Article Text

Abstract
Objective: To investigate the diagnostic potential of endoscopic tri-modal imaging and the relative contribution of each imaging modality (i.e. high-resolution endoscopy (HRE), autofluorescence imaging (AFI) and narrow-band imaging (NBI)) for the detection of early neoplasia in Barrett’s oesophagus.
Design: Prospective multi-centre study.
Setting: Tertiary referral centres.
Patients: 84 Patients with Barrett’s oesophagus.
Interventions: The Barrett’s oesophagus was inspected with HRE followed by AFI. All lesions detected with HRE and/or AFI were subsequently inspected in detail by NBI for the presence of abnormal mucosal and/or microvascular patterns. Biopsies were obtained from all suspicious lesions for blinded histopathological assessment followed by random biopsies.
Main outcome measures: (1) Number of patients with early neoplasia diagnosed by HRE and AFI; (2) number of lesions with early neoplasia detected with HRE and AFI; and (3) reduction of false positive AFI findings after NBI.
Results: Per patient analysis: AFI identified all 16 patients with early neoplasia identified with HRE and detected an additional 11 patients with early neoplasia that were not identified with HRE. In three patients no abnormalities were seen but random biopsies revealed HGIN. After HRE inspection, AFI detected an additional 102 lesions; 19 contained HGIN/EC (false positive rate of AFI after HRE: 81%). Detailed inspection with NBI reduced this false positive rate to 26%.
Conclusions: In this international multi-centre study, the addition of AFI to HRE increased the detection of both the number of patients and the number of lesions with early neoplasia in patients with Barrett’s oesophagus. The false positive rate of AFI was reduced after detailed inspection with NBI.
Statistics from Altmetric.com
Oesophageal adenocarcinoma has the fastest rising incidence in the western world and has a known precursor lesion: Barrett’s oesophagus. Oesophageal adenocarcinoma has a poor prognosis when diagnosed at an advanced stage.1–6 Endoscopic surveillance of patients with Barrett’s oesophagus is therefore recommended to detect neoplastic lesions at an early and curable stage.7 8 Early neoplastic lesions (i.e. high-grade intraepithelial neoplasia (HGIN) or early cancer (EC)), however, are difficult to detect with standard endoscopic techniques and may easily be missed by random biopsies.
In recent years several new endoscopic imaging techniques have been developed which may improve the detection of early neoplastic lesions in Barrett’s oesophagus. Autofluorescence imaging (AFI) is a technique that can potentially differentiate tissue types based on their differences in fluorescence emission. When tissues are exposed to short wavelength light endogenous biological substances (i.e. fluorophores) are excited, leading to the emission of fluorescent light of a longer wavelength (i.e. autofluorescence). Normal and neoplastic tissue have different autofluorescence characteristics that may enable their distinction.9 10 Until recently the use of autofluorescence diagnosis was restricted to either autofluorescence spectroscopy or autofluorescence endoscopy using fibre-optic endoscopes, which provide poor white-light images compared with currently available high-resolution video-endoscopes (HRE).11 We have recently reported on the use of a video-autofluorescence imaging (AFI) system that incorporates HRE for high-quality white-light images and a real-time video-autofluorescence modality. In an uncontrolled feasibility study, AFI led to the detection of a significant number of patients with HGIN/EC who showed no visible abnormalities on HRE. AFI, however, was also associated with a false positive rate of 51%.12
Narrow band imaging (NBI) is novel imaging technique that enhances the visualisation of superficial mucosal structures. In NBI, the band-pass ranges of the green and blue components of the excitation light are narrowed and the relative intensity of the blue spectrum is increased. This improves the visualisation of mucosal structures and further enhances mucosal blood vessels because the blue light excitation is highly absorbed by haemoglobin.13 14 Several reports have shown that NBI may improve the detection of mucosal and vascular patterns in Barrett’s oesophagus.15–17 In a recent study, we found that regular mucosal and vascular patterns were associated with non-dysplastic Barrett’s oesophagus, whereas irregular mucosal and vascular patterns as well as abnormal blood vessels were associated with early neoplasia.18
In a subsequent proof-of-principle study, we demonstrated that HRE and AFI can serve as “red-flag” techniques to identify suspicious lesions followed by NBI for confirmation of suspicious surface structures to reduce the false positive rate.19 This set-up, however, requires the use of two different endoscopes and endoscopy units. Recently, a new endoscopic system has become available that incorporates HRE, AFI and NBI (with an optical zoom capability) in one system: Endoscopic tri-modal imaging (ETMI). The AFI mode of this system has a different algorithm compared to the previous AFI prototype, which consisted of total autofluorescence, red reflectance and green reflectance. The new algorithm incorporates total autofluorescence after blue light excitation and green reflectance.
The aim of this study was to assess the feasibility of using ETMI for the detection of HGIN/EC in Barrett’s oesophagus in a multi-centre setting and to study the relative contributions of each imaging modality (i.e. HRE, AFI and NBI).
METHODS
Setting
This study was performed in four tertiary referral centres for the diagnosis and treatment of patients with early neoplasia in Barrett’s oesophagus: Academic Medical Center, Amsterdam, Netherlands; Mayo Clinic Jacksonville, Florida, US; Mayo Clinic Rochester, Minnesota, US, and Queens Medical Centre, Nottingham, UK. All procedures were performed by five expert endoscopists in Barrett’s oesophagus with extensive experience in advanced imaging techniques (JB, KR, MW, HW and LWKS). Prior to patient enrolment in the study, all participating endoscopists were considered to have performed at least 15 procedures with the ETMI system of which five were in patients with early neoplasia. In addition, the endoscopists were provided with an instructional DVD showing examples of AFI positive areas, HRE and NBI images of regular and irregular mucosal and vascular patterns as well as an instruction on the endoscopic study protocol.
Patients
Patients with Barrett’s oesophagus were included in the study if they were scheduled for endoscopy for the following reasons: (1) work-up of recently diagnosed HGIN/EC that, according to the referring physician, was endoscopically inconspicuous; (2) follow-up after endoscopic therapy for early neoplasia; and (3) regular Barrett’s oesophagus surveillance for low-grade intraepithelial neoplasia (LGIN) or non-dysplastic Barrett’s oesophagus. Patients with an active erosive oesophagitis (more than grade A according to the Los Angles classification of erosive oesophagitis) were excluded. The patients were enrolled on a first-come-first-enrolled basis. The study protocol was approved by the medical ethics committees of the participating institutions, and informed consent was obtained from all patients before the procedure.
The endoscopic tri-modal imaging system
The prototype ETMI system consisted of a high-resolution white-light endoscope with optical zoom (magnification 100×, XGIF-Q240FZ, Olympus Inc., Tokyo, Japan) equipped with an AFI and NBI mode. The light source (XCLV-260HP, Olympus Inc., Tokyo, Japan) contains two sets of rotating RGB filters: one for white-light imaging and one for NBI. For NBI the band-pass ranges of the RGB filters are narrowed to 530–550 nm (green) and 390–445 nm (blue). The intensity of the blue light is relatively increased while the intensity of the green light was minimised enabling enhanced imaging of the superficial mucosal surface and vasculature.
The ETMI endoscope has two separate high-quality monochromatic charge-coupled devices (CCDs); one for high-resolution white-light imaging and NBI, and one for AFI.
In the white light and NBI mode, the reflected red, green and blue light is detected by a monochromatic CCD and is converted into an electrical signal that is transmitted to the video processor (XCV-260 HP3P, Olympus Inc., Tokyo, Japan), which is synchronised with the rotary filter. The processor electronically overlays the red, green and blue images to produce a high-quality white-light or NBI image.
In the AFI mode, the image is composed of total emitted autofluorescence after blue light excitation (390–470 nm) and green reflectance (540–560 nm). A barrier filter is placed in front of the AFI CCD to only allow passage of fluorescent light with a wavelength between 500 and 630 nm, thus eliminating the blue excitation light.
All three imaging modalities of the ETMI system provide real-time endoscopic images. The location of control buttons on the handle of the endoscope enables easy and fast switching (1–2 s) between modalities.
Endoscopic procedure
Patients underwent upper endoscopy under conscious sedation with intravenous midazolam (5–10 mg) supplemented with fentanyl (50–100 μg) when necessary.
At the discretion of the endoscopist, a black flexible cap (MB-046, Olympus Inc., Tokyo, Japan) was mounted on the tip of the endoscope to facilitate magnification endoscopy during the procedure.
The oesophagus was first examined with HRE without magnification. The presence and length of the Barrett’s segment and/or hiatal hernia were recorded according to the Prague C&M classification.20 The oesophagus was further investigated for the presence of reflux oesophagitis and the presence of any visible abnormalities that raised a suspicion for early neoplasia. Visible abnormalities were defined and classified according to the Paris classification.21 22 For all suspicious lesions the location (distance from upper incisor teeth and endoscopic quadrant) were recorded. Subsequently, the Barrett’s segment was inspected with AFI for the presence of additional lesions. AFI suspicious lesions were defined as violet–purple areas while non-suspicious AFI areas were defined as light-green in colour. For all detected lesions the technique that primarily led to their detection was recorded and still images of these lesions were obtained with HRE and AFI. For lesions detected primarily by HRE their appearances with AFI were recorded and vice versa.
All suspicious lesions detected with HRE and/or AFI were further investigated with NBI and still images were obtained in overview and magnification. The following NBI characteristics were documented: (1) the mucosal pattern (regular, irregular or flat); (2) the vascular pattern (regular or irregular); and (3) the presence of abnormal blood vessels.18 Finally, the overall NBI appearance was classified as one of three categories: suspicious for neoplasia, not suspicious for neoplasia, or indeterminate. In addition, a number of unsuspicious AFI areas (green) were imaged with the three modalities. After completing inspection with HRE, AFI and NBI biopsy specimens were obtained of all suspicious lesions according to a prioritised biopsy protocol (see Biopsy protocol).
Biopsy protocol
For all detected abnormalities, irrespective of their final NBI appearance, a minimum of two biopsy specimens were obtained. A minimum of one biopsy sample was obtained from negative control areas. Finally, four-quadrant random biopsies were taken at every 2 cm of the Barrett’s segment avoiding taking biopsies from areas with suspicious lesions.
Biopsy sampling was performed using standard forceps with the following priorities: (1) all visible lesions were sampled before random sampling of the Barrett’s segment; (2) lesions that were only visible with AFI were sampled before lesions that were also recognisable with HRE; (3) lesions and control areas that were difficult to localise were sampled before easily recognisable lesions or control areas; (4) distal lesions were sampled before proximal lesions; (5) random sampling of the Barrett’s segment was preformed from distal to proximal.
Histological assessment
All biopsy specimens were routinely processed and stained. All specimens were routinely evaluated and subsequently reviewed by an expert gastrointestinal pathologist at each centre. The pathologists were blinded to the endoscopic findings. The histological outcome was recorded on standardised forms according to the revised Vienna classification of GI neoplasia in the following categories: non-dysplastic Barrett’s oesophagus, indefinite for dysplasia, LGIN, HGIN or invasive carcinoma.23
Outcome parameters
The following outcome parameters were assessed: (1) the number of patients diagnosed with HGIN/EC and the relative contributions of HRE, AFI and random biopsies in making this diagnosis (i.e. per patient analysis of the results); (2) the number of lesions with HGIN/EC detected with HRE and AFI (i.e. per lesion analysis of the results); (3) the reduction of false positive AFI findings after evaluation with NBI; and (4) negative predictive value of AFI-unsuspicious areas.
Statistical analysis
Continuous variables with normal distribution were summarised by the mean and standard deviation (SD), whereas those with a skewed distribution were summarised by the median and the inter-quartile range (IQR). All statistical analyses were performed using a statistical software package (Statistical Package for the Social Sciences 12.0.1; SPSS Inc, Chicago, IL).
RESULTS
Patient characteristics
From September 2005 to May 2007 eighty-four patients with Barrett’s oesophagus (70 males, mean age 67 years [SD 12]) were included in this study. The indications for endoscopy were: (1) surveillance of non-dysplastic Barrett’s oesophagus or LGIN in 42 patients; (2) work-up for endoscopically inconspicuous HGIN/EC in 33 patients; and (3) follow-up after endoscopic treatment of HGIN/EC in nine patients. The median length of the circumferential Barrett’s oesophagus segment was 4 cm (IQR 2–8) and the median length of the maximum extent of the Barrett’s oesophagus segment was 7 cm (IQR 4–10). One patient was found to have concomitant grade A reflux oesophagitis.
Per patient analysis
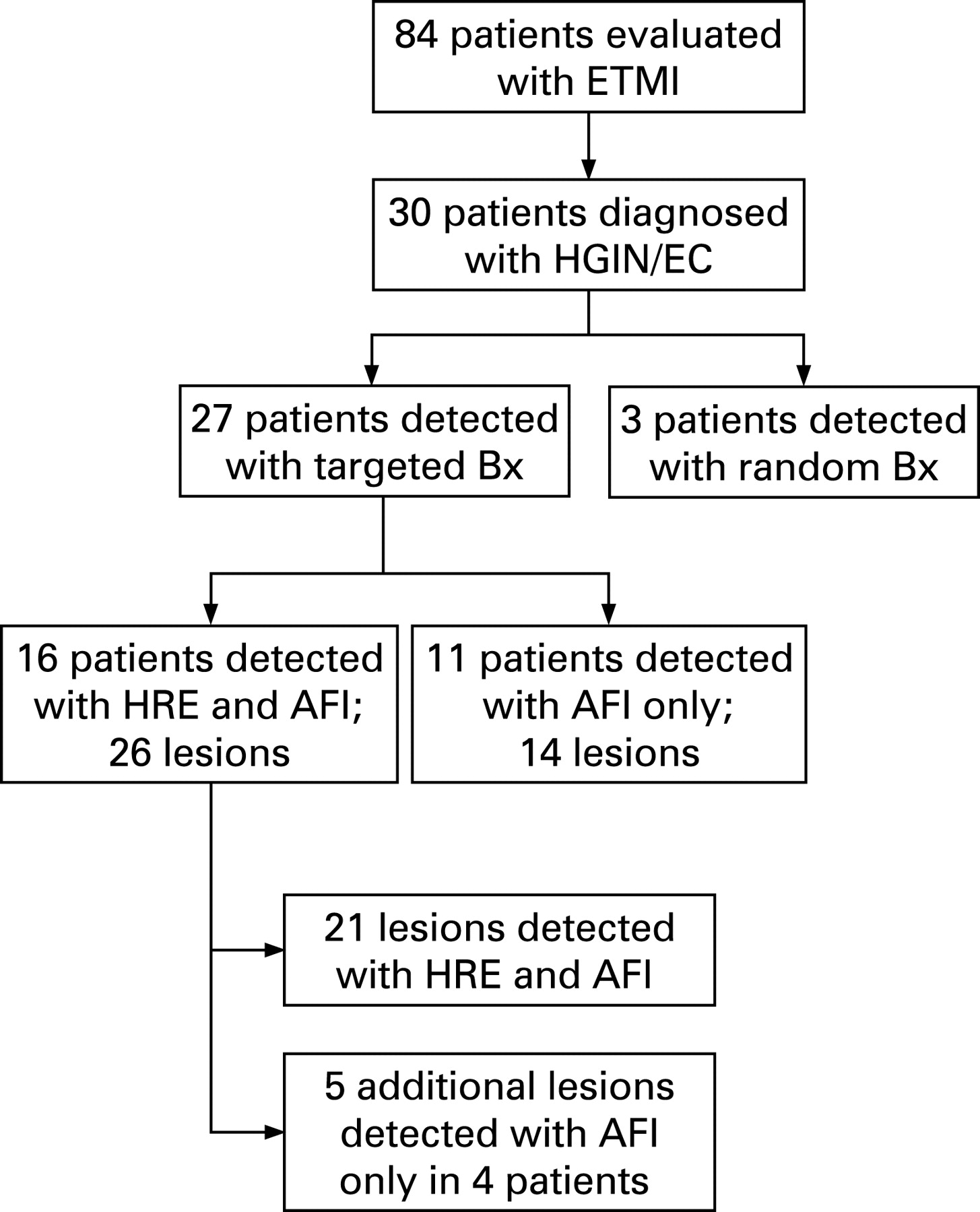
Thirty patients were diagnosed with HGIN/EC; most were referred for work-up of endoscopically inconspicuous HGIN/EC (23 patients), three patients underwent endoscopy for follow-up after treatment, and four patients underwent surveillance of which three had a prior history of LGIN.
Of the 30 patients diagnosed with HGIN/EC, 16 were detected with HRE, 11 were detected solely with AFI, whereas three were diagnosed only by random biopsies (fig. 1). In the 16 patients detected with HRE, the latter identified 21 visible lesions containing HGIN/EC. AFI correctly identified all these 21 lesions and detected five additional lesions in four of these patients that were not seen with HRE (fig. 1). In 11 patients no visible abnormalities were seen with HRE whereas AFI detected 14 lesions with HGIN/EC. Thus, relative to HRE, AFI increased the detection of patients with HGIN/EC in these 84 patients from 45% (16/30) to 90% (27/30). The use of AFI also increased the total number of detected lesions containing HGIN/EC from 21 (HRE only) to 40 (HRE and AFI combined).
Per lesion analysis
A total number of 165 lesions were identified as endoscopically suspicious with the ETMI system: 82 lesions were histologically non-dysplastic, eight were “indefinite for dysplasia”, 35 contained LGIN, and 40 contained HGIN/EC (fig. 2).

Sixty-three lesions were detected with HRE and 21 of these contained HGIN/EC, a false positive rate of 67% (42/63) (fig. 2). After detailed inspection with NBI, 20 of the 21 true positive lesions identified with HRE were found to be “NBI” suspicious versus 26 of the 42 HRE false positive lesions. The false positive rate of HRE was therefore reduced by detailed inspection with NBI from 67% (42/63) to 41% (26/63) at the expense of misclassifying one lesion containing EC as “NBI-unsuspicious”.
AFI detected 102 additional lesions that were not identified as suspicious with HRE; 19 lesions contained HGIN/EC: a false positive rate of 81% (83/102). After detailed inspection with NBI, 27 of the 83 false positive AFI lesions were noted as suspicious on detailed NBI inspection (figs 3 and 4). Of the 19 lesions containing HGIN/EC that were detected with AFI only, two containing HGIN were considered to have an unsuspicious NBI appearance. Therefore, NBI reduced the initial false positive rate of AFI from 81% (83/102) to 26% (27/102) at the expense of misclassifying two lesions containing HGIN as “NBI-unsuspicious”.


AFI-unsuspicious areas
In 71 patients, 97 areas with an unsuspicious AFI-appearance (light-green fluorescence) were imaged and subsequently biopsied. Eighty-four areas contained non-dysplastic Barrett’s oesophagus, three “indefinite for dysplasia” and 10 contained LGIN. The negative predictive value of AFI for this selected group of negative controls therefore was 100% (97/97).
No NBI evaluation was available for 18 of the 97 control areas. For the remaining 79 areas, 94% (74/79) was unsuspicious on NBI evaluation (fig. 5). Five lesions were classified as suspicious on NBI evaluation of which one contained LGIN and the remainders were non-dysplastic Barrett’s oesophagus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
One of the challenges concerning the endoscopic surveillance of Barrett’s oesophagus is the difficulty in detecting early neoplastic lesions with current endoscopic techniques. Surveillance guidelines for Barrett’s oesophagus, therefore, recommend taking random biopsies, which is inevitably associated with sampling error. AFI is an imaging technique that may improve the targeted detection of early neoplasia in Barrett’s oesophagus. In a recent study we showed that AFI increased the targeted detection rate of patients with HGIN/EC from 63 to 91%.12 Finding additional lesions with AFI after HRE was associated with a high false positive rate, however. In our first feasibility study, lesions that were detected with AFI and that were negative with HRE only showed HGIN/EC in 34% of cases.12 In a subsequent study, further assessment of AFI-suspicious lesions by NBI decreased the false positive rate to 10%.19 This approach, however, is impractical for routine practice given the need for two separate endoscopy systems.
This report is the first to describe the combined use of HRE, AFI and NBI incorporated into a single prototype endoscopy system in a multi-centre setting for the detection of early neoplasia in Barrett’s oesophagus. HRE and AFI were used as overview techniques for the detection of suspicious lesions with AFI as an adjunct to HRE. Subsequently, NBI was used for the detailed inspection of suspicious lesions detected with HRE and/or AFI.
In the current multi-centre study, AFI increased the targeted detection rate of HGIN/EC from 53% to 90%. The results confirm our previous single centre experience that AFI may significantly improve the targeted detection of HGIN/EC in Barrett’s oesophagus.12 19 Whether AFI will eliminate the need for taking random biopsies in Barrett’s oesophagus is difficult to conclude from this study. Three patients were diagnosed with HGIN based on random biopsies only and no visible abnormalities were noted with WLE and AFI. This implies that these three patients would have been missed if AFI would have been used instead of random biopsies. On the other hand, of the 11 patients who were found to have HGIN/EC in abnormalities detected with AFI only, nine showed no HGIN/EC in their random biopsies which might imply these would have been missed if random biopsies would have been used instead of AFI. The role of random biopsies in combination with AFI remains speculative, however, and randomised cross-over studies are needed to answer this question.
A drawback of AFI is its relatively high false positive rate of 81%. This is considerably higher than described in our previous studies where AFI was associated with a false positive rates of 40% and 51%.12 19 In these studies, however, lesions that were primarily detected with HRE and that were AFI positive were also included in the false positive rate analysis. If we exclude these lesions from our previous studies, the false positive rates of truly additional lesions detected with AFI (and thus negative on HRE) were 66% and 63%, respectively.12 19 Although we can not formally compare these false positive rates, these data suggest that in the current study a higher false positive rate was found than in our previous studies. Possible explanations for this finding may be the relative inexperience with the use of AFI in three of the four centres and the different AFI algorithm employed in the ETMI system compared to previous prototypes: three-band algorithm (i.e. autofluorescence, green reflectance and red reflectance) versus two-band algorithm (i.e. autofluorescence and green reflectance).
The high false positive rate of AFI, however, has to be put into perspective with the high false positive rate of 67% associated with HRE. This is probably explained by the tertiary referral function of the participating centres and the selected patient population. A high percentage of patients were referred for work-up of HGIN/EC and the participating endoscopists were not blinded to the patients’ clinical history. This may have led to endoscopically scrutinising the oesophagus and obtaining tissue samples from every small irregularity in the Barrett’s segment during inspection with HRE or from each area with a slightly different AFI appearance.
NBI is a new endoscopic technique that enhances the superficial imaging of mucosal and vascular patterns. We have reported that irregular mucosal and vascular patterns as well as the presence of abnormal blood vessels are associated with HGIN/EC, whereas regular patterns are associated with non-dysplastic Barrett’s oesophagus.18 In a proof-of-principle study in 20 patients, we showed that detailed NBI evaluation after AFI, reduced the false positive rate of AFI from 40% to 10%.19 In this study, NBI reduced the false positive rate of AFI from 81% to 26% (fig. 4). In addition, detailed inspection with NBI of HRE detected lesions also reduced the false positive rate of HRE from 67% to 44%. Although NBI appears to be a promising technique for reducing the false positive rate of AFI in Barrett’s oesophagus, there are some limitations. Three lesions containing HGIN/EC, one detected with HRE and two with AFI, were diagnosed as “NBI unsuspicious” after detailed inspection with NBI. Re-evaluation of the still images of these areas indeed showed regular mucosal and vascular patterns and no abnormal blood vessels; all features of non-dysplastic Barrett’s oesophagus according to our proposed classification of mucosal morphology.18 There are a number of possible explanations for these findings. First, irregular mucosal patterns, irregular vascular patterns, and the presence of abnormal blood vessels may not distinguish all dysplastic Barrett’s oesophagus areas from non-dysplastic Barrett’s oesophagus. Other features may be of importance for differentiating between neoplastic and non-dysplastic Barrett’s oesophagus (e.g. mucosal relief) or NBI images may not reveal them. Second, the areas evaluated with NBI may not have correlated with the endoscopically identified lesions (endoscopic sampling error) or the area biopsied (histological sampling error).
The true clinical relevance of NBI as a confirmatory technique remains to be shown in larger prospective studies. Moreover, studies assessing inter-observer agreement for the various mucosal and vascular features seen under NBI are needed. The current findings, however, suggest that it is questionable whether endoscopists can rely on their interpretation of NBI features of lesions to decide if these should be biopsied or not; simply taking biopsies from HRE and AFI suspicious lesions may be a more practical and easier approach.
Some limitations of this study need to be addressed. First, as aforementioned, this feasibility study was conducted in tertiary referral centres for Barrett’s oesophagus in a population with a high risk profile for HGIN/EC. The endoscopists all had extensive experience in evaluation and treatment of patients with a dysplastic Barrett’s oesophagus. In this setting, endoscopists were aware of the clinical history of the patients. With their experience the participating endoscopists may have detected suspicious lesions with white-light endoscopy that would be inconspicuous for less experienced endoscopists. In addition, the white-light image of the ETMI system is of superior quality compared to that of most standard endoscopy systems and may therefore allow the detection of more subtle lesions. This may lead to an under-estimation of the additional value of AFI. Second, white-light endoscopy and AFI were sequentially performed by the same endoscopist, therefore making the AFI assessment potentially biased by previous white-light findings. This may have led to an over-estimation of the detection rate of AFI.
We cannot exclude the possibility that certain areas were endoscopically mismatched (endoscopic sampling error) or wrongly sampled (histological sampling error). In addition, targeted biopsy sampling may have been obscured by bleeding from previous biopsy sites. All procedures, however, were performed by endoscopists with extensive experience in advanced imaging in Barrett’s oesophagus, all lesions were thoroughly documented during the procedure by an assistant on a specially designed scoring sheet, and a prioritised biopsy protocol was used starting with the lesion that was most difficult to recognise. We did not record procedure times during this study. ETMI in combination with random biopsies is probably more time consuming than standard video endoscopy with random biopsies. In future randomised studies procedure times of both methods will need to be taken into account.
Although a uniform pathology review would have been preferable to reduce inter-observer variability in the histopathological evaluation of Barrett’s oesophagus, in the current study all specimens were evaluated by two pathologists (including one expert gastrointestinal pathologist) in each centre. In addition, all participating centres were tertiary referral centres for the evaluation of Barrett’s neoplasia and have an extensive histopathological expertise in this field.
Since we did not have surgical resection specimens as the “gold standard” for our histopathology, we cannot exclude the possibility that other areas containing early neoplasia may have been missed.
In conclusion, this study established the feasibility of ETMI for enhancing the detection of HGIN/EC in Barrett’s oesophagus. AFI almost doubled the number of patients detected with HGIN/EC relative to HRE. This confirms our previous AFI results in a single centre setting. None of the control areas with unsuspicious AFI showed HGIN/EC upon biopsy suggesting a high negative-predictive value of AFI. AFI was, however, also associated with a high false positive rate. Subsequent lesion characterisation of AFI-suspicious lesions by NBI resulted in a reduction in the false positive rate. NBI, however, also misclassified two lesions containing HGIN. This questions whether detailed inspection with NBI may replace biopsy sampling in the future. Future randomised cross-over studies comparing ETMI with standard video endoscopy, especially performed in a non-expert setting, have to clarify the true diagnostic potential of ETMI for the detection of HGIN/EC in Barrett’s surveillance.
REFERENCES
Footnotes
Funding: The work of Wouter Curvers is supported by an unrestricted research grant from AstraZeneca BV, Zoetermeer, The Netherlands. The ETMI-prototype endoscopy equipment was provided by Olympus Inc., Tokyo, Japan.
Competing interests: None.
Linked Articles
- Digest