Article Text

Abstract
Background: Mouse models of colitis and cancer are indispensable for our understanding of the pathogenesis of these diseases. In the past, mice had to be sacrificed in order to analyse colitis activity and tumour development. We have developed a safe method for high resolution endoscopic monitoring of living mice.
Methods: Mice developing colitis or colonic tumours were anaesthetised using avertine and repeatedly examined by endoscopy. A novel miniendoscope (1.9 mm outer diameter), denoted Coloview, was introduced via the anus and the colon was carefully insufflated with an air pump before analysis of the colonic mucosa. An extra working channel allowed the introduction of biopsy forceps or injection needles as well as surface staining with methylene blue in order to visualise the surface of the crypts and the pit pattern architecture.
Results: Endoscopic pictures obtained were of high quality and allowed monitoring and grading of disease. Scoring of colitis activity as well as tumour size and growth was possible. In addition, pit pattern analysis using chromoendoscopy permitted discrimination between inflammatory and neoplastic changes. Biopsies yielded enough tissue for molecular and histopathological analyses.
Conclusions: In summary, chromoendoscopy in mice allows monitoring of the development of colitis and colon cancer with high resolution. Manipulations such as local injection of reagents or taking biopsies can be performed easily.
- DSS, dextran sodium sulphate
- AOM, azoxymethane
- FITC, fluorescein isothiocyanate
- TNF, tumour necrosis factor
- MEICS, murine endoscopic score of colitis severity
- ACF, aberrant crypt foci
- RT-PCR, reverse transcription-polymerase chain reaction
- endoscopy
- chromoendoscopy
- mouse
- cancer
- colitis
Statistics from Altmetric.com
- DSS, dextran sodium sulphate
- AOM, azoxymethane
- FITC, fluorescein isothiocyanate
- TNF, tumour necrosis factor
- MEICS, murine endoscopic score of colitis severity
- ACF, aberrant crypt foci
- RT-PCR, reverse transcription-polymerase chain reaction
Numerous mouse models of inflammatory bowel disease and colon cancer have been developed in the past (for comprehensive reviews see Wirtz and Neurath1 and Strober and colleagues2). These models substantially helped to understand the pathogenesis of these diseases but have also been used as model systems of mucosal immune responses investigating the interplay of different immune cells. In the past it has been impossible to investigate the mucosal surface or the development of tumours in a living animal over a long period of time, as animals had to be sacrificed in order to visualise the colonic mucosa. Thus to assess the state of the disease, only indirect parameters such as weight of the animal, food and water uptake, or the presence of blood in faeces could be used. In contrast, recurrent endoscopic examination of the colon is of the utmost importance for the diagnosis and staging of inflammatory bowel diseases and colon cancer in humans. Recent attempts to perform examinations with flexible or rigid endoscopes in mice were promising.3,4 However, to our knowledge no such attempt resulted in generation of high resolution pictures that would allow detailed analysis of the colon mucosa, necessary to examine all aspects of mucosal surface pathology in the colon.
In the present study, we have developed a high resolution chromoendoscopic system, allowing repeated monitoring and manipulation of colon pathogenesis in an individual mouse over a long period of time. As an experimental model we used azoxymethane plus dextran sodium sulphate (DSS) induced colitis and associated tumour formation, as previously described.5–7 We have developed endoscopic scores allowing the grading of colon pathology during routine mouse endoscopy. Finally, techniques to collect biopsies, inject reagents in vivo, or stain colonic crypts with methylene blue were developed, giving the investigator the tools to assess and manipulate disease progression in vivo.
METHODS
Animals
Specific pathogen free FVB/N mice (eight weeks old) were obtained from our central animal facility (ZVTE, University of Mainz, Germany). All animal experiments were performed in accordance with the guidelines of the institution. Colitis followed by colon tumours was induced as previously described.6 In brief, mice were injected intraperitoneally with a single dose (7.4 mg/kg) of the mutagenic agent azoxymethane (AOM), followed by three cycles of 3% DSS in drinking water for one week and normal drinking water for two weeks.
Endoscopic procedures
For continuous monitoring of colitis and tumorigenesis, a high resolution mouse video endoscopic system was developed. Mice were anaesthetised using intraperitoneal injection of avertine (Sigma Chemical Co, St Louis, Missouri, USA). The experimental endoscopy setup, denoted “Coloview system”, consisted of a miniature endoscope (scope 1.9 mm outer diameter), a xenon light source, a triple chip camera, and an air pump (all from Karl Storz, Tuttlingen, Germany) to achieve regulated inflation of the mouse colon. The endoscopic procedure was viewed on a colour monitor and digitally recorded on tape (DSR-20MDP; Sony, Cologne, Germany). This novel technique was combined with whole colon chromoendoscopic staining with methylene blue to visualise the crypt pattern and detect aberrant crypt foci in vivo. Therefore, the colon was flushed with 500 µl of a 1% solution of methylene blue using a syringe mounted to the Luer lock cones of the examination sheath of the endoscope. Tumour sampling in living mice was performed by taking biopsies using a flexible biopsy forceps with a diameter of 3 Fr. Biopsies were either immediately frozen in liquid nitrogen for cryosections, put into formalin for paraffin sections, or put into lysis buffer of the RNeasy micro kit (Qiagen, Hilden, Germany) for subsequent RNA isolation. In one experiment a needle (26 G) mounted on the tip of a small tube was introduced through the working sheath and 20 µl of an fluorescein isothiocyanate (FITC) solution were injected directly into the tumour.
Tumour scoring
Two scores were used. Tumours observed during endoscopy were counted to obtain the overall number of tumours. Furthermore, tumour sizes of all tumours in a given mouse were scored yielding the tumour score. Tumour sizes were graded as follows: grade 1 (very small but detectable tumour), grade 2 (tumour covering up to one eighth of the colonic circumference), grade 3 (tumour covering up to a quarter of the colonic circumference), grade 4 (tumour covering up to half of the colonic circumference), and grade 5 (tumour covering more than half of the colonic circumference).
Isolation of mRNA and reverse transcription-polymerase chain reaction (RT-PCR)
Total RNA was isolated from sonicated biopsies using the RNeasy micro kit (Qiagen) according to the manufacturer’s recommendations. The yield was usually 1–2 µg of RNA per biopsy. Reverse transcription into cDNA was performed using the Superscript II reverse transcriptase (Invitrogen, Karlsruhe, Germany) according to the manufacturer’s recommendations. PCR was performed using the following primers: murine β-actin, 5′-TGA CGG GGT CAC CCA CAC TGT GCC CAT CTA-3′ and 5′-CTA GAA GCA TTT GCG GTG GAC GAT GGA GGG-3′; and murine tumour necrosis factor α (TNF-α) 5′-AAC TGG CAG AAG AGG CAC TC-3′ and 5′-TTG GGC AGA TTG ACC TCA GC-3′. PCR products were analysed on 1% agarose gels.
Histological analysis of colon cross sections
Biopsies were removed from mice during endoscopy and immediately embedded in paraffin. Sections were made and stained with haematoxylin-eosin. The degree of dysplasia on microscopic cross sections of the colon was graded by an experienced pathologist (HAL).
Immunohistochemistry
Immunofluorescence was performed using the TSA Cy3 system (Perkin Elmer, Heidelberg, Germany) and a fluorescence microscope (Olympus, Melville, New York, USA) as described previously.8 In brief, cryosections were fixed in ice cold acetone for 10 minutes followed by sequential incubation with methanol, avidin/biotin (Vector Laboratories, Burlingame, California, USA), and protein blocking reagent (Dako, Wiesbaden, Germany) to eliminate unspecific staining. Slides were then incubated overnight with primary antibodies specific for TNF-α (Santa Cruz, California, USA). Subsequently, slides were incubated for 30 minutes at room temperature with a biotinylated secondary antibody (Dianova, Darmstadt, Germany). All samples were finally treated with streptavidin-horseradish peroxidase and stained with Tyramide (Cy3) according to the manufacturer’s instructions (Perkin Elmer). Before examination, nuclei were counterstained with Hoechst 3342 (Molecular Probes, Eugene, Ohio, USA).
RESULTS
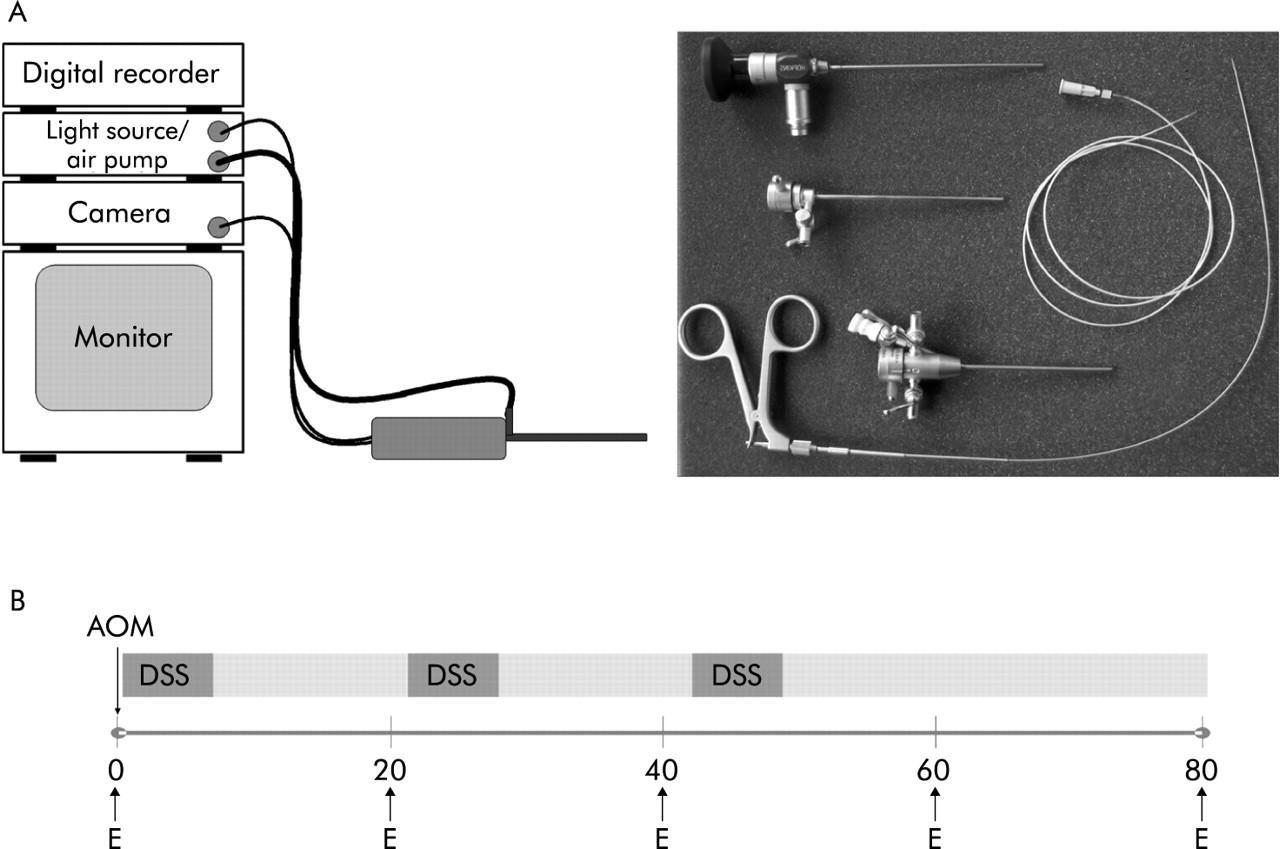
We developed a novel high resolution endoscopic system, denoted Coloview, consisting of a straightforward Hopkins telescope (1.9 mm diameter), a xenon cold light fountain combined with an air pump, allowing inflation of the colon, and a pal triple chip camera (fig 1A). The endoscopic procedure was monitored on a standard PAL colour monitor and recorded digitally on tape (Sony digital video recorder and cassettes). To endoscopically investigate colitis and colitis associated colon tumours, FVB/N mice were injected intraperitoneally with a single dose of the mutagenic agent AOM followed by 3 cycles of 3% DSS in drinking water for one week and normal drinking water for two weeks (fig 1B). Mice were endoscopically examined on days 0, 20, 40, 60, and 80, as indicated. On day 0, mice were healthy and showed a smooth, shiny, and thin (translucent) mucosal surface and normal blood vessel architecture (fig 2A). Staining of the colon with methylene blue revealed a regular crypt pattern.
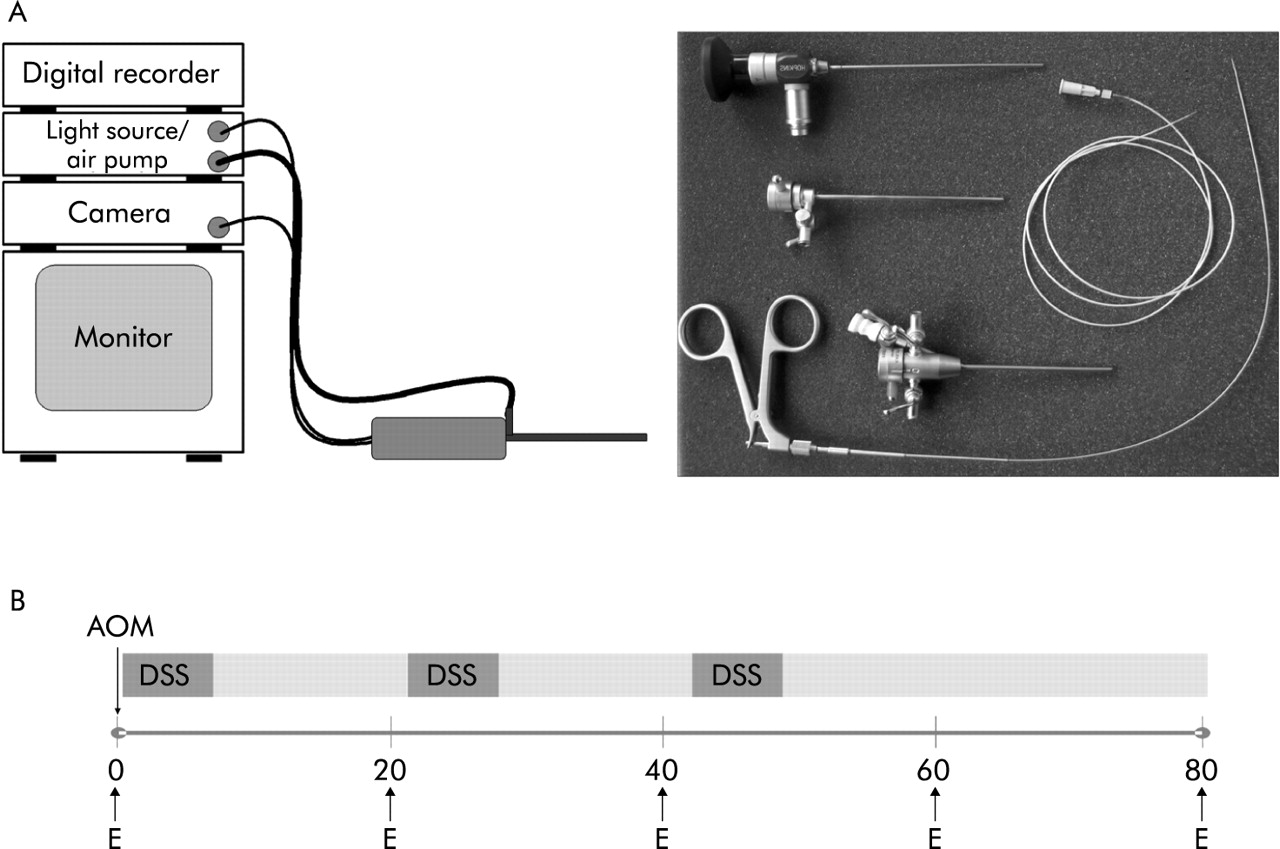
Experimental setup of the Coloview miniendoscopic system. (A) Schematic diagram of the endoscopic setup. Endoscopic tools used for mouse examinations: straightforward telescope, examination sheath, manipulation sheath, biopsy forceps, and injection tube. (B) Experimental procedure used to induce colon carcinogenesis in FVB mice. Mice were injected intraperitoneally with a single dose (7.4 mg/kg) of the mutagenic agent azoxymethane (AOM) followed by three cycles of dextran sodium sulphate (DSS) in drinking water for one week and normal drinking water for two weeks. E = endoscopic examination.

In vivo high resolution endoscopy and chromoendoscopy of mice treated with azoxymethane and dextran sodium sulphate. Mice were anaesthetised by intraperitoneal injection of avertine. The colon mucosa was stained with methylene blue to visualise the crypt pattern. (A) Representative endoscopic pictures showing the colon of a healthy mouse. Note the smooth and transparent mucosa, normal vascular pattern, and regular crypt pattern in the methylene blue stained colon. (B) Representative endoscopic pictures showing signs of severe inflammation. Note the close up pictures of bleeding mucosa, altered vascular pattern, transparent mucosa, and fibrin. (C) Endoscopic colitis score based on the observed signs of inflammation. The modified murine endoscopic index of colitis severity (MEICS) consisted of five parameters, as indicated. (D) Methylene blue staining of the colonic mucosa during endoscopy at day 20. Shown are representative pictures of chromoendoscopic signs of inflammation and early neoplasias (aberrant crypt foci (ACF)).
In contrast, mice examined on day 20 of the experiment showed marked endoscopic signs of mucosal inflammation (fig 2B). Accordingly, we observed thickening of the mucosa, bleeding, and sometimes a granular mucosa surface, traces of faeces, loss of blood vessel structure, and the presence of fibrin. Based on these endoscopic signs of inflammation, we developed a colitis score, the modified murine endoscopic score of colitis severity (MEICS), ranging from 0 (no signs of inflammation) to 15 (very severe colitis) (fig 2C). Staining of the mucosa with methylene blue demonstrated local mucosal erosions and multiple ulcers (fig 2D; left panels). In addition, multiple aberrant crypt foci (ACF) were observed that were undetectable in the absence of staining (fig 2D; right panels). These ACF lesions could be clearly differentiated from inflammatory changes, highlighting the use of methylene blue to detect such early lesions during tumorigenesis.
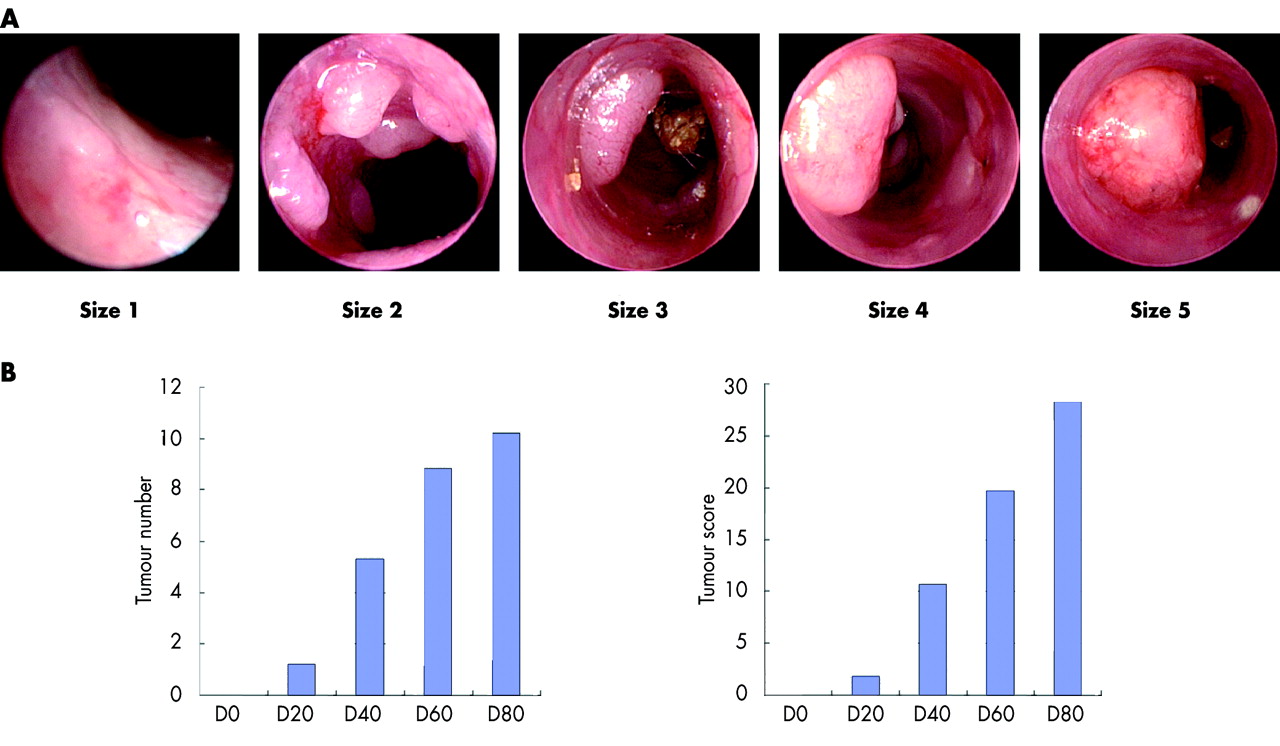
At approximately day 40 of the experiment, tumours became macroscopically visible during endoscopic examination, even in the absence of methylene blue aided chromoendoscopy. Tumours then grew continuously until the end of the experiment (fig 3A). In order to endoscopically grade tumour development, two novel scoring systems were developed: one representing only the number of tumours counted during endoscopy and a second score combining the number and sizes of tumours based on their circumference (see methods). To keep the endoscopic procedure short, such scoring was performed on analysis of previously recorded tapes. During the course of the experiment, overall tumour number continuously increased in AOM plus DSS treated wild-type mice, reaching an average of approximately 10 tumours per mouse between day 60 and day 80 of the experiment (fig 3B). Tumour score increased continuously until day 80.
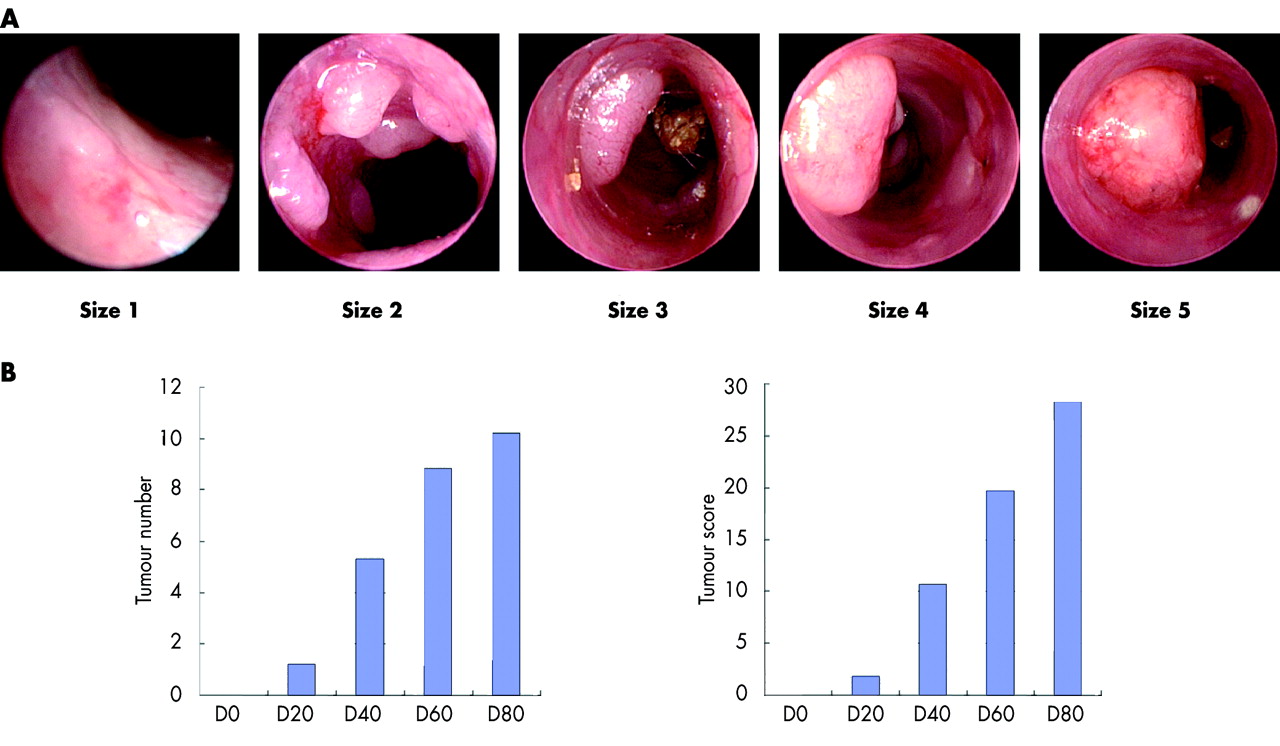
Endoscopic scoring of tumour development in mice. (A) Representative endoscopic pictures showing the development of colon tumours during the course of the experiment. The grading of tumour size was performed as indicated in materials and methods. (B) Number of lesions in each mouse was counted and compared during the course of the experiment (left panel). Alternatively, the size of each tumour was graded at the indicated time points and summed up for each mouse (right panel).
We have currently performed more than 500 endoscopic and chromoendoscopic examinations in mice, most of them with signs of severe colitis (n>200) and tumours (n>200). Endoscopic examinations were also performed in mice of different inbred strains (FVB/N, Balb/c, C57Bl6) and in immunocompromised mice (SCID, Rag1−/−). In addition, several models of colitis were investigated, including trinitrobenezene sulphonic acid or oxazolone induced colitis, and colitis induced by the adoptive transfer of CD62L+ cells into Rag1−/− mice. Mice usually tolerated the procedure very well and very few mice (less than 1%) died after endoscopy due to inability to recover from anaesthesia because of high disease activity or dramatic weight loss as a consequence thereof. However, given the low complication rate, even in mice with very advanced colitis and weight loss, endoscopy could still be considered safe. No differences in complication rates were noted between different mouse strains or colitis models. Finally, no perforations were noted on obtaining tumour biopsies.
In order to examine tumours without sacrificing the animal, biopsies were taken during endoscopy (fig 4A) and either snap frozen for immunofluorescence and molecular analyses or fixed in formalin for haematoxylin-eosin staining. Haematoxylin-eosin stains of tumour biopsies were most frequently scored as high grade intraepithelial neoplasias by our pathologist. To investigate whether the quality of tumour biopsies was sufficient for more sophisticated methods of analysis, we performed immunofluorescence staining of tumour biopsies for TNF-α. As shown in fig 4A (upper right panel), the tumour stroma stained positive for TNF-α, indicating that lamina propria cells express this cytokine in colitis associated colon tumorigenesis. Furthermore, we tested whether biopsies could be used for molecular biological analysis of gene activity. Therefore, RNA was isolated from biopsies and subjected to RT-PCR analysis. The presence of bands for the 28S and 18S rRNA, as shown in fig 4A (lower panels), indicates that the quality of RNA from tumour biopsies was sufficient for RT-PCR analysis. Consistently, RT-PCR using gene specific primers demonstrated abundant expression of TNF-α in all tumour biopsies. β-Actin was used as a control. Thus endoscopic biopsies yield sufficient tissue for a wide range of experimental methods. Finally, we examined whether our endoscopic system could be used to locally inject reagents. Therefore, we mounted a 26 G needle on the tip of a small tube connected to a syringe. The needle was endoscopically introduced into a tumour and FITC was carefully injected. As shown in fig 4B, only minimal bleeding was observed after removal of the needle. The tumour was then removed from the mouse and cryosections of this tumour were analysed by immunofluorescence. As shown in fig 2D, FITC was located in the entire tumour mass, implying that this system can be used to locally administer reagents specifically into individual tumours.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Molecular investigation and manipulation of tumour development in mice. (A) Biopsy sampling (upper left panel) of a tumour during routine endoscopic monitoring of azoxymethane/dextran sodium sulphate treated animals. Tumour biopsies were snap frozen in liquid nitrogen and cut for staining. Subsequent haematoxylin-eosin staining (upper middle panel) demonstrated high grade intraepithelial neoplasias. Immunohistochemistry for tumour necrosis factor α (TNF-α) (upper right panel) of cross sections was performed using the TSA Cy3 system. Cryosections were fixed in acetone. Slides were then incubated with primary antibodies specific for TNF-α. Before examination, nuclei were counterstained with Hoechst 3342. Lower left panel: gel electrophoretic picture showing the high quality of RNA extracted from five tumour biopsies. Tumours typically yielded 1–2 µg RNA per biopsy. Lower right panel: reverse transcription-polymerase chain reaction analysis for TNF-α expressed in tumour biopsies. β-Actin served as a control. (B) Injection of fluorescein isothiocyanate (FITC) into a tumour during endoscopy. A needle mounted onto a thin tube was introduced through the instrument channel of the endoscope and FITC was slowly injected. Tumour samples were then analysed by immunofluorescence. One representative picture of a tumour injected with 20 µl of an FITC solution and a control tumour not injected is shown.
In summary, we have developed a high resolution endoscopic system allowing the investigator to monitor pathological changes on the mucosal surface of the colon, to obtain sample material without sacrificing the animal, and finally to deliver reagents locally. This novel method may thus be of crucial importance in monitoring the pathogenesis of colonic diseases in mice.
DISCUSSION
In this study, we have characterised a novel system for high resolution endoscopic monitoring of the mouse colon. This method allows fascinating new insights into the pathogenesis of murine colitis and colon cancer by monitoring and scoring of colitis activity and colon cancer. Furthermore, mouse colonoscopy allows colonic biopsies to be obtained, and local injections into single tumours can be performed. As the investigator can analyse the success of the experiments early on and can monitor disease activity and extent in vivo, this approach may also help to limit the costs and number of mice per experiment.
Murine experimental models provide important tools to investigate the pathogenesis and therapies for chronic intestinal inflammation and colon cancer in humans. The main advantages of mouse models are relatively easy breeding and the possibility of using syngeneic mouse strains. Furthermore, mouse lines transgenic or deficient for specific proteins provide important tools to investigate the role of these factors in colitis and colon cancer in vivo. However, an obstacle in the use of mice for investigating colon pathogenesis has always been examination of the colon in living mice. Endoscopy of the colon is the most important examination for diagnosis and grading of colonic diseases in humans. In the past, several attempts were made to perform endoscopy in mice.3,4 However, the small diameter of the mouse colon made it difficult to obtain pictures with high quality sufficient to endoscopically grade disease activity. Our endoscopic setup produced high resolution pictures of publication quality, allowing us to score the degree of colitis and tumour development. Endoscopy was found to be safe, reproducible, and fast, and usually required no longer than two minutes.
Using methylene blue to stain the colonic crypts it was possible to detect lesions that were not visible during standard colonoscopy before staining. Furthermore, inflammatory lesions could be easily differentiated from preneoplastic ACFs. Finally, chromoendoscopy allowed us to classify ACFs with regard to their pit pattern according to the Kudo classification.9 Therefore, consistent with previous studies in humans,10–12 chromoendoscopy emerges as a useful approach to discriminate between neoplastic and inflammatory changes in the murine colon.
In summary, chromoendoscopy in mice is a safe procedure allowing the investigator to repeatedly monitor colitis activity and progression of colon cancer and obtain pictures with high resolution. This technique may be of crucial importance in performing long term studies in mice with chronic colitis and colitis associated colon cancer and in helping the investigator to determine the success of the experiment at an early stage. Furthermore, biopsies obtained during endoscopy provide a unique opportunity of analysing colonic inflammation and carcinogenesis over time by modern immunological and molecular methods.
REFERENCES
Footnotes
-
Conflict of interest: None declared.