Article Text

Abstract
Introduction Gastro-oesophageal reflux occurs twice as much during transient lower oesophageal sphincter relaxations (TLOSRs) in patients with gastro-oesophageal reflux disease (GORD) compared to healthy volunteers (HVs). Our aim was to assess whether the localisation of the postprandial acid pocket and its interaction with a hiatal hernia (HH) play a role in the occurrence of acidic reflux during TLOSRs.
Methods Ten HVs and 22 patients with GORD (12 with HH<3 cm (s-HH), 10 with HH≥3 cm (l-HH)) were studied. The squamocolumnar junction and diaphragmatic impression were marked with a radioactively labelled clip. To visualise the acid pocket, 99mTc-pertechnetate was injected intravenously and images were acquired up to 2 h postprandial. Concurrently, combined manometry/impedance and four-channel pH-metry were performed, with pH pull-through at multiple time-points.
Results The rate of TLOSRs and the per cent associated with reflux was comparable between all groups. However, acidic reflux was significantly increased in patients, especially in patients with l-HH. Acid pocket length was significantly enlarged in patients. Moreover, immediately before a TLOSR, the acid pocket was more frequently located within the hiatus or above the diaphragm in patients with GORD (s-HH, 54%; l-HH, 77%) compared to HVs (22% of TLOSRs). Acidic reflux was significantly increased when the acid pocket was located above the diaphragm in all groups compared to a sub-diaphragmatic localisation.
Conclusion The position of the acid pocket is largely determined by the presence of a HH. Entrapment of the pocket above the diaphragm, especially in patients with l-HH, is a major risk factor underlying the increased occurrence of acidic reflux during a TLOSR in patients with GORD.
Statistics from Altmetric.com
Introduction
Increased oesophageal acid exposure is one of the most important hallmarks of gastro-oesophageal reflux disease (GORD), which is characterised by symptoms of heartburn, acid regurgitation and retrosternal pain.1 Symptoms are present in 30–40% of the Western population and about 5% suffer from daily symptoms.2 It is widely accepted that transient lower oesophageal sphincter relaxations (TLOSRs) are the main mechanism underlying the occurrence of gastro-oesophageal reflux in both patients with GORD and healthy subjects.3 4 Although some authors suggest that the number of TLOSRs is increased in patients with GORD, and contributes to increased acidic reflux, these data are rather controversial and not confirmed by others.5 6 In contrast, several studies agree that the risk of having acidic reflux during a TLOSR is twice as great in patients with GORD compared to healthy subjects.3–5 7 The underlying mechanism for this observation, however, remains unclear.
The presence of a hiatal hernia (HH) is one of the most important risk factors for GORD. Anatomical separation of the lower oesophageal sphincter (LOS) and the crural diaphragm leads to an altered pressure profile and significantly impaired anti-reflux barrier function of the oesophago-gastric junction (OGJ).8 Moreover, Pandolfino et al clearly demonstrated that a HH was also associated with an increased distensibility of the OGJ.9 Due to this change in mechanical properties of the OGJ, the risk of having liquid reflux increases, which was suggested to contribute to the increased acid exposure observed in patients with HH.9 Recent studies, however, show no difference in liquid reflux between patients with GORD and healthy controls,9–11 making it unlikely that changes in distensibility can explain the increased occurrence of acidic reflux during a TLOSR in these patients. The fact that liquid reflux is more frequently acidic in patients with GORD rather suggests that differences in acid or meal distribution in the proximal stomach or entrapment of acid in the hiatal sac must be involved. Previous studies showed that the hiatal sac can function as a reservoir from which ingested fluid can re-reflux into the oesophagus during periods of low sphincter pressure.12 13 After swallowing a barium bolus, patients with a large HH indeed had impaired clearance with stasis of contrast in the hiatal sac. In a proportion of patients, re-reflux of this contrast even occurred during swallowing. As comparable dynamics will apply when the hiatal sac is filled with gastric contents, this mechanism has been suggested to play a role in the increased acid exposure in patients with GORD. Evidence to support this hypothesis is lacking, however.
With the description of a postprandial acid pocket just distal of the squamocolumnar junction (SCJ) in healthy subjects by Fletcher et al,14 the acid environment in the proximal stomach has gained enormous interest. As the acid pocket may represent an unbuffered reservoir from which acid will escape into the oesophagus during periods of low LOS pressure, subsequent studies have further investigated the potential role of the acid pocket in the pathogenesis of gastro-oesophageal reflux.15–17 Two studies revealed that the acid pocket is larger and extends more proximal in patients with GORD compared to healthy subjects.18 19 To what extent these findings explain the increased oesophageal acid exposure observed in these patients remains unclear, however.20 Previous studies confirmed the presence of the acid pocket by pH pull-through,17–19 but this technique only provides information during a very brief period of time and thus is not suitable to study whether the position of the acid pocket determines the risk of having acidic reflux.
In the present study, we hypothesised that the position of the acid pocket relative to the diaphragm, rather than its size, could be an important determinant of acid exposure in the distal oesophagus. Especially in patients with a large HH, the acid pocket may be trapped in the hiatal sac above the diaphragm, facilitating the occurrence of gastro-oesophageal reflux. The position of a HH, however, changes frequently in time.21 Therefore, assessment of the acid pocket at a single fixed time point14 19 or even at 15 min intervals15–17 is insufficient to study the relationship between acid pocket position and gastro-oesophageal acid exposure. To this end, continuous registration of the acid pocket relative to the crural diaphragm is required. We previously reported preliminary evidence that the acid pocket can be visualised using single photon computed tomography (SPECT) of the stomach.22 When 99mTc-pertechnetate is injected intravenously, it is secreted by parietal cells and subsequently accumulates into the gastric lumen.22 Using SPECT scanning, three-dimensional images clearly showed that the accumulation of scintigraphic activity in the proximal stomach is not located within the stomach wall, but is a reservoir of secreted fluid.22 23 In the present study we validated and used this mechanism for dynamic scintigraphic visualisation of the postprandial acid pocket in both healthy subjects and patients with GORD and assessed the interaction between a HH, the acid pocket and acid exposure. Furthermore, we hypothesised that (1) the position of the acid pocket immediately before and during a TLOSR is a major determinant of the chemical composition of the refluxate; and (2) this position is determined by the presence of a HH. To evaluate these hypotheses, we continuously monitored the position of the acid pocket and simultaneously measured LOS function and gastro-oesophageal reflux in healthy subjects and patients with GORD with a small or large HH.
Materials and methods
Subjects
Studies were performed in 12 healthy volunteers (HVs) (mean age, 32 years (range, 22–53 years), seven men) and 22 patients with GORD (mean age, 52 years (range, 19–66 years), 12 men), of which 12 patients with no or a small hiatal hernia <3 cm (s-HH) and 10 patients with a large hiatal hernia ≥3 cm (l-HH). All HVs were free of any gastrointestinal symptoms. Only healthy subjects with a normal upper endoscopy and no HH were included. Patients with GORD were defined by the presence of oesophagitis obtained during a previous upper endoscopy or chronic heartburn symptoms responsive to proton pump inhibitor therapy. None of the subjects had a history of gastrointestinal surgery or took any medication known to influence gastrointestinal motility at time of the study. The use of proton pump inhibitors was discontinued for a minimum of 5 days prior to the study. Intake of alcohol and nicotine was not allowed 12 h and 4 h prior to the study, respectively. Each subject gave written informed consent to participate in the study.
Study design
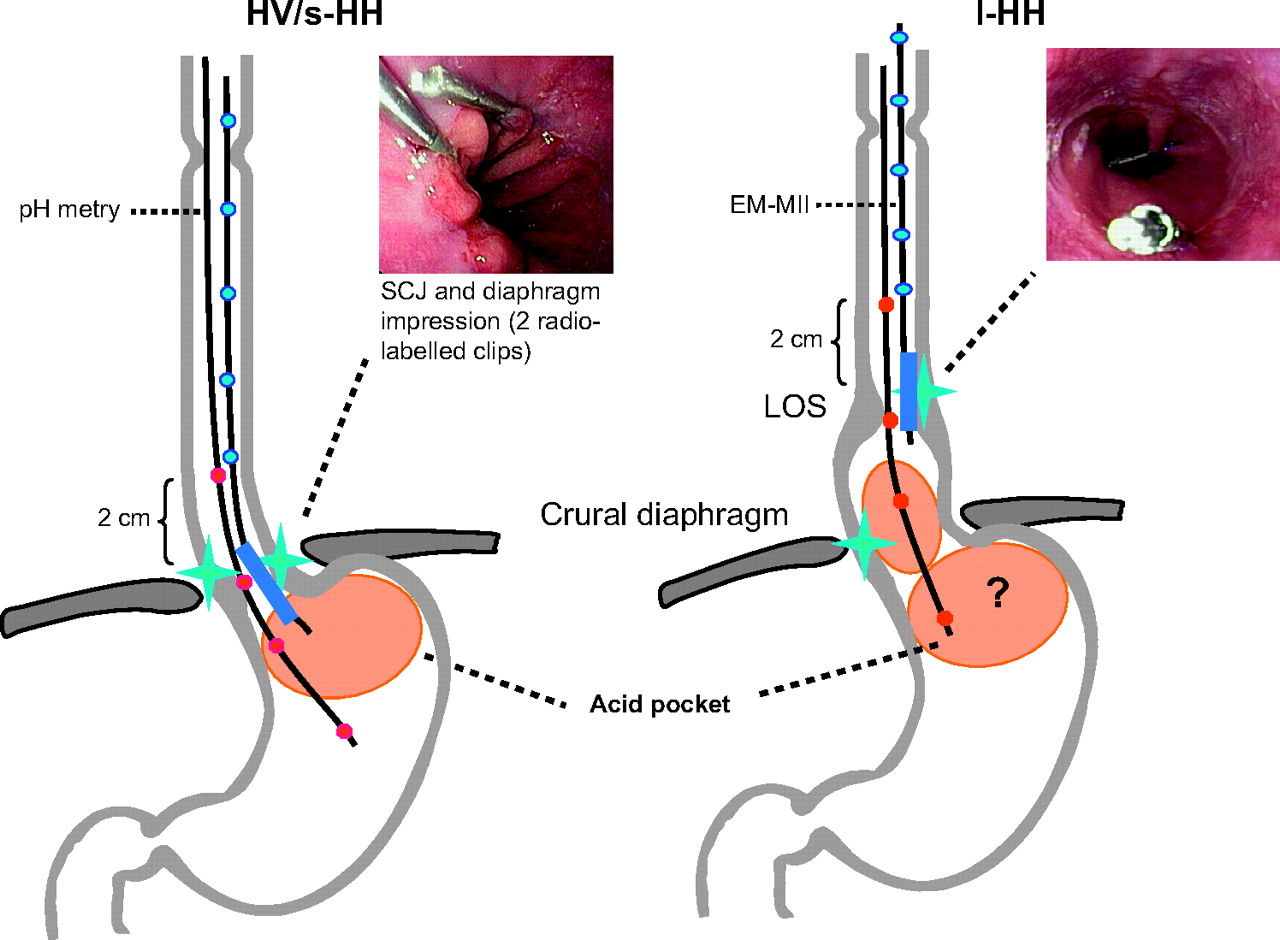
All studies were performed after an overnight fast. During upper endoscopy, performed after xylocaine throat spray, both the squamocolumnar junction and diaphragmatic impression were marked with a 99mTc-pertechnetate-labelled endoscopic clip (Boston Scientific International, Jeffersonville, Indiana, USA) (figure 1). After endoscopy, subjects were imaged fluoroscopically in the upright and supine positions to assess the exact size of the HH. The position of the diaphragmatic impression and the proximal extent of the gastric folds were ascertained from liquid barium swallows. The l-HH patients had ≥3 cm axial herniation of the gastric folds. Approximately 90 min after upper endoscopy, combined oesophageal manometry–multichannel intraluminal impedance (OM–MII), pH-metry and scintigraphy were performed. To record TLOSRs and reflux episodes, the OM–MII catheter (prototype developed by Taher Omari, Adelaide, Australia) was introduced through an anaesthetised nostril and positioned so that the sleeve straddled the LOS. To measure acidic reflux, a specially designed four-channel pH catheter (Zinetics 24ME multi-use pH catheter; Medtronic A/S, Skovlunde, Denmark) was introduced through an anaesthetised nostril and positioned with the most proximal pH electrode located 2 cm above the proximal margin of the LOS, the second pH electrode 4 cm distal to the proximal pH electrode (ie, within the LOS), the third and fourth pH electrodes were located 6 and 9 cm distal to the proximal pH electrode, respectively (figure 1). Thereafter, 450 MBq 99mTc-pertechnetate was injected intravenously for visualisation of the acid pocket. 30 min after injection, the subjects received a meal (510 kcal), consisting of two pancakes with jam and an orange juice (200 ml). After the meal, OM–MII, pH and scintigraphic recordings were performed for 2 h. In addition, pH catheter pull-through was performed preprandially and at 15, 30, 45, 60, 90 and 120 min after meal ingestion. Studies were performed in the sitting position, with the subjects leaning backwards against the gamma camera, and their upper body was restrained by a vacuum blanket to minimise movement.

Illustration of the study set-up in health volunteers (HVs) and patients with small hiatal hernia (s-HH; left) and large hiatal hernia (l-HH; right).
Recording methods
Manometry
The OM–MII catheter consisted of an eight-lumen water-perfused manometric assembly, with a sleeve sensor incorporated to monitor LOS pressure. A side hole at the distal margin of the sleeve monitored gastric pressure; oesophageal body pressure was recorded 3, 6, 9, 12 and 15 cm above the sleeve. A side hole in the pharynx monitored swallows. Each lumen was perfused with degassed distilled water at 0.1 ml/min, using a pneumohydraulic capillary perfusion pump (Dentsleeve Pty, Wayville, South Australia). Pressures were sensed by external transducers connected to a polygraph (Solar System; Medical Measurement Systems, Enschede, The Netherlands).
Impedance
The OM–MII catheter contained five pairs of cylindrical electrodes, spaced at 3 cm intervals. Each pair formed an impedance measurement segment, with the segments located 3, 6, 9, 12 and 15 cm above the sleeve. The electrodes were connected to an impedance transducer and data was sampled at a frequency of 50 Hz.
pH recording
A four-channel antimony pH catheter with external reference was used. Before and after the study the pH electrodes were calibrated at room temperature using pH 1.0 and 7.0 buffer solutions (Medtronic A/S). Calibration at room temperature was corrected by computer software for pH measurements at body temperature. At the start of each pull-through the pH catheter was further introduced into the stomach until at least the two most distal electrodes were measuring pH<3. The catheter was then withdrawn in 0.5 cm increments every 2 s until the most distal electrode measured oesophageal pH (>4). After each pull-through, the catheter was repositioned in its original location. Signals were digitalised, computer-processed, stored and analysed using commercially available software (Medical Measurement Systems).
Scintigraphy
Prior to each endoscopy, two stainless steel clips were radiolabelled by evaporating small drops of 99mTc-pertechnetate on the curved inside of one jaw with subsequent covering of this jaw with a thin layer of liquid and acid resistant methacylate coating. Finally, approximately 3 MBq 99mTc-pertechnetate was attached to each clip, remaining fixed under previously tested liquid and acidic conditions. Dynamic scintigraphic images were acquired on a gamma camera system (Orbiter; Siemens Medical Solutions, Illinois, USA), equipped with a low-energy all-purpose collimator. Thirty minutes after intravenous injection of 450 MBq 99mTc-pertechnetate, a baseline scan was made to identify the marked SCJ and hiatal hernia. Subsequently, after the meal, a dynamic acquisition was made up to 2 h (480 views, 15 s/view, 120 min total acquisition time). Every acquisition was processed on a Hermes processing station (Hermes, Nuclear Diagnostics, Stockholm, Sweden) for further analysis.
Data analysis
The position of the SCJ, considered to be localised 1 cm below the upper border of the LOS,24 was calculated for each subject and then averaged, allowing comparisons on pocket position between pull-through and scintigraphy.
Basal LOS pressure was measured at end-expiration relative to intragastric pressure, and was determined as visual means of 1-min periods every 15 min. TLOSRs were evaluated according to previously published criteria25: (1) absence of swallowing for 4 s before to 2 s after the onset of LOS relaxation, (2) relaxation rate of ≥1 mm Hg/s, (3) time from onset to complete relaxation of ≤10 s, and (4) nadir pressure of ≤2 mm Hg. LOS relaxations associated with a swallow and fulfilling the above-mentioned criteria 2, 3 and 4 that lasted more than 10 s were included as TLOSR. TLOSRs were counted for each subject during the two postprandial hours. In addition, the percentage of TLOSRs accompanied by an acidic reflux episode was determined, as well as the proportion of acidic reflux episodes associated with a TLOSR. From the oesophagogastric pH recordings, mean pH values were obtained during 2-min intervals every 10 min, providing a postprandial pH profile for each pH recording site in the distal oesophagus and stomach. Mean pH values were calculated per subject and per group by averaging the values of all healthy subjects, s-HH patients and l-HH patients separately.
Total acid exposure time was calculated either at the level of the LOS and at 2 cm above the LOS.
Reflux was defined as either pure liquid, pure gas or a mixture of liquid and gas detected by impedance. Liquid reflux was defined as a retrograde 40% fall in impedance from baseline starting at the most distal impedance site. Gas reflux was defined as a rapid increase in impedance (3 kΩ/s), occurring simultaneously in at least two impedance sites, in the absence of swallowing. Mixed reflux was defined as gas reflux occurring during or immediately before liquid reflux.10 11 Each reflux episode as recorded by impedance was classified as: (1) acidic reflux, with a pH fall from above to below 4; (2) non-acidic reflux; or (3) reflux during pull-through.
During pull-through, the pH step-up point was defined as a persistent increase in pH to oesophageal pH above 4. An acid pocket was defined as a drop in pH>2 units to a pH<4.16 17 For each pocket, its presence, length, location and mean pH were recorded. In addition, gastric pH and the mean pH of the buffering segment were calculated for each pull-through.
The scintigraphic length of the acid pocket and its position relative to the SCJ were measured at 15, 30, 45, 60, 90 and 120 min postprandially. Measurements were made through a straight line in a planar posterior view of the stomach. A pocket was considered as present, when a clear pool of radiolabelled activity was distinguishable in the proximal stomach. In the case of scintigraphic labelling throughout the stomach, no measurements on pocket length were performed. The radiolabelled clips were scintigraphically visualised as clear dots. The distance between the pocket and the SCJ was measured with the centre of the endoscopic clip marking the position of the SCJ. The position of the acid pocket relative to the diaphragm was determined by visual positioning of the acid pocket below, above or just overlapping the diaphragmatic clip. The spatial resolution, ie, the ability to detect two separate point sources of gamma photons, is approximately 2 cm apart, at 5 cm from the gamma camera detector. To minimise loss in spatial resolution, patients were positioned with their back against the detector. The system resolution for a point source at 5 cm is approximately 5 mm. Therefore, the margin of error in our measurements can be expected at the ±5 mm level.
Statistical analysis
Statistical analysis was performed using SPSS 12.02 software for Windows. Results are presented as mean ± SEM in the case of a normal distribution or as median and interquartile range for variables with a skewed distribution. For statistical analysis, the unpaired Student t test or the Mann–Whitney test were used. The correlation between pull-through and SPECT measurements was determined using the Spearman rank correlation coefficient, performed using Prism software version 4.00 (GraphPad). To identify independent risk factors for the occurrence of acidic reflux during a TLOSR, a multivariate analysis was performed. The effect of the co-variables on acidity was fitted via a logistic regression model with a random intercept (package lme4 in the statistical software program R (The R Foundation for Statistical Computing, Vienna, Austria). Acidic reflux was used as continuous variable and odds ratios (ORs) were calculated. A p value <0.05 was considered as statistically significant.
Validation of the scintigraphic detection of the acid pocket
After an overnight fast, 450 MBq 99mTc-pertechnetate was injected intravenously in two healthy subjects. Thirty minutes after injection, the subjects received a meal (510 kcal), consisting of two pancakes with jam and an orange juice (200 ml). Thirty minutes after the injection of 99mTc-pertechnetate, a scintigraphic scan was made to confirm the presence of an acid pocket. In addition, a nasal tube was introduced, with a radiolabelled clip attached to its distal end to localise its position. Subsequently, the acid pocket was aspirated and the pH of the substrate was measured. A repeated scan was made to test our hypothesis that the detected scintigraphic activity indeed represents luminal acid pooled on top of the meal rather than accumulation of 99mTc-pertechnetate in the gastric mucosa. Aspiration, with subsequent scanning, was repeated at 80 min postprandially.
Results
Validation of the scintigraphic detection of the acid pocket
Thirty minutes postprandially, a clear acid pocket was visualised scintigraphically, located in the proximal stomach. To determine that this scintigraphic activity indeed resulted from radiolabelled acid pooled on top of the meal, a gastric tube was introduced into this pool under scintigraphic guidance to aspirate the radioactive material. After aspiration of the pocket (70 ml), the scintigraphic activity disappeared, and slowly recovered within approximately 10 min (figure 2). The pH of the aspirated gastric content at 30 min postprandially was 1.8. A second aspiration at 80 min after meal intake resulted again in disappearance of the acid pocket. The pH of the aspirated gastric content (50 ml) was 2.3.

Validation study. Postprandially (PP), a clear acid pocket is observed in the proximal stomach. After aspiration of the acid pocket, the scintigraphic activity disappeared and slowly recovered. The clear dots resemble the radiolabelled clip attached to the distal end of the nasal tube used for aspiration.
Acid pocket length
Both pH pull through and scintigraphy demonstrated that acid pocket length was significantly increased in patients with GORD compared to HVs, reaching its maximum around 60 min postprandial. For further details, we refer to the supplementary file online.
Acid pocket position
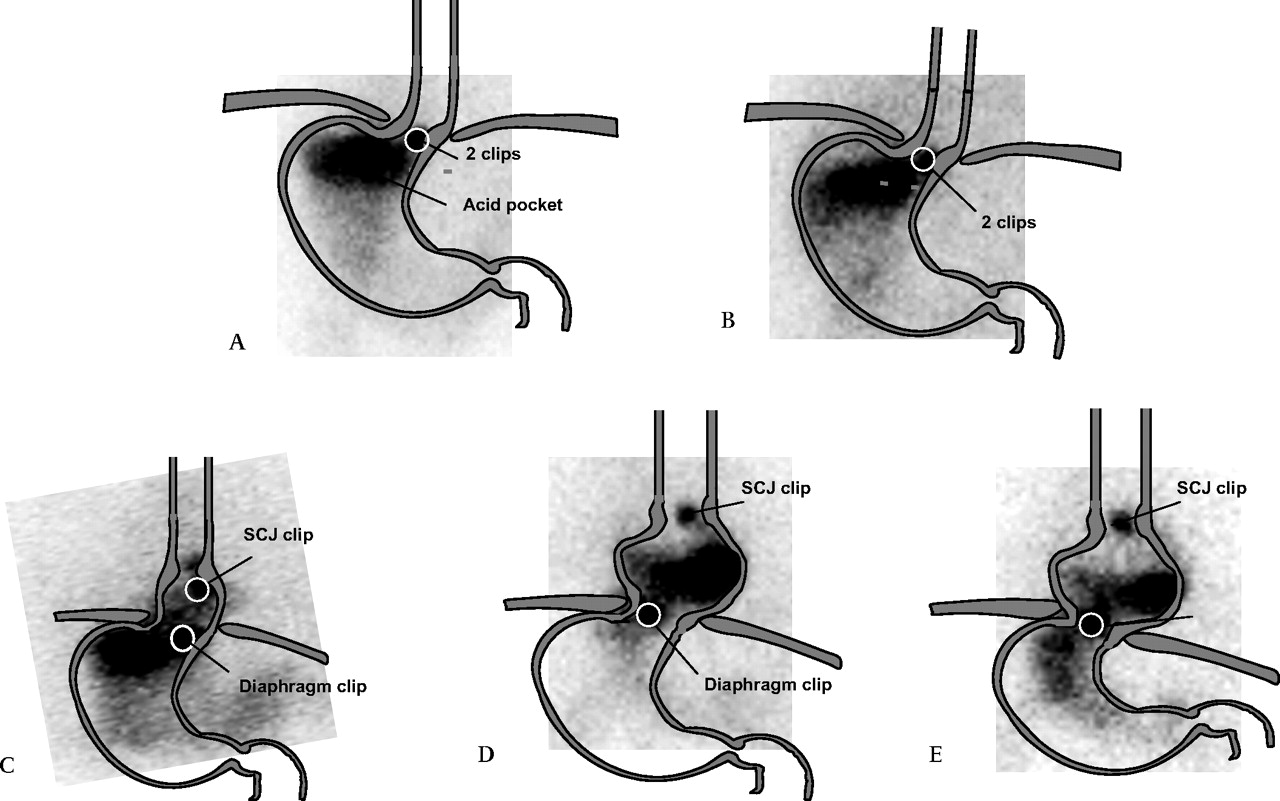
Before meal intake, the pH-transition point was located distally to the SCJ in all groups. Meal ingestion resulted in a non-significant proximal migration of the transition point in HVs. The postprandial pH-transition point was located above the SCJ throughout the entire study in 16% of the patients with s-HH and in 50% of the patients with l-HH (figure 3). Scintigraphically, the acid pocket was located immediately distal to the SCJ in HVs and patients with s-HH (figure 4). On the contrary, the acid pocket extended above the diaphragm during the entire study in 40% of the patients with l-HH. In the remainder of the patients with l-HH the pocket was largely located distal to the diaphragm but the acid pocket intermittently migrated actively into the hiatal sac in almost all patients (90%) (figure 4).

Individual measurements of the pH transition point in relation to the squamocolumnar juction (SCJ) before the meal and during the entire postprandial period. *p<0.05 compared to preprandial. §p<0.05 compared to healthy volunteers (HVs) and patients with small hiatal hernia (s-HH) during the corresponding period.

(A) Representative scintigraphic image of the postprandial acid pocket and squamocolumnar juction (SCJ) in a healthy subject. The SCJ and the level of the diaphragmatic impression are depicted as a clear dot. (B) Image of a patient with gastro-oesophageal reflux disease (GORD) and a small hiatal hernia (s-HH) in whom the acid pocket was located just distal to the SCJ. (C) A patient with GORD and a large hiatal hernia (l-HH) in whom the acid pocket located distal to the SCJ, but some acid is trapped in the hiatal sac. (D) A patient with a l-HH and with the acid pocket completely located within the hiatal sac. (E) A patient with a l-HH and with a large acid pocket extending into the hiatal sac.
Oesophageal coating
In those patients with l-HH and with the acid pocket continuously located within the hiatal sac, we observed frequent episodes of radiolabelling of the distal oesophagus (figure 5). In contrast to the acid pocket, the radiolabelling was less intense, suggesting a thin acid layer coating the oesophageal mucosa. If present, the proximal extension of this coating was 5.6±0.7 cm above the SCJ.

Image of a patient with a large hiatal hernia (l-HH) and with radioactivity in the distal oesophagus. No distinct pocket is observed, but intense radiolabelled activity is present throughout the stomach, including part of the hiatal sac. Note the clear, but less intense staining of the distal oesophagus. In line with this, pull-through did not reveal an acid pocket and the transition point was well located above the squamocolumnar juction (SCJ).
Scintigraphy versus pull-through
The correlation between scintigraphic and pull-through pocket length was 0.73 (p<0.0001). The correlation between the distance between the pocket and SCJ assessed using the two different techniques was less pronounced (r=0.45, p<0.0001). For more information, we refer to the supplementary file on line.
Reflux during TLOSRs: healthy volunteers versus patients with hiatal hernia
Three hundred and seventy-four TLOSRs were identified during the 2 h postprandial period: 152 in HVs, 124 in patients with s-HH and 98 in patients with l-HH. The number of TLOSRs per subject was comparable in HVs and patients with GORD (table 1). Of all TLOSRs, the majority was accompanied by a reflux episode as recorded with impedance (HVs: 88.0±4.7%; s-HH: 89.8±3.1%; l-HH: 92.1±3.2%). The composition of the refluxate is listed in table 1.
Rate of TLOSRs and the occurrence of reflux
Acidic reflux during a TLOSR occurred more frequently in patients with a HH. The per cent of TLOSRs accompanied by acidic reflux was significantly higher in l-HH compared to s-HH and HVs (figure 6A). This difference was most pronounced at 2 cm above the LOS. Total acid exposure was also increased in patients with a HH. Especially in patients with a l-HH, per cent time pH<4 was much higher both at the level of the LOS and 2 cm above the LOS (figure 6B).

(A) The percentage of transient lower oesophageal sphincter relaxations (TLOSRs) associated with acidic reflux is significantly increased in patients with gastro-oesophageal reflux disease (GORD) compared to healthy volunteers (HVs). (B) Acid exposure is significantly increased in patients with a large hernia. Data is presented as median and interquartile range (IQR) *p<0.05 compared to HVs.
Compared to HVs, the refluxate in patients with GORD extends significantly higher into the oesophagus, especially in patients with a large HH (proximal extent, measured from the upper margin of the sleeve: HV 7.3±0.4 cm; s-HH 8.8±0.3 cm (p=0.002); l-HH 11.5±0.4 cm (p<0.001)). When the acid pocket was located above the diaphragm, the proximal extent of the refluxate was 11.3±0.5 cm. This was significantly increased compared to episodes with the acid pocket located distally to the diaphragm (8.5±0.4 cm, p<0.001) or extending into the SCJ (9.1±0.4 cm, p=0.003).
Timing of reflux
Acidic reflux occurred throughout the entire study in all groups (figure 7). In HVs, the highest rate of acidic TLOSRs occurred between 40 and 60 min after the meal (55 min (IQR: 35–86 min)). In patients with s-HH, acidic TLOSRs were most frequent during the first postprandial hour (43 min (IQR: 19–75 min)), whereas in patients with l-HH, acidic TLOSRs occurred equally throughout the entire study (53 min (IQR: 20–86 min)).
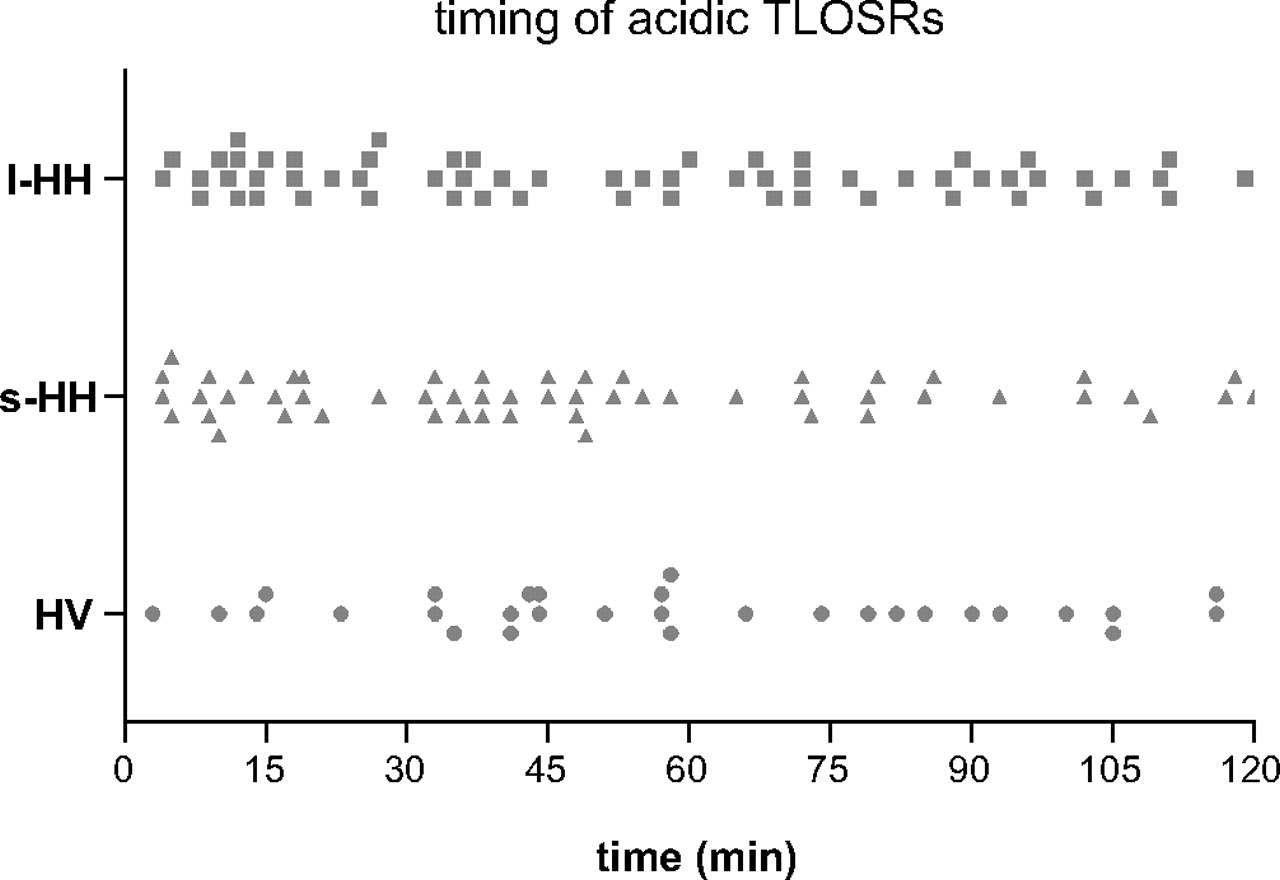
Timing of individual transient lower oesophageal sphincter relaxations (TLOSRs) accompanied by acidic reflux. Acidic reflux occurred throughout the entire study in all groups, especially in patients with large hiatal hernia (l-HH). In patients with small hiatal hernia (s-HH) and healthy volunteers (HVs), most acidic TLOSRs occurred during the first postprandial hour.
Acid pocket position prior to a TLOSR and the occurrence of acidic reflux
We hypothesised that the position of the acid pocket would largely determine the risk of having acidic reflux during a TLOSR. Therefore, we determined the position of the acid pocket relative to the most important anatomic landmarks, the SCJ and the diaphragm, immediately before the occurrence of a TLOSR. As shown in figure 8, the acid pocket was mostly located below the diaphragm in HVs. In contrast, in the presence of a HH, the acid pocket was more frequently located above the level of the diaphragm (figure 8A). Importantly, when the acid pocket was located below the diaphragm, only 7–20% of TLOSRs was accompanied with acidic reflux in all three groups studied (figure 8B). When the acid pocket was above the diaphragm before the onset of the TLOSR, this percentage increased significantly to more than 74–85% in all groups, including healthy subjects (figure 8B). In parallel, the number of non-acidic reflux episodes was clearly increased when the acid pocket was located below the diaphragm (figure 8C), an observation which was most frequent in HVs (figure 8A).

Position of the acid pocket immediately before the start of a transient lower oesophageal sphincter relaxation (TLOSR) (A). Note that in healthy volunteers (HVs), the acid pocket is located below the diaphragm during most TLOSRs. This in contrast to patients with large hiatal hernia (l-HH). (B) When the acid pocket extends into the hiatus or is located above the diaphragm, most TLOSRs are associated with acidic reflux. (C) Non-acidic reflux mainly occurred when the acid pocket was located below the diaphragm, both in HVs and in patients with gastro-oesophageal reflux disease (GORD).
A similar analysis was performed evaluating the relationship between the position of the acid pocket relative to the SCJ and the occurrence of acidic reflux during a TLOSRs; however, no relationship could be detected (data not shown).
Acid pocket position and the occurrence of acidic reflux during mechanisms different from TLOSRs
Also, for reflux episodes not related to a TLOSR, we evaluated the importance of the position of the acid pocket with regard to having acidic reflux. A total of 49 reflux episodes were recorded in 19 subjects (two HVs, eight patients with s-HH, and nine patients with l-HH). Almost half of the episodes were related to abdominal straining (49%). Other mechanisms were cough (12%), swallow induced (12%), deep inspiration (10%) and low LOS pressure (16%). Most episodes were non-acidic (67%). When the acid pocket was located below the diaphragm, 93.9% of the reflux episodes were accompanied by non-acidic reflux. In contrast, when the acid pocket was located above the diaphragm or extending into the hiatus, 85.7% and 88.9% of the reflux episodes are accompanied by acidic reflux, respectively.
Oesophageal shortening during TLOSRs and the occurrence of reflux
In the majority of TLOSRs, we observed a proximal movement of the clip positioned at the SCJ in all groups (figure 9), corresponding with oesophageal shortening (% TLOSRs with shortening are HV: 56±10%; s-HH: 62±10%; and l-HH: 77±7%). The mean length of shortening was 2.4±0.2 cm, 3.0±0.1 cm and 2.6±0.3 cm in HV, s-HH and l-HH patients, respectively. No differences were observed between acidic or non-acidic reflux episodes. Our scintigraphic technique was, however, not suited (too few pictures per time unit) to perform any further detailed analysis on shortening.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration of oesophageal shortening as it was observed during transient lower oesophageal sphincter relaxations (TLOSRs). A clear upwards movement of the squamocolumnar junction (SCJ) clip occurred, returning to its former position directly afterwards.
Factors associated with acidic reflux
Multivariate regression analysis identified the presence, but not the size of a hiatal hernia, and the position of the acid pocket above the diaphragm or extending into the SCJ as independent risk factors for the occurrence of acidic reflux during a TLOSR (table 2). On the other hand, the distance between the acid pocket and the SCJ was protective against acidic reflux.
Multivariate regression analysis of risk factors for acidic reflux
Discussion
In the present study, we introduced and validated a new method for continuous visualisation of the acid pocket to evaluate the importance of its position relative to the diaphragm in the pathogenesis of GORD. We showed that (1) in patients with a HH ≥ cm, the acid pocket is enlarged and extends into the hiatal sac above the diaphragm, associated with acidic coating of the distal oesophagus in almost half of these patients; (2) acidic reflux during a TLOSR occurs more often in patients with a HH, especially in those with a large HH, even in the early postprandial period; (3) the risk of having acidic reflux is mainly determined by the position of the acid pocket relative to the diaphragm, and (4) the position of the acid pocket is significantly influenced by the presence of a HH. These findings provide further insight in our understanding of the role of a HH in the pathophysiology of GORD, and for the first time provide an explanation for the increased occurrence of acidic reflux during TLOSRs in patients with GORD.
Intravenously injected 99mTc-pertechnetate is taken up and secreted by parietal cells in the gastric mucosa and accumulates into the gastric lumen.22 Using this technique in combination with radiolabelled clipping of the SCJ and diaphragm, we were able to show accumulation of the radiolabel in the proximal stomach, compatible with the acid pocket. Most importantly, scintigraphy allowed continuous visualisation of the pocket throughout the entire study period. Previously, it was questioned whether the acid pocket represents acid floating on top of the meal, or is rather created by a lack of buffering capacity of the meal.15 20 In the latter case, however, one would rather observe a more diffuse distribution of the radiolabel throughout the stomach and not a clear collection floating on top of the meal. Moreover, we clearly showed scintigraphic disappearance of the acid pocket after aspiration, with subsequent re-appearance of the pocket, confirming our hypothesis of newly secreted acid into the gastric lumen, leading to the formation of the postprandial acid pocket.
The incidence of an acid pocket after meal ingestion was comparable between HVs and patients with GORD. The size of the acid pocket was, however, significantly increased compared to HVs, especially in patients with l-HH. Compared to previous studies,14–19 the length of the acid pocket measured in our study was greater both in HVs and patients with GORD. This difference might be due to methodological differences in the pull-through technique. Irrespectively, scintigraphic assessment of the acid pocket correlated well with the pull-through recordings.
More important was our finding that the position of the acid pocket in patients with l-HH differed from patients with s-HH and with HVs. In approximately 40% of patients with l-HH, the acid pocket was continuously located within the hiatal sac, whereas in the remainder of patients with l-HH, the acid pocket intermittently migrated into the hiatal sac throughout the study. This in contrast to the suggestion by Clarke et al that a hiatal hernia provides a physiological acid pocket as it is lined by acid secreting mucosa.18 Rather than size, we suggest that this supradiaphragmatic location of the acid pocket represents an important mechanism promoting acidic reflux into the distal oesophagus. In line with this, we clearly showed coating of the distal oesophagus with radiolabelled material in those patients where the acid pocket was trapped within the hiatal sac. The intensity of this staining was less pronounced compared to the activity of the pocket, most likely compatible with coating of the distal oesophageal mucosa with a thin acid layer. This was further confirmed by the observation that the proximal extent of the coating corresponded well with the proximal extension of the pH-transition point above the SCJ. Our findings are in line with those previously reported by Pandolfino et al,19 who suggested that this proximal extension of the transition point above the SCJ most likely represents an acid film coating the mucosa, as it occurred in the context of an intact oesophagogastric high-pressure zone. In both studies, coating occurred in patients with large hiatal hernias, strengthening the hypothesis that mechanical disruption of the oesophagogastric junction promotes either re-reflux from the hiatal sac, poor oesophageal clearing or probably diminished buffering capacity of the mucosa or saliva.
For years, it has been known that patients with a large HH are more prone to have acidic reflux than patients with no or a small hernia.26–31 Low LOS pressure, impaired clearance and accumulation of gastric contents in the hiatal sac, thereby facilitating reflux during swallow-induced LOS relaxation, are proposed as possible mechanisms for this increased acid exposure. It has previously been suggested by Pandolfino et al that a positive pressure gradient between the stomach and oesophagus, developed by repositioning the SCJ to a supradiaphragmatic position, is a prerequisite for reflux to occur.32 This pressure gradient can be achieved by abdominal straining, inspiration or positioning of the OGJ above the diaphragm into the thoracic cavity. In the setting of a HH, this separation is pre-existent. In addition, Bredenoord et al recently reported episodes of intermittent separation of the LOS and diaphragm, both in patients with GORD and in healthy subjects.21 33 Moreover, in that study, reflux occurred more frequently during evident spatial separation of the diaphragm and LOS.21 It is most likely that, in the setting of normal anatomy, repositioning of the OGJ above the diaphragm occurs as a result of oesophageal shortening.32 34 35 In the present study, we confirmed the occurrence of oesophageal shortening, a phenomenon associated with TLOSRs.32 34 35 Due to the limited number of images per time unit, however, our scintigraphic technique does not allow the determination of the precise relationship between shortening, timing of LOS relaxation and the occurrence of reflux.
Although the presence of a HH and the phenomenon of oesophageal shortening are important factors in the occurrence of gastro-oesophageal reflux, it remains unexplained why acidic reflux occurs more frequent in patients with GORD compared to healthy controls, especially in the postprandial period when acid is thought to be buffered by the meal. Comparable to Sifrim et al,10 11 the risk to have (acid and non-acid) reflux in our study is comparable in healthy controls and patients with GORD. In contrast, and in line with previous studies,6 36–38 acidic reflux is more frequently acidic in GORD patients compared to HVs, most pronounced in patients with a large HH. This observation rather suggests that differences in acid or meal distribution in the proximal stomach or entrapment of acid in the hiatal sac must be involved. Our study is the first study to provide evidence supporting this hypothesis. We showed that the position of the acid pocket above the diaphragm is a major risk factor for acidic reflux to occur during a TLOSR. Indeed, when the acid pocket is located above the diaphragm or is extending into the hiatal opening, 70–85% of all TLOSRs are accompanied by acidic reflux. In contrast, when the acid pocket is located below the diaphragm prior to a TLOSR, only 7–20% is accompanied by an acidic reflux episode. Most importantly, this observation not only holds for GORD patients, but even for healthy volunteers, illustrating its importance in determining the composition of the refluxate. As a consequence, factors influencing the position of the acid pocket relative to the diaphragm will have a major impact on the risk of having acidic reflux during episodes of an insufficient anti-reflux barrier.
Most likely, the most important factor determining the position of the acid pocket is the presence of a HH. In patients with a HH, the acid pocket was located more frequently above the diaphragm compared to HV (76% vs 22%). Multivariate regression analysis revealed the presence of a HH and a supradiaphragmatic acid pocket position as major independent risk factors for acid reflux to occur, with odds ratios above 5. This supradiaphragmatic position occurred more frequently with increasing size of the hernia. In line with this supradiaphragmatic position, the per cent of TLOSRs accompanied by acidic reflux is highest in patients with a large HH. Whereas in HVs only 3% of all TLOSRs was associated with acid reflux, this increased to 43% and 64% in patients with, respectively, a small and large HH. The combination of a positive pressure gradient due to the hernia and acid trapped within the hiatal sac almost guarantees the occurrence of acidic reflux during TLOSRs or when LOS pressure is low.
Even in HVs, most acidic reflux episodes occurred when the acid pocket extended into the hiatus during a TLOSR. This phenomenon could be explained by the intermittent spatial separation of the LOS and diaphragm.33 39 Bredenoord et al showed that maximum separation was approximately 2.5 cm, both in patients with a small hernia and in HVs.21 33 When during this separation the acid pocket migrates upwards with the LOS, a situation comparable with a small hernia is formed, promoting acidic reflux. Thus, any extension of the acid pocket above the diaphragm seems to be sufficient to promote acidic reflux, as long as it occurs in the presence of a positive pressure gradient caused by separation of the LOS and diaphragm, both in HVs and in patients with GORD. In contrast, when the acid pocket was located below the diaphragm, reflux was mainly non-acidic. Our hypothesis is further strengthened by the observation that not only during TLOSRs, but also during reflux episodes caused by other mechanisms, the position of the acid pocket is of major importance. Although most reflux episodes related to mechanisms different from TLOSRs were non-acidic, a supradiaphragmatic position of the acid pocket resulted in acidic reflux in 85–89% of these episodes. Half of the reflux episodes not related to a TLOSR occurred during straining, when, although a positive pressure gradient is clearly present, still the majority of all reflux events was non-acidic because of a subdiaphragmatic position of the acid pocket.
Recently, the role of the acid pocket in the occurrence of acidic reflux was questioned as a disparity was suggested between the time course of the acid pocket and that of the occurrence of acidic reflux.20 This conclusion was based on the assumption that the acid pocket exists for only 60–90 min after meal intake, whereas acidic reflux episodes would appear mainly during the second postprandial hour. We clearly showed that acidic reflux occurs throughout the entire study period in both HVs and GORD patients. Moreover, in patients with a HH, the highest rate of acidic reflux episodes occurs during the first postprandial hour. These findings argue against the suggestion that acidic reflux hardly occurs directly postprandial due to buffering of the meal,11 but favour the assumption that the position of the acid pocket determines whether refluxate is acidic or not. This was indirectly supported by our observation that the occurrence of acidic reflux during TLOSRs in time parallels the presence of the acid pocket. TLOSRs accompanied by acidic reflux were most prevalent between 45 and 60 min after the meal in HVs and patients with s-HH and GORD, the time window in which the size of the acid pocket is maximal and in close proximity to the SCJ.40 In patients with a l-HH, acidic reflux during TLOSRs was recorded throughout the entire study, coinciding with entrapment of the acid pocket in the hiatal sac as visualised on the scintigraphic images.
Despite a good correlation between scintigraphy and pH pull-through, some discrepancies occurred between both techniques. First, when the acid pocket is located more towards the fundus, part of the pocket will be easily missed by the pH catheter. Consequently, conventional pH pull-through might incorrectly demonstrate the presence or absence of an acid pocket, whereas scintigraphy provides detailed information on the exact localisation of the pocket. Second, as acidic contents may be pulled up with the pH sensor during pull-through, the proximal border of the acid pocket may incorrectly be determined more proximally compared to scintigraphy. On the other hand, our scintigraphic method was limited in some cases by the inability to determine the position of the radiolabelled clips because of overlap with the acid pocket. Attempts to label the clips with another radioisotope, such as 111In, to overcome this technical problem failed. Finally, even when the acid is finally mixed with the meal and buffered, the radioactive label will still be detected and will be misinterpreted as gastric acid, leading to overestimation of pocket length. It could be interesting for future studies to use an alternative radiolabelled meal to locate the meal in relation to the acid pocket and get insight in the mixing properties of the pocket.
What is the clinical impact of our findings? First of all, our data provide additional evidence highlighting the importance of a HH in the pathogenesis of GORD. In addition, we demonstrate that the acid pocket is an important determinant of the chemical composition of the refluxate. From a therapeutic point of view, this would imply that reduction of the size of the acid pocket by acid suppression could contribute to the beneficial effect of proton pump inhibitors in GORD. Vo et al indeed demonstrated that PPI treatment decreases the amount and size of postprandial acid pockets.17 Furthermore, pharmacological agents, like baclofen or prokinetics might be effective, at least in part, by altering the position of the acid pocket due to inhibition of the postprandial fundic relaxation41 42 or by enhancement of gastric emptying,43 respectively. Finally, especially in patients with a large HH, the acid pocket will be entrapped in the hiatal sac and will easily enter the oesophagus during episodes of low LOS pressure. To what extent reflux inhibitors or drugs increasing LOS pressure will be efficient to prevent reflux under these conditions is rather questionable and deserves further study. In these patients, it would therefore be more appropriate to surgically correct the large HH and to reposition the stomach and the acid pocket within the abdominal cavity.
In summary, we showed that a supradiaphragmatic position of the acid pocket represents an important mechanism promoting acid reflux into the distal oesophagus. Besides a significantly enlarged acid pocket compared to HVs, the acid pocket is captured in the hiatal sac in patients with a large HH, leading to increased reflux and acidic coating of the distal oesophagus. Furthermore, this study demonstrates that the observation that patients with GORD more often have acidic reflux during a TLOSR compared to HVs results from differences in the dynamics of the postprandial acid pocket. Supradiaphragmatic localisation of the pocket was more frequent in patients with GORD, especially those with a large HH, and was associated with a 5-fold risk of having acidic reflux. These findings contribute to a better understanding of the pathogenesis of GORD and further stress the importance of a HH in promoting acidic reflux.
References
Supplementary materials
Web only data gut.2009.178061
Files in this Data Supplement:
Footnotes
Linked article 192922.
Funding HB is supported by an unrestricted grant from AstraZeneca. GEB is supported by a grant (Odysseus program, G.0905.07) of the Flemish “Fonds Wetenschappelijk Onderzoek” (FWO).
Competing interests None.
Ethics approval The study was approved by the Medical Ethics Committee of the Academic Medical Center, Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.