Article Text

Abstract
Background and aim: It is not known why some reflux episodes evoke symptoms and others do not. We investigated the determinants of perception of gastro-oesophageal reflux.
Methods: In 32 patients with symptoms suggestive of gastro-oesophageal reflux, 24 hour ambulatory pH and impedance monitoring was performed after cessation of acid suppressive therapy. In the 20 patients who had at least one symptomatic reflux episode, characteristics of symptomatic and asymptomatic reflux episodes were compared.
Results: A total of 1807 reflux episodes were detected, 203 of which were symptomatic. Compared with asymptomatic episodes, symptomatic episodes were associated with a larger pH drop (p<0.001), lower nadir pH (p<0.05), and higher proximal extent (p<0.005). Symptomatic reflux episodes had a longer volume and acid clearance time (p<0.05 and p<0.002). Symptomatic episodes were preceded by a higher oesophageal cumulative acid exposure time (p<0.05). The proximal extent of episodes preceding regurgitation was larger than those preceding heartburn; 14.8% of the symptomatic reflux episodes were weakly acidic. In total, 426 pure gas reflux episodes occurred, of which 12 were symptomatic. Symptomatic pure gas reflux was more frequently accompanied by a pH drop than asymptomatic gas reflux (p<0.05).
Conclusions: Heartburn and regurgitation are more likely to be evoked when the pH drop is large, proximal extent of the refluxate is high, and volume and acid clearance is delayed. Sensitisation of the oesophagus occurs by preceding acid exposure. Weakly acidic reflux is responsible for only a minority of symptoms in patients off therapy. Pure gas reflux associated with a pH drop (“acid vapour”) can be perceived as heartburn and regurgitation.
- GORD, gastro-oesophageal reflux disease
- LOS, lower oesophageal sphincter
- oesophagus
- pH monitoring
- gastro-oesophageal reflux
- impedance
- heartburn
Statistics from Altmetric.com
Symptoms suggestive of gastro-oesophageal reflux disease (GORD) are a common reason for consultation. In the past decades the relationships between oesophageal acid exposure and reflux symptoms have been explored extensively, in particular with 24 hour oesophageal pH monitoring. However, several questions concerning the generation of reflux symptoms have remained unanswered. For instance, it is not clear why some patients suffer from symptoms such as heartburn and regurgitation whereas others, with an apparently similar reflux profile, do not.1 Likewise, why do some reflux episodes evoke symptoms while other reflux episodes in the same patient do not? Studies using multiple pH sensors at different positions in the oesophagus have shown that symptomatic reflux episodes have a more proximal extent, a longer duration, and a lower pH compared with reflux episodes that remain asymptomatic.2–4 Furthermore, studies on the effect of acid secretion inhibiting therapy on oesophageal sensitivity to acid instillation suggested that exposure of the oesophagus to acid leads to hypersensitivity for subsequent reflux episodes.5,6 While these studies have increased our understanding of perception of acid gastro-oesophageal reflux (that is, of episodes associated with a fall in pH below 4), the techniques used in these studies did not allow assessment of symptoms induced by non-acid refluxate.7
Recently, multiple intraluminal impedance was introduced as a new and reproducible technique to monitor gastro-oesophageal reflux.8,9 With this technique detection of gastro-oesophageal reflux is irrespective of acidity, so that reflux with a nadir pH between 4 and 7 (weakly acidic reflux) and with a nadir pH above 7 (alkaline reflux) can also be detected.10 Studies using impedance monitoring have shown that, in patients who are not on acid suppressant therapy, approximately one third of all reflux episodes are weakly acidic.11 It is not clear to what extent reflux of material with a pH >4 leads to symptoms. The aim of this study was therefore to identify factors, acidic, weakly acidic, and weakly alkaline, that are important in the elicitation of reflux symptoms.
METHODS
Subjects
In 32 patients with typical reflux symptoms (17 males, 15 females; age 27–65 years (median 53)), ambulatory 24 hour combined impedance and pH monitoring was performed. The 20 studies in which at least one reflux related symptom episode occurred were selected for further analysis. Written informed consent was obtained from all subjects and the protocol was approved by the medical ethics committee of the University Medical Centre Utrecht.
Study protocol
The use of gastric acid inhibitory drugs and drugs that might influence gastrointestinal motility was discontinued five days before the study. Stationary oesophageal manometry was performed to determine the distance from the nostrils to the lower oesophageal sphincter (LOS). After this, impedance and the pH catheter were introduced transnasally and positioned based on the manometric findings (see below).
Patients were instructed to press the event marker button on the pH datalogger whenever they experienced a symptom suggestive of reflux. The nature and time of onset of their symptoms was written down on a specially designed diary. Patients were instructed to distinguish between regurgitation and heartburn. Regurgitation was defined as the sensation of effortless return of gastric or oesophageal fluid into the mouth or throat, and heartburn was defined as a burning retrosternal sensation. Furthermore, patients were instructed to consume three meals and two beverages with snacks at fixed times during the 24 hour measurement period. The period spend in the supine position was also noted in the diary.
Oesophageal impedance and pH monitoring
For intraluminal impedance monitoring a seven channel impedance catheter was used (Aachen University of Technology, FEMU, Aachen, Germany). This catheter (outer diameter 2.3 mm) enabled recording from seven segments, each recording segment being 2 cm long. The recording segments were located at 0–2, 2–4, 4–6, 8–10, 10–12, 14–16, and 17–19 above the upper border of the manometrically localised LOS. Impedance signals were stored in a portable digital system (Aachen University of Technology, FEMU, Aachen, Germany) using a sample frequency of 200 Hz.12 Intraluminal pH monitoring was performed with a glass pH electrode (Ingold AG, Urdorf, Switzerland) and data were stored in a separate digital datalogger (Orion, MMS, Enschede, the Netherlands) using a sampling frequency of 2 Hz. The pH glass catheter was positioned 5 cm above the upper border of the LOS. Using a cable that connected the pH datalogger with the impedance datalogger the pH signals were also stored on the impedance datalogger enabling synchronisation.
Data analysis
Analysis of the tracings was performed independently by two experienced investigators. Thereafter, the two investigators conjointly analysed the reflux episodes that were not recognised by both of them. A consensus decision was made on each of these episodes. Signals recorded during consumption of meals and beverages were not taken into account during analysis of the data.
In the analysis of the impedance tracings, gas reflux was defined as a rapid (>3000 Ω/s) and pronounced retrograde moving increase in impedance in at least two consecutive impedance sites.13 Liquid reflux was defined as a fall in impedance of ⩾40% of baseline impedance that moved in a retrograde direction in the two distal impedance sites.11 Mixed liquid-gas reflux was defined as gas reflux occurring during or immediately before liquid reflux. In the subsequent analysis, mixed reflux was considered as liquid reflux with a gas reflux component, and mixed reflux episodes were combined with pure liquid reflux episodes. Gas reflux episodes were analysed separately. For all reflux episodes, the proximal extent of both the gas and liquid component was noted as well as the time needed to reach this proximal sensor, and the ascending velocity of the components of the refluxate was calculated. Clearance time of the volume of the refluxate was defined as the time in seconds from the 40% drop in impedance until impedance recovered to above this point again, as measured in the impedance segment at the level of the tip of the pH probe.14
For each liquid, gas or mixed reflux episode, as observed in the impedance tracings, the change in pH and the nadir pH during the reflux episode was noted. Reflux episodes that caused a change in pH of less than 0.5 units were not unambiguously distinguishable from baseline noise, and these were scored as a pH drop of 0. Reflux episodes were classified as acid when the pH dropped below 4; reflux episodes were classified as weakly acidic when nadir pH was between 7 and 4.10 Reflux was classified as weakly alkaline reflux when the nadir pH was above 7. For reflux episodes with a nadir pH of less than 4, the acid clearance time was measured, defined as the time during which pH was below 4.15
In order to assess the potential sensitising effect of preceding oesophageal acid exposure on symptom perception, the total time with pH below 4 was measured in the 15, 30, 45, 60, 75, and 90 minute time segment preceding the onset of each reflux episode.16
Reflux episodes were considered symptomatic if a symptom occurred within the two minute time window starting at the onset of the reflux episode.17 The time between the onset of the reflux episode and the occurrence of the symptom was measured. Only the symptoms heartburn and regurgitation were evaluated and other symptoms such as chest pain, belching, coughing, and hoarseness were not taken into account.
Statistical analysis and presentation of data
Analysis was performed on a per subject basis. Comparison of symptomatic and asymptomatic reflux episodes within subjects was performed using the Wilcoxon signed rank test. Comparison of the properties of reflux episodes preceding heartburn and regurgitation was performed using the Wilcoxon rank sum test. Comparisons of proportions were calculated using the χ2 test. Relationships between parameters were expressed using the Spearman correlation coefficient. Differences were considered statistically significant when p⩽0.05. Throughout the manuscript data are presented as median (interquartile range).
RESULTS
In the 20 24 hour impedance recordings, median percentage of time with pH <4 was 7.9 (5.3–11.0)%; three patients had physiological acid exposure (time pH <4 less than 6.0%). A total of 1807 reflux episodes were detected, 728 of which were classified as pure liquid reflux, 426 as pure gas, and 653 as mixed gas-liquid. The majority of reflux episodes occurred while patients were in the upright position (1628 upright v 179 supine). Acid clearance time of the acid reflux events was significantly longer than the volume clearance time of these reflux events (50.0 (24.8–62.8) v 12.3 (10.1–15.3) seconds; p<0.001). A total of 301 symptoms were reported. Of these, 203 episodes were associated with a reflux episode (67.4 %), ranging from 3 to 26 in individual patients. There was no relationship between the number of symptoms reported by individual patients and their acid exposure time (r = 0.136, p = 0.5).
Upright liquid reflux
In patients in the upright position, 1231 reflux episodes with a liquid component (pure liquid and mixed gas-liquid) occurred. Of these, 189 reflux episodes were associated with a symptom and 1042 were not. Median time interval between the onset of a reflux episode and the onset of the associated symptom was 14.0 (9–30.5) seconds.
Symptomatic liquid reflux episodes were significantly more often acidic (nadir pH<4) than asymptomatic reflux episodes and were more often accompanied by a pH fall of more than 0.5 units or 1.0 unit (table 1). A gaseous component in the liquid refluxate (mixed gas-liquid reflux) was present as frequently in asymptomatic as in symptomatic reflux episodes.
Characteristics of liquid reflux episodes
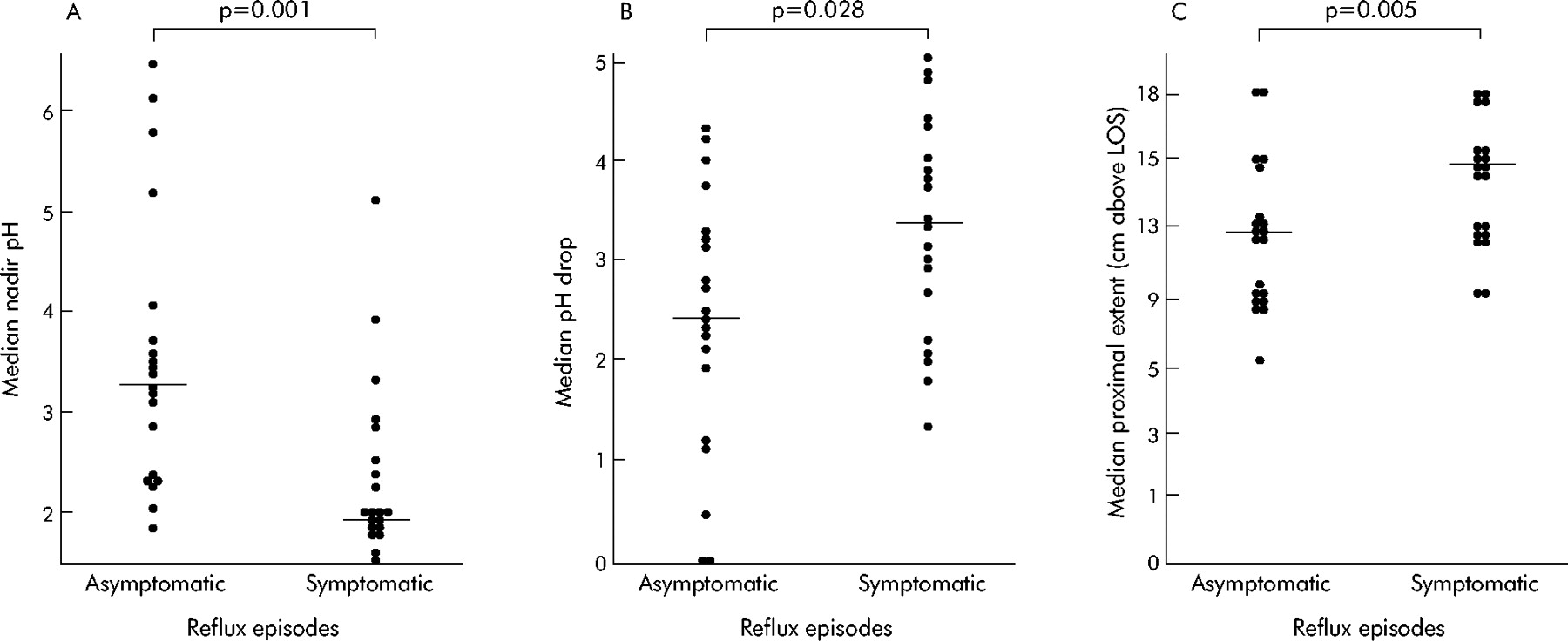
As shown in fig 1, median nadir pH was significantly lower and the median pH drop was significantly larger with symptomatic than with asymptomatic reflux episodes, and symptomatic reflux episodes had a significantly higher proximal extent. The ascending velocity of the liquid reflux component was not different between symptomatic and asymptomatic reflux episodes. Median acid clearance time (recovery of pH to 4) as well as volume clearance time (impedance recovery) were significantly longer with symptomatic than with asymptomatic reflux episodes (fig 2).

Characteristics of asymptomatic and symptomatic liquid reflux episodes in the upright position in 20 patients with gastro-oesophageal reflux disease. (A) Median nadir pH. (B) Median pH drop. (C) Median extent of the reflux episodes. Horizontal lines indicate group medians. Comparisons were performed using the Wilcoxon signed rank test. LOS, lower oesophageal sphincter.

Acid (A) and volume (B) clearance times (medians per patient) of asymptomatic and symptomatic liquid reflux episodes.
Symptomatic reflux episodes were preceded by a significantly higher oesophageal cumulative acid exposure time compared with asymptomatic reflux episodes (fig 3). The difference in preceding oesophageal acid exposure was apparent for time windows with a length of up to 75 minutes.

{kind=link}
{kind=link}
{kind=link}
Cumulative acid exposure in the time windows 15–90 minutes’ duration preceding asymptomatic and symptomatic reflux episodes in the upright position. *p<0.05 (Wilcoxon signed rank test).
Statistically significant but weak relationships were found between the extent of the liquid component of the refluxate and the drop in pH (r = −0.330, p<0.0001), nadir pH (r = 0.333, p<0.0001), and acid clearance time (−0.108, r = 0.002). Acid clearance time did not correlate with pH drop (r = 0.04, NS) but correlated weakly with nadir pH (r = −0.215, p<0.0001) and volume clearance (r = 0.127, p<0.0001).
Upright gas reflux
A total of 397 episodes of pure gas reflux (belches) were identified, 12 of which were symptomatic. These 12 symptomatic gas reflux episodes without a liquid component were found in seven different subjects. Comparison of asymptomatic and symptomatic gas reflux episodes in these seven subjects showed that symptomatic gas reflux episodes were more frequently accompanied by a detectable pH drop (>0.5 unit) than asymptomatic reflux episodes (100 (67–100) v 63 (21–63)%; p = 0.028). A fall in pH of more than 1.0 unit was also more frequently encountered in symptomatic pure gas reflux episodes than in asymptomatic gas reflux episodes (100 (33–100) v 33 (15–47)%; p = 0.028). The proportion of reflux episodes that were accompanied by a drop in pH below 4 was not higher in symptomatic than in asymptomatic reflux episodes (33 (0–100)% v 13 (0–41)%; p = 0.22). The majority of gas reflux episodes (87.6%) reached the most proximal impedance segment. Symptomatic gas reflux episodes were associated with a larger drop in pH and a lower nadir pH than asymptomatic gas reflux episodes (table 2). No differences in ascending velocity of the gaseous refluxate or acid clearance were observed between asymptomatic and symptomatic reflux episodes (table 2).
Characteristics of pure gas reflux episodes
Supine reflux
Of the 1381 reflux episodes with a liquid component, only 150 occurred while patients were in the supine position. Both volume and acid clearance of the supine reflux episodes were significantly longer than those of the upright episodes (18 v 14 seconds (p<0.004) and 77 v 48 seconds (p<0.015)). Only two of the 150 liquid reflux episodes in the supine position were followed by a symptom in the two minute time window after the onset of the reflux episode. Both of these symptomatic reflux episodes were acidic (nadir pH <4) whereas 91 (60.7%) of the 148 asymptomatic liquid reflux episodes were acidic. In the supine position, only 29 pure gas reflux episodes occurred, versus 397 in the upright position.
Heartburn versus regurgitation
The 203 symptomatic reflux episodes consisted of 166 episodes of heartburn and 37 episodes of regurgitation. Thirteen patients suffered from both symptoms, one patient suffered from regurgitation only, and six suffered from heartburn only during the measurement period. Table 3 shows the results of comparison of the characteristics of the reflux associated with these two types of symptoms. Reflux episodes inducing regurgitation had a significantly higher proximal extent of the liquid component than episodes inducing heartburn (table 3). Also, a gaseous component was more often present in reflux episodes preceding regurgitation than in those preceding heartburn (68 v 40%; p = 0.003). Other characteristics such as ascending velocity, size of the pH drop, nadir pH, and acid and volume clearance times were not significantly different between these two symptoms.
Characteristics of heartburn and regurgitation
DISCUSSION
The relation between gastro-oesophageal reflux episodes and the conscious perception thereof is complex and despite many studies the mechanisms responsible for the development of reflux symptoms are incompletely understood. This is the first study in which impedance technology was used to investigate the determinants of symptomatic and asymptomatic reflux. Application of this technique made it possible to investigate the role of weakly acidic reflux and gas reflux in symptom generation.
Ambulatory pH studies have shown that the perception of acid reflux episodes (nadir pH <4) is dependent on the proximal extent of the refluxate, nadir pH reached, and the magnitude of the pH drop.2–4 Using impedance monitoring, we were able to show that the same factors are important for symptom generation by both acid and weakly acidic reflux and even by gas reflux. The weak correlations between the above mentioned factors indicate that they are largely independent. Determinants of reflux symptoms identified in this study constitute therapeutic targets, and reduction of acidity of the refluxate with a proton pump inhibitor or reduction of the proximal extent of the refluxate with endoscopic therapy can significantly reduce symptoms.18 Impedance monitoring also made it possible to show that not only acid clearance times but also volume clearance times are significantly longer in symptomatic reflux episodes. Previously, the importance of the volume of the refluxate in symptom generation had been inferred from indirect measures such as proximal extent and acid clearance times but it had never been shown before that symptomatic reflux episodes actually have longer volume clearance times.19 It has to be pointed out however that volume clearance times also depend on the effectiveness of oesophageal peristalsis. The fact that most symptoms occurred relatively shortly after a reflux episode (median 14 seconds) also suggests that the time that acid is present in the oesophagus is less important for the generation of symptoms than the volume and protonic content of the refluxed material.
Acid clearance time was significantly longer than volume clearance time. This confirms the concept that clearance in the oesophagus starts with peristalsis removing most of the refluxed volume and is followed by acid neutralisation by swallowed saliva.15
In a previous study using multiple pH sensors we found that the ascending velocity of the refluxate was higher in healthy volunteers than in GORD patients, suggesting a role for this parameter in the disease, but in this study the ascending velocity of the refluxate was found not to be a determinant of reflux perception.20
The characteristics of reflux episodes not only appear to determine whether or not a reflux episode is perceived but also the nature of the sensation. In particular, the proximal extent of reflux episodes preceding regurgitation was higher than the proximal extent of reflux episodes preceding heartburn. Other parameters such as nadir pH and pH drop were not significantly different between heartburn and regurgitation.
The vast majority (85.2%) of the liquid reflux related symptoms occurred after an acid reflux episode (pH<4) and only 14.8% were associated with weakly acidic reflux (pH between 4 and 7). This finding and the observation that the magnitude of the pH drop and nadir pH are important for symptom generation indicate that weakly acidic reflux is not a very important cause of typical reflux symptoms in patients who do not take acid suppressive drugs. Performing symptom association analysis with and without inclusion of weakly acidic reflux episodes in a larger group of patients can determine whether or not a subgroup of patients exists in whom weakly acidic reflux causes typical reflux symptoms. A larger contribution of weakly acidic reflux and weakly alkaline reflux is more likely to occur in patients with reflux symptoms after gastrectomy. For evaluation of symptoms of chronic cough and acid suppression resistant symptoms, it has already been shown that the combination of impedance and pH monitoring is more useful than pH monitoring alone.7,21 Impedance measurements also provide information about the proximal extent of reflux episodes, an important factor in symptom generation which is not provided by routine pH-metry.
The results of several studies suggest that the sensitivity of the oesophagus for acid is dependent on the preceding acid exposure. Various studies showed that oesophageal sensitivity, defined as the inverse of time to onset of pain after acid infusion, decreases after acid suppression with cimetidine or famotidine.5,22,23 Furthermore, after a 30 day course of omeprazole 60 mg there was a 35% reduction in intensity scores during an acid perfusion test.6 Conversely, a study in healthy volunteers showed an increase in oesophageal perception of acid after preceding perfusion of the oesophagus with acid.24 These observations prompted the hypothesis that oesophageal acid exposure leads to sensitisation for subsequent reflux episodes. In other words, the chance that a reflux episode is perceived would be dependent on acid exposure during the preceding period.16 Some evidence for this phenomenon was provided by a study by Beedassy et al in which time periods preceding symptomatic and asymptomatic reflux episodes were compared.25 However, in Beedassy’s study, reflux episodes recorded from different subjects were pooled, which can yield misleading results, as patients with higher oesophageal acid exposure times are more likely to have more symptomatic reflux episodes. Comparison of symptomatic and asymptomatic reflux episodes in a per subject analysis is therefore more appropriate than pooled data analysis. The results of our analysis indicate that acid exposure in the 75 minute period preceding a reflux episode is a determinant of whether or not a subsequent reflux episode will be perceived as a symptom.
Surprisingly, some reflux symptom episodes (heartburn, regurgitation) were induced by pure gas reflux. This is the first study to report that symptoms, other than belching, can be elicited by gastro-oesophageal reflux without a liquid component. Oesophageal distension by the refluxed gas might play a role. It has been reported that balloon distension of the oesophagus may induce symptoms of heartburn and chest pain.26,27 Another possibility is that very small droplets of acid (“acid vapour”) accompany the refluxing gas. Many of the pure gas reflux episodes were accompanied by a drop in pH. This phenomenon was previously observed in studies using impedance measurements and high frequency intraluminal ultrasound of the oesophagus.13,28,29 Our finding that symptomatic gas reflux episodes are accompanied by a significantly larger pH drop compared with asymptomatic gas reflux episodes supports the concept that minute amounts of acid can induce a sensation of heartburn.30 Theoretically, a third explanation could be that the fluid component of the refluxate is not detected by the impedance technique because the liquid volume is too small. However, validation studies have shown that the impedance technique is very sensitive for the detection of even small volumes of liquid materials and therefore this explanation does not seem very likely.8,31
Reflux episodes in the supine position occurred much less frequently but lasted significantly longer than upright reflux episodes (both acid and volume clearance time were longer). Reduced saliva production during sleep and the absence of primary peristalsis are likely to be the cause.32 Notwithstanding the prolonged duration of reflux episodes during the night, nocturnal heartburn was very rare in our study, with only two symptoms observed. Arousal seems to be a more frequent complaint caused by nocturnal reflux.32
It is important to realise that although differences between symptomatic and asymptomatic reflux episodes were found in this study, considerable overlap in the properties of symptomatic and asymptomatic reflux episodes is present. Hence, in individual patients, even proximally extending reflux episodes with a longlasting large pH drop may go unnoticed. It is therefore not possible to establish thresholds for the duration, pH drop, or proximal extent above which reflux episodes would consistently provoke symptoms. As noted previously, while we showed that, on average, weakly acidic reflux does not play a major role in symptom elicitation, it can be important in a subgroup of patients.
In conclusion, this study used impedance technology to show that whether or not a reflux episode is perceived as a symptom is determined by the proximal extent of the refluxate, nadir pH, magnitude of the drop in pH, as well as by volume and acid clearance time. Reflux episodes inducing regurgitation have a more proximal extent than episodes inducing heartburn. Furthermore, this study has provided further evidence of sensitisation of the oesophagus by preceding acid exposure. Weakly acidic reflux (pH between 4 and 7) is responsible for a minority of symptoms only. Acidic gas reflux without a liquid component or “acid vapour” can be perceived as heartburn and regurgitation.
Acknowledgments
A J Bredenoord received a clinical research trainee grant from Janssen Pharmaceuticals, Tilburg, the Netherlands.
REFERENCES
Footnotes
-
Published online first 24 August 2005
-
Conflict of interest: None declared.
Linked Articles
- Digest