Article Text

Abstract
Background: Minichromosome maintenance (Mcm) proteins are essential for eukaryotic DNA replication, and their expression implies potential for cell proliferation. Expression is dysregulated in dysplastic states but data for oesophageal squamous mucosa and Barrett's mucosa have not been published.
Aim: To test the hypothesis that Mcm proteins are downregulated together with the proliferation marker Ki-67 in differentiating epithelial compartments of non-dysplastic squamous and Barrett's epithelium, and that this process does not occur in dysplastic mucosae.
Methods and cases: Forty five patients with Barrett's oesophagus included 20 with glandular dysplasia (10 low grade, eight high grade, two both, and four with invasive adenocarcinoma). Twenty five other patients included 12 with oesophageal squamous dysplasia (three low grade, six high grade, three both, and four with invasive squamous carcinoma). Formalin fixed paraffin embedded tissue sections from biopsy series and resections were immunostained using antibodies to Mcm2, Mcm5, and Ki-67. Percentage of nuclei positive for Mcm2, Mcm5, and Ki-67 was estimated and scored from 0 to 6 as: 0, none +; 1, <10%+; 2, 10–30%+; 3, 30–70%+; 4, 70–90%+; 5, >90%+; 6, all+. Four separate epithelial strata were scored: in squamous epithelium the basal layer and thirds to the surface, in Barrett's mucosa the luminal surface, upper and lower crypt, and deep glands.
Results: In non-dysplastic squamous epithelium and Barrett's mucosa, high level expression of Mcm2, Mcm5, and Ki-67 proteins was largely confined to the proliferative compartments and downregulated in differentiated compartments. Expression persisted up to the mucosal surface in dysplastic squamous epithelium and Barrett's mucosa.
Conclusions: Persistent expression of Mcm2, Mcm5, and Ki-67 proteins in luminal compartments of dysplastic oesophageal squamous epithelium and dysplastic Barrett's mucosa may be diagnostic markers and imply disruption of cell cycle control and differentiation in these dysplastic epithelia.
- Barrett's oesophagus
- minichromosome maintenance proteins
- oesophageal cancer
- oesophageal squamous epithelium
- Mcm proteins, minichromosome maintenance proteins
- pre-RCs, pre-replicative complexes
- mAb, monoclonal antibody
Statistics from Altmetric.com
- Barrett's oesophagus
- minichromosome maintenance proteins
- oesophageal cancer
- oesophageal squamous epithelium
- Mcm proteins, minichromosome maintenance proteins
- pre-RCs, pre-replicative complexes
- mAb, monoclonal antibody
Lethality of symptomatic oesophageal cancer motivates screening1–,3 for earlier disease, treatable by surgical resection or mucosal ablation by laser,4 argon beam,5 or photodynamic therapy.6 Population screening for squamous oesophageal carcinoma is only practised where the incidence is high (for example, Japan and China). Dysplasia and carcinoma surveillance by endoscopy and biopsy of Barrett's patients in Western populations is also undertaken, but with uncertain benefit.7 It is a substantial commitment, rigorous definition of Barrett's dysplasia is difficult, and inter- and intra-pathologist agreement is imperfect.8, 9 Even four quadrant sampling with jumbo biopsy forceps does not guarantee that all significant dysplasia will be detected,10 and the natural history of oesophageal glandular dysplasia is obscure.
Abnormal proliferation and differentiation typify epithelial dysplasia. Normal oesophageal squamous epithelial cells divide slowly in the basal layer, proliferate suprabasally, and mature towards the luminal surface.11 In Barrett's mucosa, despite its partially intestinal phenotype, proliferation and differentiation patterns resemble gastric mucosa, with maximal proliferation in a crypt zone beneath the mucosal surface12 and differentiation into deep glands and characteristic cell populations on the mucosal surface (in normal small intestine, stem cells in the crypts of Lieberkühn feed a proliferative compartment from which differentiating enterocytes and goblet cells migrate to the villi11 while Paneth cells migrate basally).
Proliferation and differentiation compartments break down in dysplastic epithelia. “Dysplastic” cells adjacent to an invasive carcinoma probably represent the neoplastic clone from which the carcinoma emerged. Dysplasia alone implies an increased cancer risk, and motivates eradication or increased intensity of surveillance. Difficulty in reliably recognising and grading dysplasia is therefore therapeutically relevant, and improved methods for doing so are desirable.
In eukaryotic cells, initiation of DNA synthesis at specific sites (origin firing) is tightly restricted to permit duplication of the genome once only per cell cycle.13 Initiation factors including the origin recognition complex, Cdc6,14 and minichromosome maintenance (Mcm) proteins which assemble during G1 into pre-replicative complexes (pre-RCs) at replication origins to establish competence for DNA replication in S phase. Activated Cdc7/Dbf4 kinase14 and S phase promoting cyclin dependent kinases trigger unwinding of replication origins and establish bidirectional replication forks, and disassembly of pre-RCs during replication prevents reinitiation of DNA replication within a single cycle.
When mammalian cells exit the cell cycle into quiescent, differentiated, and senescent states, the Cdc6 and Mcm components of the pre-RCs are downregulated,15, 16 and dysregulated expression of these proteins is characteristic of both dysplastic cervical squamous epithelium16 and urothelium.17 It seemed appropriate therefore to evaluate their potential as markers of dysplasia and dysregulated cell cycle control in normal oesophageal squamous epithelium, Barrett's mucosa without dysplasia, and in their dysplastic and neoplastic counterparts.
MATERIALS AND METHODS
Production of antibodies
Anti-Mcm2 monoclonal antibody (mAb) (mouse IgG1 isotype) was raised against a fragment of human Mcm2 (amino acids 725–888; BM28, Transduction Laboratories, Lexington, Kentucky, USA). The specificity of the anti-Mcm2 mAb was established by immunoblot, immunofluorescence, and immunoprecipitation assays. Rabbit polyclonal antibodies were raised against a fragment of human Mcm5 (amino acids 372–590) and purified by affinity chromatography over a column prepared by linking the immunogen to Sulfolink Gel (Pierce, Rockford, Illinois, USA). Specificity of anti-Mcm2 mAb and anti-Mcm5 polyclonal antibody was established by immunoblot, immunofluorescence, and immunoprecipitation assays. The anti-Ki-67 mAb MIB1 was supplied by Dako (Ely, Cambridge, UK).
Immunohistochemistry
Preliminary testing of six different antibodies at different dilutions and antigen retrieval schedules including enzymatic digestion and microwave heating in citrate and EDTA buffer was performed on formalin fixed paraffin embedded tissue sections. Good results were obtained with antibodies against Mcm proteins 2 and 5 using EDTA buffer and microwave heating antigen retrieval. Both Mcm antibodies were used diluted 1:4000 and conventional three stage streptavidin/biotin and peroxidase with diaminobenzidine/H202 detection. Antibody MIB1 was applied diluted 1:100 following microwave antigen retrieval and detected as for Mcm2/Mcm5.
Cases
Seventy patients were studied. Twenty five patients without Barrett's oesophagus included 13 with no squamous dysplasia, three with low grade squamous dysplasia, six with high grade squamous dysplasia, and three with both. Four patients in this group also had invasive squamous carcinoma. Forty five patients with Barrett's oesophagus included 25 without dysplasia, 10 with low grade glandular dysplasia, eight with high grade dysplasia, and two with both. Four patients in this group also had invasive adenocarcinoma.
Patients were from cohorts undergoing diagnostic endoscopy for upper gastrointestinal symptoms, enrolled in a yearly surveillance of Barrett's oesophagus, or having surgical resection of oesophageal carcinoma. Dysplastic changes were assessed on haematoxylin and eosin stained sections of paraffin embedded endoscopic biopsies and tissue blocks from resection specimens which were chosen from pathology department archives to represent a range of morphologies from normal (non-dysplastic) oesophageal squamous epithelium through low and high grade squamous dysplasia to invasive squamous carcinoma. Similarly, examples of Barrett's mucosa without dysplasia, low grade and high grade dysplasia in Barrett's mucosa, and invasive Barrett's adenocarcinoma were selected for study, and 4 μm sections were immunostained as described.
Scoring immunocytochemistry
A semiquantitative scoring scheme was designed to describe the immunostaining observed. Cell nuclei were positive or negative for Mcm2, Mcm5, or Ki-67. All scoring was done by one specialist upper gastrointestinal pathologist (JJG). Within each separate mucosal compartment, the estimated percentage of positive cells was allocated to scoring bands as follows: 0, none+; 1, <10%+; 2, 10–30%+; 3, 30–70%+; 4, 70–90%+; 5, >90%+; and 6, all+. Four compartments were recognised in oesophageal squamous epithelium: the most basal single layer of cells, and the thickness of the epithelium above that divided into parabasal, middle, and luminal thirds. In Barrett's mucosa, four strata again were defined: the surface epithelium between “crypts”, the underlying “crypts” or “pits” divided into upper and lower halves, and the deepest layer, a differentiated glandular zone. These compartments correspond to those defined by Lauwers and colleagues18 in their study of cell proliferation in Barrett's mucosa.
Reproducibility of scoring and statistical analysis
Reproducibility of scoring was evaluated by “blind” re-scoring by JJG of all sections stained for Mcm2 after six months. Weighted kappa κw19 was calculated for duplicate scores from 562 separate cellular populations; κw=0.65 implied acceptable agreement. Univariate statistical significance of differences between immunostaining was tested using the non-parametric Mann-Whitney test for two independent samples, two tailed, with correction for ties. Kappa and Mann-Whitney calculations were performed in Analyse-It for Microsoft Excel (Analyse-It Software, Leeds, UK).
RESULTS
Immunostaining with the Mcm2 antibody yielded predominantly nuclear staining. The Mcm5 antibody stained nuclei but also cell membranes in glandular mucosae and tumours. Qualitatively, nuclear staining was similar with the two antibodies. Ki-67 staining was purely nuclear.
In non-dysplastic squamous epithelium and Barrett's mucosa, strong Mcm2, Mcm5, and Ki-67 staining of most to all nuclei was present in the expected proliferative transit compartment—that is, the suprabasal compartment of squamous epithelium—and in the lower crypt compartment of Barrett's mucosa. In differentiated compartments—that is, the surface of squamous epithelium and Barrett's mucosa—and in the small differentiated deep glands of Barrett's mucosa, expression was downregulated. In dysplastic squamous epithelium and dysplastic Barrett's mucosa there was persistence of Mcm2, Mcm5, and Ki-67 expression in compartments in which they are normally absent or sparse, especially towards the surface of squamous epithelium and Barrett's mucosa. Downregulation of Mcm2 and Mcm5 expression in the deep (glandular) mucosal compartment of Barrett's mucosa was also significantly reduced in high grade dysplasia. These relationships are illustrated in figs 1 and 2⇓⇓ which plot median, quartiles, and range for Mcm2, Mcm5, and Ki-67 staining scores for the various compartments of oesophageal squamous (fig 1⇓) and Barrett's mucosa (fig 2⇓). Photomicrographs illustrate these staining patterns (fig 3A–C⇓ for Barrett's mucosa and fig 4A, B⇓ for squamous epithelium). Statistical testing confirms that overexpression of these markers in the surface and subsurface compartments of dysplastic squamous and Barrett's mucosa is significant at a high level of probability (table 1⇓).
p values by Mann-Whitney testing of the differences between groups

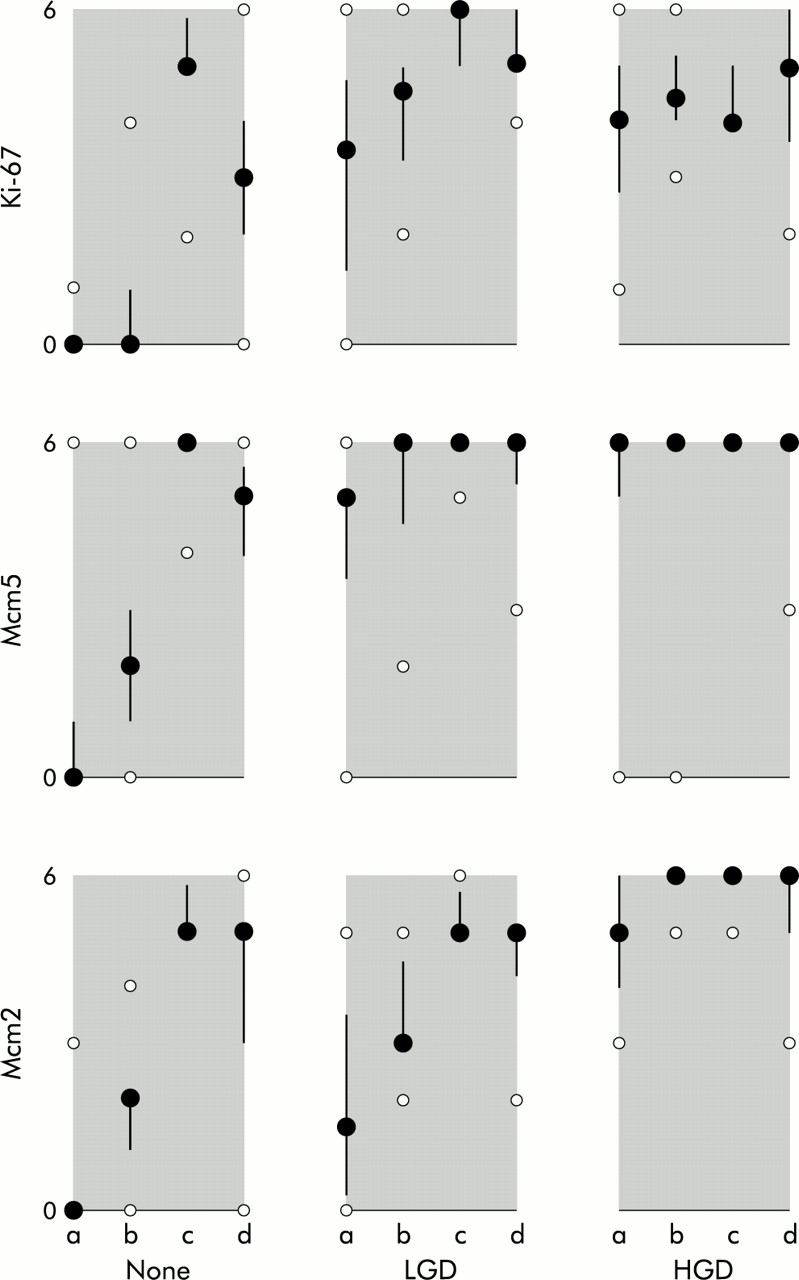
Graphs of minichromosome maintenance protein (Mcm) and Ki-67 expression in oesophageal squamous epithelium: quartile plots of immunohistochemical scores (range 0–6) for Ki-67, Mcm5, and Mcm2 (rows 1–3). Columns from left to right represent squamous epithelium without dysplasia (none), low grade dysplasia (LGD), and high grade dysplasia (HGD). Epithelial layers are represented as a–d with a=basal; b=suprabasal, lower third; c=suprabasal, middle third; and d=suprabasal, upper third. Filled dots represent medians, bars interquartile range, and small open dots the range.

Graphs of minichromosome maintenance protein (Mcm) and Ki-67 expression in Barrett's mucosa: quartile plots of immunohistochemical scores (range 0–6) for Ki-67, Mcm5, and Mcm2 (rows 1–3). Columns from left to right represent Barrett's mucosa without dysplasia (none), low grade dysplasia (LGD), and high grade dysplasia (HGD). Mucosal layers are represented as a–d with a=deep glands; b=lower crypt; c=upper crypt; and d=mucosal surface. Filled dots represent medians, bars interquartile range, and small open dots the range.

Minichromosome maintenance protein 2 (Mcm2) expression in Barrett's mucosa. On the right of (A), non-dysplastic intestinal type “specialised” Barrett's mucosa shows Mcm2 expression in cells of the proliferative zone beneath the mucosal surface. Expression falls away markedly on the mucosal surface. There is an abrupt transition (arrow) to mucosa showing mild (low grade) dysplasia in which Mcm2 downregulation does not occur. More pronounced but still low grade Barrett's dysplasia (B) shows strong Mcm2 expression in the upper crypt and surface, with weaker expression in deep glands.
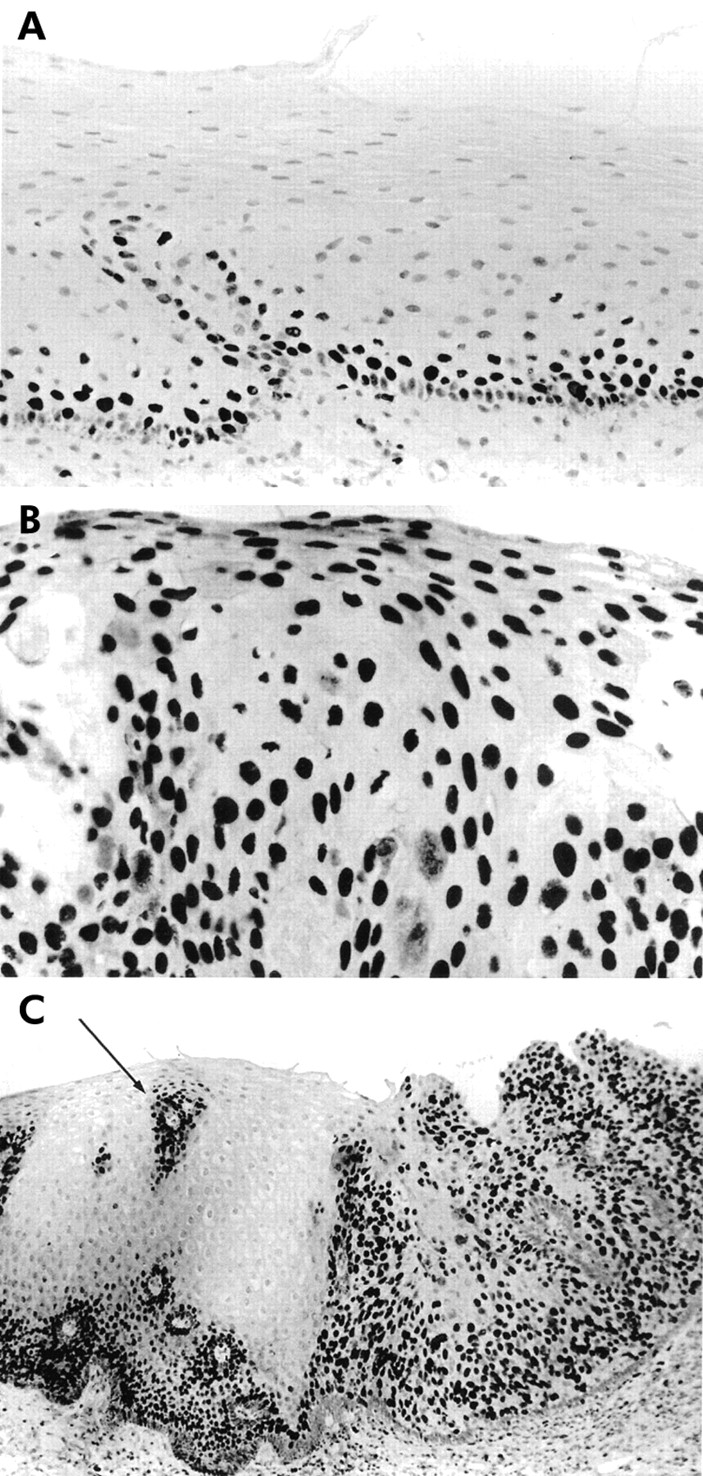
Minichromosome maintenance protein 2 (Mcm2) expression in oesophageal squamous epithelium. In normal squamous epithelium (A), maximal expression immediately above a well defined basal layer falls to undetectable levels in the upper third (top). In low grade dysplasia (B), detectable Mcm2 persists to the luminal surface. In (C), there is an abrupt transition between high grade squamous dysplasia (right) and morphologically normal oesophageal squamous epithelium (left). The apparent “island” of Mcm2 expression (small arrow) in the normal epithelium represents tangential sectioning of a submucosal papilla.
Although abnormally persistent expression of Mcm2, Mcm5, and Ki-67 is clearly associated with premalignant dysplasia in oesophageal squamous epithelium and Barrett's mucosa, variant patterns were identified. The dysplastic squamous epithelium in fig 5A⇓ clearly downregulates Mcm2 expression towards the surface, and in the same case Mcm2 downregulation occurs in invasive squamous carcinoma towards the centre of cell nests—that is, in areas of differentiation (fig 5B⇓). Similarly, viable but Mcm2 and Mcm5 negative cells were present in invasive adenocarcinomas (fig 6⇓).

Downregulation of minichromosome maintenance protein 2 (Mcm2) with differentiation in dysplastic and neoplastic squamous epithelium. In (A), full thickness squamous dysplasia with Mcm2 expression up to the mucosal surface (on the left of the picture) is associated with a basaloid phenotype. On the right, marked nuclear atypia persists to the mucosal surface but cells towards the surface have more cytoplasm and this morphological change is associated with loss of detectable Mcm2. Similarly, in a moderately differentiated invasive oesophageal squamous carcinoma (B), many carcinoma cells are Mcm2 positive but viable Mcm2 negative carcinoma cells are present within cell nests with morphological features of differentiation (keratinisation).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Minichromosome maintenance protein 2 (Mcm2) expression in an oesophageal adenocarcinoma. This carcinoma was in a Barrett's oesophagus. Malignant glandular acini invade muscularis propria. Most of the carcinoma cells are Mcm2 positive but viable Mcm2 negative carcinoma cells are also present.
DISCUSSION
Our data document spatial organisation of cell proliferation in normal oesophageal squamous epithelium and non-dysplastic Barrett's mucosa, and disruption of this highly organised spatial arrangement in premalignant dysplasia. These disturbances are relevant to the identification of dysplasia in oesophageal squamous epithelium and Barrett's mucosa, both of which are problematic in individuals and populations. Squamous oesophageal cancer is a target for screening in Far Eastern populations. Barrett's oesophagus and Barrett's cancer are relatively common in the West. Patients with Barrett's oesophagus may be subjected to relatively frequent endoscopy and biopsy (for example, yearly). A sensitive and specific test for dysplasia might allow Barrett's patients to be screened for dysplasia and divided into a cohort without dysplasia, at low risk of oesophageal adenocarcinoma, for whom less intensive follow up would be safe, and a higher risk group, with dysplasia, for whom more frequent endoscopic and biopsy surveillance could be appropriate. A sensitive test for early dysplastic changes in endoscopic biopsies would be useful to the pathologist although to date various tests that have been proposed have been disappointing in practice.
Abnormal expression of Mcm5 protein in dyskaryotic cervical smears is associated with cervical intraepithelial neoplasia, and immunocytochemistry for Mcm5 protein facilitates detection of dyskaryotic cells in such smears, which may otherwise be a problem if they are present in small numbers.16 Similarly, biochemical assay of these proteins in urine is a sensitive and specific test for the presence of urothelial epithelial neoplasia.17 These examples and the present study support the use of Mcm proteins (and Ki-67) as markers of dysplasia. These studies in cervix, bladder, and oesophagus support the concept that persistence of Mcm protein expression in dysplastic epithelia is associated with preneoplastic cells locked in the cell cycle (confirmed by persistence of Ki-67 expression) compared with normal epithelial cells that exit the cell division cycle during maturation and differentiation.
A problem in Barrett's surveillance is that dysplastic changes may be very focal, and biopsy series may not sample dysplasia, even if large biopsy forceps are used systematically.10 Aberrant superficial expression of Mcm2, Mcm5, and Ki-67 proteins by dysplastic Barrett's mucosa suggests that exfoliative cytology could be used to sample more widely than biopsy procedures. Brush cytology could be directed at endoscopy or a balloon cytology catheter employed to collect cells from the mucosal surface.3, 20 Balloon cytology does not require endoscopy. Sampled cells could be evaluated by immunohistochemistry or biochemically. The data presented here justify critical prospective evaluation in an appropriate clinical setting of Mcm proteins as candidate markers of dysplasia and cancer risk in squamous and columnar lined oesophagus.
Although persistence of Mcm2 and 5 proteins in differentiating compartments of dysplastic squamous oesophageal epithelium and Barrett's mucosa is characteristic, it is not invariable. Downregulation can occur in surface cells overlying clearly atypical cells of squamous and glandular mucosae. These surface cells may themselves appear atypical, or relatively normal in morphology. One interpretation of this appearance is the biologically trivial one that the morphologically normal cells may appear to be related to the underlying cells only as a consequence of vagaries of the plane of section in randomly orientated mucosal biopsies. Histological interpretation of Barrett's dysplasia routinely requires this to be taken into account. However, our own data show that even in invasive carcinomas, molecular events associated with differentiation appear capable of switching off Mcm protein expression. These findings support the concept of mutual antagonism between the cellular circuits controlling differentiation and proliferation. As this would usually be understood to prevent further cell division, such events may have therapeutic relevance.
Acknowledgments
GHW is supported by a CRC Senior Clinician Scientist Fellowship and KS by an MRC Research Studentship and John Lucas Walker Senior Scholarship.