Article Text

Abstract
Aim The aim of this epidemiological study was to follow the time trends of mortality from gastric cancer and compare them with those of gastric and duodenal ulcer.
Methods Mortality data from Denmark, England & Wales, Italy, Japan, Switzerland and the United States of the past 57–130 years were analysed. The age-specific death rates were plotted against the period of death as period-age contours and against the period of birth as cohort-age contours.
Results The long-term time trends of gastric cancer mortality were found to rise among generations born during the 18th century until the first half of the 19th century and then decline in all subsequent generations. The rise and fall of gastric cancer preceded similar birth-cohort patterns of gastric and duodenal ulcer by about 10–30 years. With the exception of gastric cancer in the USA, similar birth-cohort phenomena were seen in all countries. In general, similar temporal patterns were also seen in men and women analysed separately.
Conclusions The time trends of mortality from gastric cancer are shaped by an underlying birth-cohort pattern that resembles similar patterns of peptic ulcer mortality. The occurrence of birth-cohort phenomena in gastric cancer and peptic ulcer suggests that additional secular trends besides changes in the infection with Helicobacter pylori must have contributed to the peculiar long-term behaviour of these diagnoses.
- Birth-cohorts
- childhood infection
- duodenal ulcer
- gastric cancer
- gastric ulcer
- Helicobacter pylori
- mortality
- time trends
- epidemiology
Statistics from Altmetric.com
- Birth-cohorts
- childhood infection
- duodenal ulcer
- gastric cancer
- gastric ulcer
- Helicobacter pylori
- mortality
- time trends
- epidemiology
Introduction
The incidence of gastric cancer has fallen dramatically in all Western countries.1 This fall has been ascribed to the declining infection of the general population with Helicobacter pylori. Similarly to gastric cancer, gastric and duodenal ulcers are both linked to upper gastrointestinal infection with H pylori. The time trends of both ulcer types are known to be influenced by an underlying birth-cohort pattern.2 The risk of developing peptic ulcer increased among generations born during the 19th century. After reaching a peak shortly before the turn of the century, the risk started to decrease among all subsequent generations born during the 20th century. This birth-cohort pattern with its characteristic rise and fall has shaped the time trends of peptic ulcer in most Western countries.3 It has been observed in the time trends of essentially all morbidity parameters associated with peptic ulcer disease, such as hospitalisation, disability pensions, and mortality.2–7
Until now no such birth-cohort pattern characterised by an initial rise and subsequent fall has been reported in gastric cancer. During the time periods previously available for epidemiological analysis, the trends of gastric cancer always appeared to have been characterised by a steady decline that affected all consecutive generations alike.8 At best, the earliest birth-cohort data of gastric cancer seemed to suggest an initial plateau that was consistent with the concept of an endemic H pylori infection of the general population before increasing standards of hygiene made the infection subside. The aim of the present study was to analyse the long-term time trends of gastric cancer and extend the time frame of previous analyses. Whereas previous publications by the author dealt with the time trends of gastric and duodenal ulcer,3 the present analysis is focused primarily on the time trends of gastric cancer, which have not been presented before. It was hypothesised that the long-term trends of gastric cancer would be characterised by a stable plateau throughout the 19th century and the absence of any rise in its age-specific death rates. Unexpectedly, the analysis revealed a rise in mortality from gastric cancer during the first half of the 19th century that preceded the rise in the occurrence of both ulcer types by 10–30 years.
Methods
Data sources
The data were made available by the national statistical offices of the individual countries. The more recent data sets were supplied as Excel spreadsheets, whereas the older data were supplied as photocopies from annual compilations of causes of death or published annual vital statistics. The resident population of the six countries, stratified by sex and 5- or 10-year age groups, was also provided by the national statistical offices.
The present analysis comprised the six countries listed in table 1. The four European countries were chosen because their vital statistics of gastric cancer covered the longest available time periods of 70 and more years (Denmark, England & Wales, Switzerland and Italy). Japan and the United States were included in the present analysis because of their large population size and to gain perspective on gastric cancer time trends outside Europe. In addition to gastric cancer, deaths from gastric and duodenal ulcer were analysed for comparison. The number of deaths from gastric cancer, gastric ulcer and duodenal ulcer were broken down by 5- or 10-year age groups and individual years of death.
Number of deaths associated with gastric cancer and peptic ulcer
In general, deaths were recorded by cause according to the 1st through 10th revision of the International Classification of Diseases (ICD) (table 2). Individual countries varied by the date when they switched among different revisions of the ICD, and the periods listed in table 2 serve only as an approximation of when an actual ICD version was used. Some countries continued to record data only by a two- or three-digit ICD codes and abstained from utilising the more detailed subcodes. A separate ICD code was assigned to gastric cancer only in the 3rd revision of the ICD. However, individual countries, such as Denmark, England and Switzerland, started to record gastric cancer deaths prior to the introduction of the 3rd revision of the ICD. Since the 8th revision of the ICD a separate code has been assigned to malignant neoplasms of the cardia (151.0 and C16.0), which in most instances refers to oesophageal adenocarcinoma. This code was not included in the present analysis of gastric time trends. (Although death associated with ICD codes 151.0 and C16.0 has markedly increased during the past 20–30 years, it has never exceeded 10% of all deaths from gastric cancer.) In the case of gastric and duodenal ulcer, all codes associated with acute versus chronic ulcer, bleeding or perforation were lumped together and the temporal analysis was restricted to three-letter ICD codes only.
ICD codes pertaining to gastric cancer and peptic ulcer
Data analyses
In each country separately, age-specific death rates were calculated for consecutive 10-year periods and 10-year age groups. For instance, the total number of deaths from 1971 until 1979 among subjects aged 45–54 was divided by the corresponding number of the total resident population of the same age group and living during the same time period when the deaths occurred. In some of the countries, the first time period was represented by less than 10 years, for instance, 5 years in case of gastric cancer in Denmark during 1876–1880 or 8 years in case of gastric cancer in Italy during 1933–1940. Similarly, in all countries the most recent decennium 2001–2010 was represented by only 5–7 consecutive years. The death rates were expressed per million living population. The age-specific deaths rates were plotted against the period of death as period-age contours and against the period of birth as cohort-age contours. In the plots, each age group was labelled by its central year, for instance, 20 indicating the age group 15–24 and 30 indicating the age group 25–34. The periods of death were labelled by the mid year of death, for instance 1955 instead of 1951–1960 and 1965 instead of 1961–1970. The data analyses were carried out using Excel from Microsoft (Redmond, Washington, USA).
Statistical analyses
The age-standardised cohort mortality ratio (SCMR) was used as a summary statistic of the overall mortality associated with each consecutive birth-cohort as previously described.3 Briefly, the SCMR was calculated similarly to the standardised mortality ratio (SMR) as the ratio of observed (O) over expected (E) number of deaths in each birth-cohort: SCMR=O/E.9 The SCMR was expressed as a percentage and plotted against the period of birth. The numbers of observed and expected deaths summed over all birth-cohorts are equal, that is ∑O = ∑E, with an overall average ratio of ∑O/∑E = 1 or 100%. The individual SCMR value indicates to what extent the SCMR associated with an individual birth-cohort lies above or falls below the overall average ratio of 100%. The standard error (SE) of the SCMR is SE = SCMR/√O.10 The statistical significance of the difference between two values SCMRa and SCMRb was determined using a z-test with z = (SCMRa − SCMRb)/(SEa2 − SEb2)½.
Results
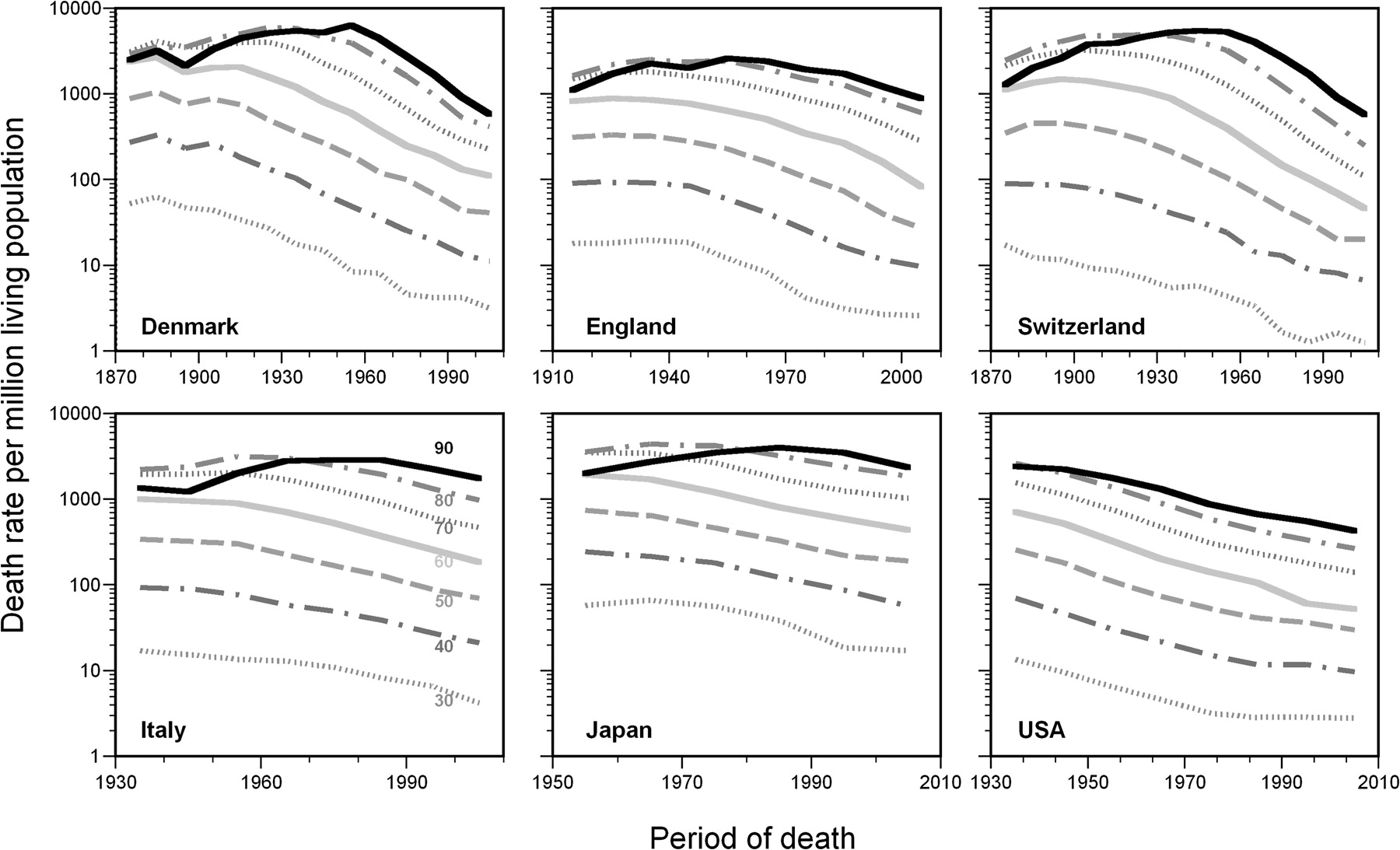
Figure 1 shows the period-age contours of mortality from gastric cancer among the six countries. In general, mortality was much higher among the older than younger age groups. The same line patterns in different countries refer to the same age groups, as indicated in the lower left graph representing Italy. In order to present the time trends of all age groups in a single graph, a logarithmic y-axis was chosen. In the USA, the period-age contours of all age groups ran a steady and parallel downward course. In the other countries, however, the period-age contours of the older age groups showed an initial rise followed by a subsequent decline. The rise was most pronounced and longest in the oldest age group. This initial rise became increasingly shorter in the younger age groups and was mostly absent in the age groups 35–44 and younger. It was also more pronounced in the countries with the longest time trends (Denmark, England, Switzerland) as opposed to the two countries with shorter time trends (Italy, Japan). Period effects, such as the introduction of diagnostic techniques or medical therapies, generally affect all age groups at the same time. In general, period effects reveal themselves as rise or fall occurring in all age groups alike during the same time period. In contradistinction, the rising trends among old and falling trends among young patients occurred simultaneously. This concurrence of different patterns among period-age contours of consecutive age groups is highly suggestive of underlying cohort effects.

Age-specific death rates of gastric cancer plotted as period-age contours, logarithmic scale.
The same age-specific death rates of gastric cancer as those depicted in figure 1 are plotted against the period of birth in figure 2. For instance, individuals in Denmark who died aged 90 between 1875 and 2005 were born between 1785 and 1915. Hence, the oldest period-age contour of Denmark, running between 1925 and 2005 in figure 1, changes into a cohort-age contour running between 1775 and 1915 in figure 2. Similarly, Danish individuals who died aged 30 between 1875 and 2005 were born between 1845 and 1975. Plotted against the period of birth rather than period of death, the death rates become re-aligned as cohort-age contours, which cover a much longer time of 190 years (1785–1975) as opposed to the 130 years (1875–2005) covered by the period-age contours. A vertical line perpendicular to the abscissa of figure 2 intersects the cohort-age contours of individuals born during the same time period, but who died from gastric cancer at a different age and during different time periods.
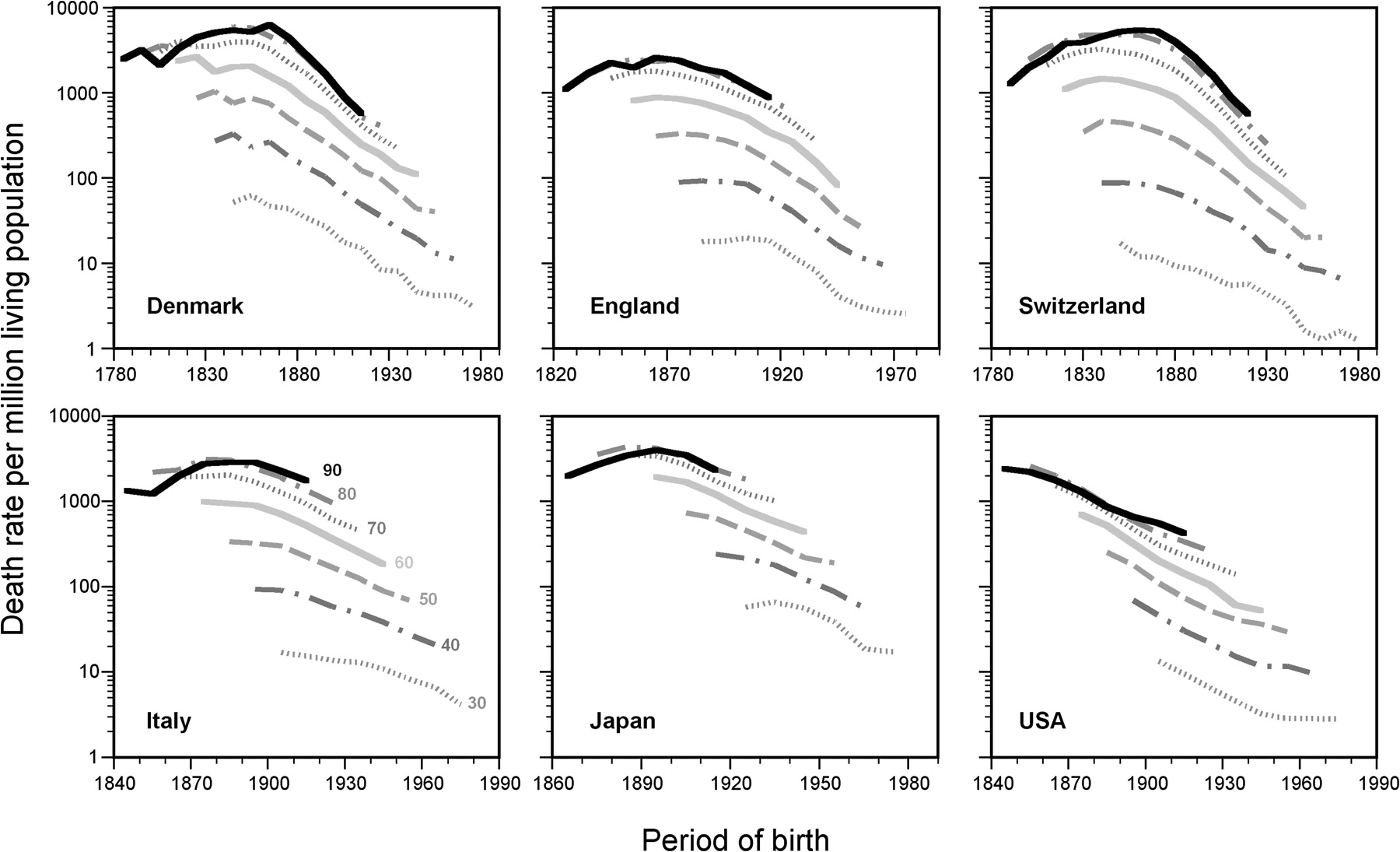
Age-specific death rates of gastric cancer plotted as cohort-age contours, logarithmic scale.
The conversion from period-age to cohort-age contours pulls the individual age-specific curves apart but leaves their individual shapes unchanged. The individual cohort-age contours align in a pattern that resembles a hyperbola with an initial rise and a subsequent decline associated with consecutive periods of birth. The oldest age groups participate in the initial rise and parts of the subsequent decline. The younger age groups contribute only to the recent decline. The location of the peak associated with the highest mortality from gastric cancer varied among individual countries between 1845 (Switzerland) and 1895 (Japan). In the USA, the cohort-age contours may suggest some plateau of peak around 1845 or earlier, but do not show any initial rise. Overall, the alignment of all the individual cohort-age contours to form one overarching pattern suggests that risk of death from gastric cancer was strongly associated with the period of birth.
The logarithmic scale of the y-axis in figures 1 and 2 allows a comparison of the relative changes of consecutive period-age or cohort-age contours within a single graph. Because the logarithmic scale tends to compress the large changes of death rates among the older age groups and expand small changes among the younger age groups, it emphasises the recent decline at the expense of concealing some of the initial rise. The underlying birth-cohort phenomenon becomes more evident if the individual cohort-age contours are plotted using a linear scale as shown in figure 3. The three countries on top of the graph with the longest cohort-age contours show that the occurrence of an initial rise in mortality from gastric cancer is supported mostly by the trends of the three to five oldest age groups. In the cohort-age contours from Italy and Japan, the initial rise is discernible in the cohort-age contours of the two to three oldest age groups.

Age-specific death rates of gastric cancer plotted as cohort-age contours, linear scale.
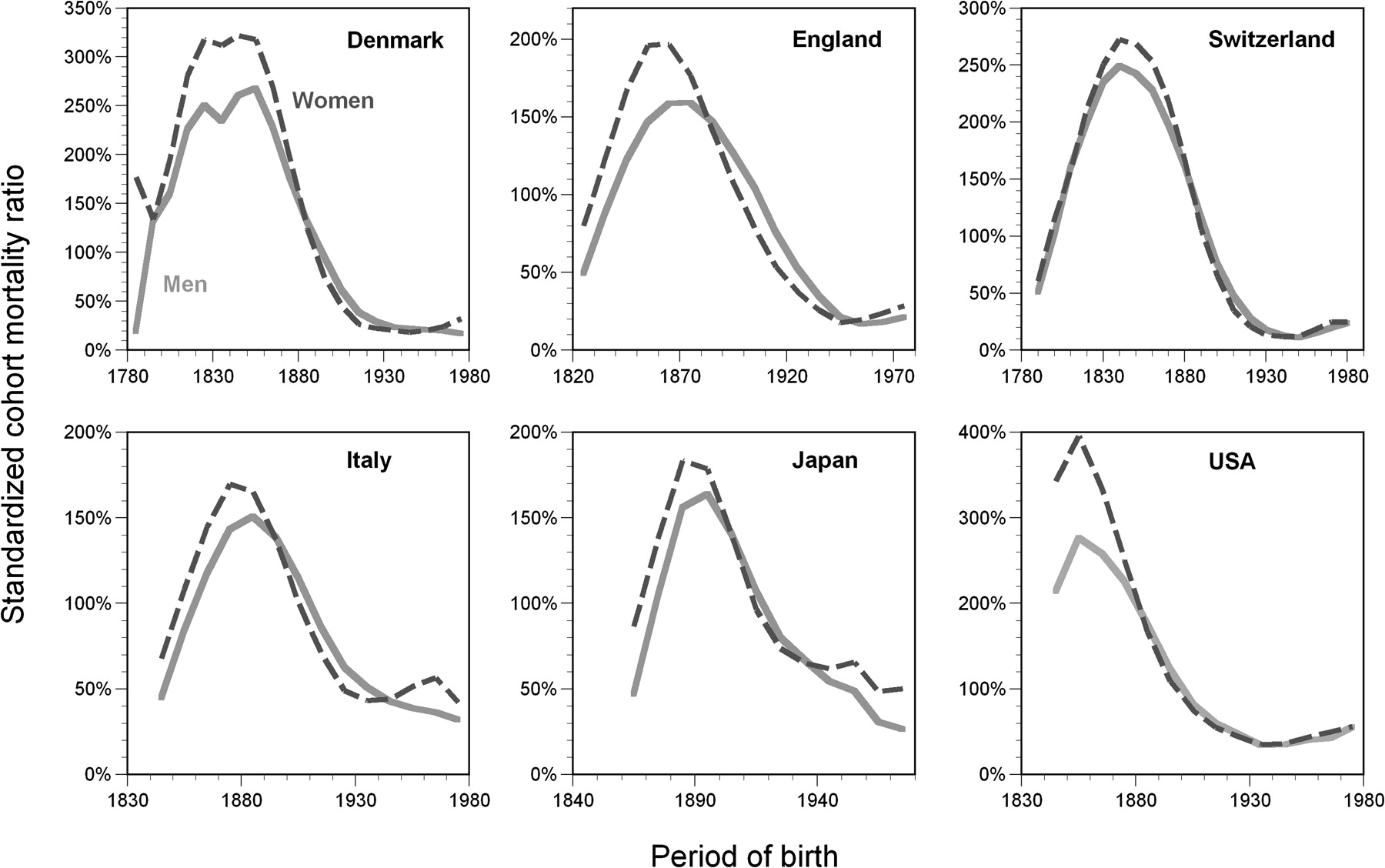
In figure 4, the individual cohort-age contours rates from figure 3 were summarised as the times trends of the age-standardised cohort mortality ratio (SCMR). Figure 4 also contains the SCMR curves of gastric ulcer and duodenal for comparison with gastric cancer. Because the period-age and cohort-age contours of gastric and duodenal ulcer were presented in previous publications, they are not shown in detail in the present analysis.2 3 Every point of the SCMR curves in figure 4 represents an approximation of the average death rate among individuals belonging to different age groups but being born during the same time period. In appreciating the SCMR curves, their temporal behaviour and location of their peaks deserve more attention than the actual height reached by the individual curve. As evidenced by the SCMR curves, mortality from gastric cancer increased among cohorts born during the 18th century until the first half of the 19th century and then declined in all subsequent generations. With the notable exception of Japan, the risk of dying from gastric cancer preceded the risk of dying from either gastric or duodenal ulcer. The time lag between gastric cancer and gastric ulcer varied between 10 years (Italy) and 30 years (Denmark, Switzerland). With the exception of the US gastric cancer data, the differences between the initial value and the peak value of the SCMR were statistically significant with p<0.001. In all countries alike, the differences between the peak value and the final value of the SCMR were also statistically significant with p<0.001 for all comparisons. Figures 1–4 contain the data of men and women analysed together. In all countries alike, very similar temporal patterns of gastric cancer were seen if men and women were analysed separately (figure 5).

Standardised cohort-mortality ratios of gastric cancer (GCA), gastric ulcer (GU), and duodenal ulcer (DU) plotted versus the period of birth.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standardised cohort-mortality ratios of gastric cancer stratified by sex.
Discussion
The present study analysed the times trends of mortality from gastric cancer, gastric ulcer, and duodenal ulcer in four European countries, Japan and the United States. The aim of the analysis was to compare the long-term time trends of gastric cancer with those of ulcer disease and test whether gastric cancer would show a steady plateau before starting to fall secondary to the declining incidence of H pylori infection in the general population. Unexpectedly, the long-term time trends of gastric cancer mortality were found to rise among generations born during the 18th century until the first half of the 19th century and then decline in all subsequent generations. The rise and fall of gastric cancer preceded similar birth-cohort patterns of gastric and duodenal ulcer by about 10–30 years. In spite of the different magnitude of mortality from gastric cancer between men and women, the time trends of gastric cancer were similar in both gender groups.
The general use of mortality data for the comparative analysis of gastric cancer and peptic ulcer may be questioned because, as opposed to gastric cancer, peptic ulcer is associated with only low case fatality rate and mortality appears to capture only a small fraction of the affected patient population. In addition, ascertainment of gastric cancer or peptic ulcer as cause of death may have been incomplete given the limited diagnostic facilities available 50–100 years ago. Two characteristic features of the birth-cohort analysis, however, have to be kept in mind. The analysis by birth cohorts opens a window to extend the analysis of secular trends by 90 years into the past. Although the cohort-age contours stretch far into a distant past, the actual diagnoses of gastric cancer were mostly established during the 20th century. This applies to all age groups alike. For the purpose of the birth-cohort analysis, moreover, the fact that the subjects died from gastric cancer or peptic ulcer is of secondary relevance. Death statistics only help to identify a large group of patients with gastric cancer or peptic ulcer, whose age-specific plots point at a prior time of exposure to environmental risk factors. The important information is contained by the diagnosis and the subject's age. The time of birth carries a specific risk for developing gastric cancer or peptic ulcer. In both instances, this time of birth appears to be a more precise epidemiological parameter than the time of incidence, morbidity or death. It may also be argued that time-dependent improvements in medical diagnosis or management of the three diseases have contributed to the observed time trends. Mortality from gastric cancer, however, is still dismally high, and has improved only marginally in the past century.11 Looking at the period-age contours of gastric cancer (or gastric and duodenal ulcer) with their fan-like appearance, it is difficult to envisage any type of diagnostic tool or therapeutic modality that would have been applied selectively only to younger but not older patients. Moreover, the time trends of gastric and duodenal ulcer shown have been shown to apply similarly to other morbidity parameters.4–7 The sudden surge of the ulcer epidemic in Europe has been well documented in a large variety of autopsy, hospital and outpatient statistics from the 19th century and the beginning of the 20th century.12 The sudden rise in the occurrence of gastric cancer during the 19th century can be similarly appreciated in old hospital statistics from Scotland, England, as well as the United States (A Sonnenberg, unpublished observation 2009).
Gastric cancer, as well as gastric and duodenal ulcer, stem from infection of the upper gastro-intestinal tract with H pylori. The decline in the occurrence of all three diseases throughout the 20th century apparently matched a similar decline of infection with H pylori in the general population.13 If all three diseases are related to H pylori, however, why were they characterised by strikingly different time trends among consecutive generations born during the 19th century? Acquisition of H pylori infection soon after birth predisposes to life-long gastritis and gastric cancer at old age. It has been speculated that a shift of first acquisition of H pylori towards later childhood predisposed to gastric ulcer, whereas even later acquisition during or after adolescence was more likely to result in duodenal ulcer.14 15 Historically, as the infection with H pylori decreased among the populations of Western countries, the age of first acquisition may have shifted towards older age groups with a concomitant increase in susceptibility to develop subsequent peptic ulcer disease. Whereas gastric gastritis and gastric atrophy developed mostly in subjects who contracted the infection with H pylori as toddlers, preserved acid secretion in subjects who contracted H pylori later in life, made infected subjects more susceptible to subsequent peptic ulceration. The superimposition of a falling infection rate and a rising fraction of subjects with age-delayed infection could have increased ulcer susceptibility and resulted in the rising and falling trends of gastric and duodenal ulcer as evidenced by their birth-cohort pattern.15 The earlier peak of gastric than duodenal ulcer would be consistent with the younger age, at which first infection occurs in gastric than duodenal ulcer patients.
The age delay in infection with H pylori was assumed to play a role only in the pathogenesis of peptic ulcer, but not gastric cancer. In comparison with gastric and duodenal ulcer, the time trends of gastric cancer appeared to be linked more directly to the underlying time trends of H pylori. This theory hinged in part, however, on the absence of an initial rise in the alignment of cohort-age contours associated with gastric cancer. The time trends of gastric cancer mortality in the USA seemingly supported such contention.8 Similarly, the study of time trends of gastric cancer mortality in various European countries, such as Germany or France, during to the past 50 years failed to show anything but a parallel decline in the age-specific death rates of gastric cancer, when similar analyses of gastric or duodenal ulcer mortality already revealed a clear-cut rise and fall (A Sonnenberg, unpublished observation 1989). The data from Japan are exceptional in showing a peak in mortality associated with gastric cancer among birth cohorts born as late as the end of the 19th century. In most other countries reliance has to be placed on far-reaching historical data to tease out the initial rise in gastric cancer risk hidden in a distant past. Although the study relies mostly on mortality data generated during the 20th century, the analysis by birth-year opens a window of opportunity to study the time trends among cohorts born during the early 19th century.
At the present time, the reasons for the initial rise in the occurrence of gastric cancer remain mysterious. The rise cannot be explained by the increased ageing of the population, because the rise is discernible in the individual cohort-age contours, which are based on the age-specific experience of identical age groups during consecutive time periods. It could possibly relate to temporal changes associated with H pylori infection or varying exposure to other environmental risk factors. H pylori infection could have been rising among the urban populations during the period of industrialisation in the late 18th and early 19th centuries. Individuals may have been suddenly exposed to many different strains and become infected by more than one strain of H pylori. New types of H pylori species may have spread through the population with a higher risk for causing gastric cancer or peptic ulcer.16 The similarity in the rise and fall of the birth-cohort patterns of gastric cancer, gastric ulcer and duodenal ulcer, albeit shifted by several decades on the time axis, could also suggest some shared environmental influence affecting all three diagnoses in sequence. Multiple previous studies have identified salt consumption as a risk factor for gastric cancer, as well as peptic ulcer.17–19 After the abolition of the excessively high salt taxes in Europe during the late 18th and early 19th century, salt consumption increased in most European populations.20 21 Presently, however, there are few if any reliable historical statistics to assess such potential associations quantitatively.
The presence of three birth-cohort phenomena underlying the time trends of gastric cancer, gastric ulcer and duodenal ulcer is difficult to ignore or discount as some minor fluke of epidemiological analysis. It shows up repetitively and consistently in many types of health statistics and is discernible in the data from a variety of different countries. The general relevance of the birth-cohort phenomenon of gastric cancer and peptic ulcer is 2-fold. First, its very existence points at the profound influence of some yet unknown and important environmental risk factor on the occurrence of these common digestive diseases. Second, as long as the mechanisms underlying the surging epidemics of gastric cancer und peptic ulcer during the 19th century remain poorly understood, a risk persists that such epidemics may re-occur, especially in countries where large fractions of the population still harbour H pylori.
In conclusion, the present analysis reveals that the time trends of mortality from gastric cancer are shaped by an underlying birth-cohort pattern that resembles similar patterns of ulcer mortality. Whereas the birth-cohort pattern of peptic ulcer is characterised by a distinctive rise and fall with its peak located around the turn of the 19th century, the cohort pattern of gastric cancer shifted in time towards earlier generations born around or shortly after the mid 19th century. The occurrence of varying birth-cohort phenomena for gastric cancer, gastric ulcer and duodenal ulcer are difficult to explain based alone on changes in the infection rate with H pylori. The birth-cohort patterns suggest that in addition to changes in the infection rate other mechanisms must have contributed to the peculiar long-term behaviour of these three diagnoses.
Significance of this study
What is already known about this subject?
The incidence of gastric cancer and peptic ulcer has fallen dramatically in all Western countries
This fall has been ascribed to the declining infection of the general population with H pylori
The time trends of both gastric and duodenal ulcer are known to be influenced by an underlying birth-cohort pattern
What are the new findings?
The long-term time trends of gastric cancer mortality were found to rise among generations born during the 18th century until the first half of the 19th century and then decline in all subsequent generations
The rise and fall of gastric cancer preceded similar birth-cohort patterns of gastric and duodenal ulcer by about 10–30 years
These time trends of gastric cancer were similar in men and women
How might it impact on clinical practice in the foreseeable future?
The very existence of the birth-cohort phenomenon points at the profound influence of some yet unknown and important environmental risk factor on the occurrence of these common digestive diseases
As long as the mechanisms underlying the surging epidemics of gastric cancer und peptic ulcer during 19th century remain poorly understood, a risk persists that such epidemics may re-occur, especially in countries where large fractions of the population still harbour H pylori
Acknowledgments
The author is indebted to following group of people who have greatly helped him in accumulating the statistical data: Lisbeth Ingeborg Kristensen at Statistics Denmark Library and Information, Denmark; Liam Beardsmore at the Office for National Statistics, England; Erwin K. Wüest at the Eidgenössisches Departement des Innern, Bundesamt für Statistik, Switzerland; Antonella Ciccarese at the Istituto Nazionale di Statistica, Italy; Aya Yamazaki and Yoko Kanegae at Statistics and Information Department, Ministry of Health, Labour and Welfare, Japan.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.