinal cord. Locus coeruleus neurones supply the brain and periaqueductal gray with norepinephrine to heighten arousal. This region also innervates the spinal intermediolateral neurones to activate sympathetic autonomic activity, and Barrington’s nucleus in the pons that activates sacral parasympathetic neurones to the rectum and bladder.52 TCAs are thought to reduce spontaneous nerve firing in the locus coeruleus due to increased inhibition by presynaptic α2 adrenergic receptors induced by blockade of norepinephrine reuptake.12,13,53 Reduced firing of locus coeruleus neurones is associated with diminished actions at its CNS targets.54 Reduced activation of the locus coeruleus would be expected to reduce pain related activation of its targets, including the anterior cingulate and other parts of the cortex. It has previously been demonstrated in rats that chronic TCA administration can reduce release of norepinephrine from the frontal cortex induced by foot shock or anxiogenic medication.50 This may be the mechanism by which perigenual anterior cingulate and parietal cortical activation during pain was selectively blunted during stress.
IBS is a condition exacerbated by psychosocial stressors and altered affective states, such as anxiety and depression. Gastrointestinal motility and pain sensitivity also appear to increase in IBS patients during stress.6,55,56 The reduction of activity in the perigenual anterior cingulate by amitriptyline during stress and pain may be critical to its benefits for IBS and other pain conditions. A reduction in brain response to the affective dimension of pain may be the mechanism of improvement. The affective dimension of pain may be determined by the anterior cingulate, given its neural connections to other affective areas such as the amygdala and intralaminar thalamus, and the role it plays in mood states. It is also possible that alteration in activity in the perigenual cingulate could reduce stress that is thought to exacerbate IBS pathophysiology and symptoms. Conversely, the insula is thought to be involved in visceral sensory perception, including pain. It is likely to serve as the sensory cortex for the gut, much like the post central gyrus of the parietal lobe (SI) serves for somatic sensation. In this study pain intensity during balloon distension was not altered by amitriptyline. The insula did not show any reduction in pain related activity during amitriptyline administration, consistent with lack of a direct effect of the drug on pain sensitivity. In this study, we assessed pain intensity but, unfortunately, not affect. Pain affect might be a domain that would be altered by a reduction in perigenual cingulate activation. Amitriptyline also inhibits serotonin transporters, leading to increased serotonin at the nerve ending. Serotonin is an important neurotransmitter in the enteric nervous system. Serotonin 3 receptor antagonists reduce pain and diarrhoea in IBS, while serotonin 4 receptor agonists reduce pain and constipation in IBS. It is conceivable that modulation of serotonin dynamics by amitriptyline in the periphery could impact IBS symptoms. However, in the current study, amitriptyline did not reduce rectal sensitivity, did not reduce brain activation in strictly sensory areas, and only had effects during mental stress. Accordingly, a CNS action of low dose amitriptyline for IBS appears most plausible.
In summary, amitriptyline reduces brain activation during rectal distension in IBS patients during mental stress, particularly in cognitive and affective cortical regions. There were no significant amitriptyline effects on subjective ratings of pain intensity or on activation of the insular cortex where visceral sensation is represented. Accordingly, we postulate that amitriptyline improves symptoms in IBS due to a CNS effect rather than a peripheral one. The mechanism of benefit is likely to be through a reduction in the affective component of pain or a reduction in stress related exacerbation of symptoms.
REFERENCES
Footnotes
-
This study was funded by NIH grant R21 DK57047.
-
Conflict of interest: None declared.