Article Text

Abstract
Background and aim: Despite the fact that bowel ultrasound (US) has recently been proved to be useful in the assessment of bowel diseases, uncertainty persists as to its diagnostic role in patients with complicated Crohn's disease (CD). Therefore, we have prospectively investigated the accuracy of US compared with x ray procedures and intraoperative findings in detecting small bowel strictures complicating CD as well as its reliability in assessing disease extent and location within the bowel.
Methods: A series of 296 consecutive patients with proven CD admitted to L Sacco University Hospital between 1997 and 1999, having undergone complete radiographic evaluation (including small bowel x ray, colonoscopy, or double contrast barium enema), were enrolled in the study. Bowel US was performed in each patient by two experienced operators unaware of the results of other diagnostic procedures. The accuracy of US in detecting strictures compared with x ray studies was determined separately in two different groups of patients: 211 patients treated conservatively (non-operative CD) and 85 patients who were candidates for surgery for CD complications or unresponsiveness to medical therapy (operative CD).
Results: Overall sensitivity and specificity of US in assessing the anatomical distribution of CD were 93% and 97%, respectively. The extent of ileal disease measured at US correlated well with that determined by x ray (r=0.52, p<0.001) in medically treated patients as well as with that measured intraoperatively in surgical patients (r=0.64, p<0.001). One or more stenoses were detected in 75 patients (35.5%) at small bowel enteroclysis in the non-operative CD group compared with 70 (82%) in the operative CD series. Sensitivity, specificity, and positive predictive values of bowel US in the detection of strictures were 79%, 98%, and 95% in non-operative CD patients and 90%, 100%, and 100% in operative CD cases, respectively.
Conclusions: In experienced hands, bowel US is an accurate technique for assessing CD extent and location and is very helpful in detecting small bowel strictures, especially in very severe cases that are candidates for surgery. The use of bowel US is therefore justified as a primary investigation in CD patients in whom complications are suspected.
- bowel ultrasound
- Crohn's disease
- small bowel strictures
- barium x rays
- surgery
- CD, Crohn's disease
- CDAI, CD activity index
- US, ultrasound
- BWT, bowel wall thickness
Statistics from Altmetric.com
Bowel stricture of clinically significant importance is a common intestinal complication of Crohn's disease (CD), occurring at some time during the natural course of the disease in approximately 50% of affected patients.1–3 Although its presence is usually heralded by specific complaints, it is sometimes difficult to diagnose on clinical grounds as symptoms may be inconspicuous or masked by the effects of steroids. Barium studies or endoscopy are therefore required to detect this complication although their reported sensitivity may vary from study to study depending on the type of technique used (that is, small bowel enema or conventional barium follow through4,5), anatomical location, and degree of stenoses,6 as well as disease severity.7
Despite the fact that bowel ultrasound (US) has been proved to be an important diagnostic tool in patients with CD, allowing clear visualisation of the bowel segment involved,8–12 its role in the detection of abdominal complications of CD remains controversial as the few studies, mostly retrospective, carried out to date have given rise to conflicting results.13 Furthermore, strictures and abscesses are often considered to be more easily detectable at US than fistulas, albeit contrasting data exist even on this point.14,15 Surprisingly, to date, no large prospective study has been performed to evaluate the reliability of bowel US in detecting intestinal strictures complicating CD in comparison with conventional x ray techniques. The role of this procedure moreover compared with that of other conventional imaging methods and intraoperative findings in localising and assessing the anatomical extent of intestinal CD remains to be fully determined.
The primary aim of this prospective study was therefore to investigate in a large series of consecutive hospitalised patients with complicated and uncomplicated CD, submitted to complete radiographic evaluation of the intestinal tract, the accuracy of bowel US in detecting small bowel strictures. The study also aimed to establish the possible role of bowel US in assessing the extent and anatomical location of CD.
PATIENTS AND METHODS
Patients
Consecutive CD patients admitted to the Department of Gastroenterology of L Sacco University Hospital between February 1997 and November 1999 were invited to take part in this prospective study. Diagnosis of CD was achieved in all patients using standard criteria16 and the site, as well as the anatomical extent, of the disease was established on total colonoscopy findings (or double contrast barium enema if colonoscopy was not successful) and small bowel enteroclysis. The criteria for admission to the study also required that patients were over 18 years of age, and had adequate medical records of clinical, anatomical, and therapeutic characteristics of the disease. In particular, details were sought concerning duration of disease as well as initial diagnosis, previous surgery, number of recurrences, and current and previous medical treatments. In addition, disease activity was assessed on admission to the study using the CD activity index (CDAI17). Patients were excluded from the study if they had only anorectal or gastroduodenal localisation of the disease (as the low accuracy of US in detecting these CD localisations is well known18).
Methods
In accordance with the study protocol, US was performed in all patients as the first diagnostic procedure, followed by endoscopy and radiographic evaluations.
US evaluation
Bowel US was performed by an experienced operator (FP or GM) who was unaware of the results of previous diagnostic procedures but was informed concerning the diagnosis of CD and any previous surgical resection. Both sonographers had experience exceeding >5000 sonographic examinations of the whole abdomen and had reached an educational level ranging from >2000 to >4000 examinations of the bowel. Sonographic scan of the whole abdomen was carried out with a real time ultrasonic apparatus (Hitachi, EUB 525, Tokyo, Japan). The examination was commenced with a convex 3.5 MHz transducer and then, for detailed evaluation, a linear 7.5 MHz transducer was used. No special preparation such as fasting, administration of spasmolytic agents, or water instillation into the bowel was deemed necessary. As previously reported,11 intestinal wall thickness of ≥4 mm was considered pathological provided that it could be measured both in longitudinal and transverse sections and it could be reproduced for at least 4 cm in length. In patients in whom more than one segment was involved, the maximum bowel wall thickness (BWT) was used. Stenosis was considered present when US revealed coexistence of thickened and stiff bowel wall, narrowing of the intestinal lumen together with distended fluid, or echogenic content filled loops just above the thickened bowel segment, as described elsewhere.13 The morphology and location of bowel wall thickening, mesenteric masses, or strictures were documented. The presence of other abdominal complications detectable at US such as internal fistulas and abscesses was also recorded, although the latter complications are not specifically considered in this report as they have been dealt with elsewhere. Stomach, rectum, and the distal part of the sigmoid colon were not evaluated as the low accuracy of US in detecting CD lesions in these areas is well known.
X ray studies
Small bowel enteroclysis was carried out in all patients using the double contrast technique, the barium suspension being introduced directly into the distal duodenum or proximal jejunum through an oral tube. Approximately 120–160 ml of diluted barium suspension were injected into the small bowel under fluoroscopy. After this, 1500–2000 ml of aqueous suspension of methylcellulose were slowly infused through the oroduodenal tube until the entire small bowel was clearly visible in double contrast. Compression spot filming of the entire small bowel was then carried out and radiographs in the prone, supine, and oblique positions were taken. Small bowel abnormalities with particular reference to disease length (expressed in cm), number and site of strictures, and fistulas were reported on a specific chart at the end of each study.
Patients in whom the examination was not feasible (that is, due to severe clinical conditions), those who were unable to pass the oral tube into the duodenum or could not tolerate intubation, underwent small bowel follow through but were excluded from the study. Small bowel enemas were performed by radiologists with specific experience in this type of examination and who were unaware of the results of bowel US.
Some patients with ileocolonic anastomosis also underwent conventional double contrast barium enema which however was not taken into consideration as the reference standard for ileal stenosis.
Surgery
The decision to operate was taken jointly by a gastroenterologist and a surgeon, on the basis of clinical symptoms, laboratory results, and imaging studies, independently of the US findings. In the CD operative series, the results obtained at surgery were taken as the reference standard for determining disease location and extension but not for the presence of strictures (see below). Surgery was performed by surgeons with specific experience in CD surgery who compiled a special form at the end of each procedure. At laparotomy, the bowel was carefully examined by the surgeon from the ligament of Treitz to the upper rectum. If adhesions were present, a complete lysis was made and CD complications (strictures, abscesses, and fistulas) were specifically sought. Bowel strictures were diagnosed in cases of significant luminal narrowing and bowel wall thickening, with or without prestenotic dilatation. If the surgeon decided on a minimal bowel resection (namely, a resection without macroscopically disease free margins, performed in the presence of a fistula arising from and/or an abscess located close to the stenotic segment), careful examination of the specimens was performed at the end of the procedure, using a 14 Ch Fooley's catheter to probe the residual lumen and the bowel extensibility. If a bowel sparing procedure was chosen using the Heineke-Mikulicz technique or by performing an ileocaecal or ileoileal side to side, or ileocolic side to side stricturoplasty, as previously described,19,20 the bowel loop was probed, through an enterotomy, downstream and upstream of the stenotic segment. The stenosis was considered severe if the catheter could not or could probe the lumen but it was impossible to blow up the balloon (Ø≅5 mm); moderate if probing was successful with the balloon blown up with 2.5 ml of saline solution (Ø≅15 mm); and absent if the probing was feasible with a 5 ml inflated balloon (Ø≅20 mm).
The study was approved by the L Sacco Hospital Ethics Committee and written informed consent was obtained from all patients before entering the study.
Statistical analysis
We performed χ2 analysis and the Student's t test for unpaired samples, where appropriate, for comparisons between the two groups. Correlation between US and radiographic extent of ileal disease was assessed by Pearson's correlation coefficient. Regarding the accuracy of US in detecting strictures, the results of US and x ray procedures were analysed on a per patient basis. Therefore, a result was considered to be truly positive when at least one stricture, identified at US, was matched to a lesion seen at small bowel enteroclysis. We did not evaluate the accuracy of US in the detection of all strictures but each patient was simply classified as a carrier of small bowel stenosis if at least one of these lesions was revealed at x ray.
RESULTS
Of the 299 CD patients who fulfilled all admission criteria and were initially enrolled, 296 (99%) had US findings consistent with CD and were therefore included in the data analysis. Eighty five of these (28%) underwent surgery, constituting the operative CD series and were further evaluated at laparotomy, whereas the remaining 211 underwent medical treatment (non-operative CD group). Of the three US negative patients who fulfilled the remaining criteria for admission to the study, one had very mild ileal disease (with few aphthoid ulcers) while two showed superficial and limited recurrence of CD at colonoscopy in the neoterminal ileum.
Demographic, clinical, and biological parameters, as well as US findings, of these two study groups are given in table 1.
Clinical, biochemical, and ultrasonographic parameters of the 211 Crohn's disease (CD) patients undergoing conservative management (non-operative CD) and 85 patients requiring surgery (operative CD)
Accuracy of US in localising CD lesions
The 211 non-operative CD patients were used to compare the accuracy of bowel US with that of x ray or colonoscopy in determining the anatomical distribution of CD. US examination showed good accuracy in detecting lesions visible at x ray or endoscopy with an overall sensitivity and specificity of 93.4% and 97.3%, respectively. Sensitivity was higher for ileal disease (96.7%) and lower for lesions located in the transverse colon (89%) (table 2). It is worth noting that the majority of the 27 false negative localisations at US consisted of superficial mucosal lesions (that is, few erosions or minute pseudopolyps) at x ray/endoscopy.
Sensitivity and specificity of ultrasound in detecting radiographic and/or endoscopic Crohn's disease (CD) lesions in the 211 non-operative CD patients
Correlations between CD extent measured at US and that determined intraoperatively or at small bowel enema were considered separately in those non-operative and operative CD patients with ileal localisation in whom an accurate measurement of the disease length was feasible at x ray or surgery, respectively. US extent was shown to be well correlated both with x ray involvement (r=0.52) and with surgical measurement (r=0.64) (fig 1). In particular, the extent of bowel involvement measured by US was 22.0 (10.7) cm versus 23.2 (15.7) cm at x ray in non-operative CD patients; similarly, in the operative CD series, US extent was comparable with surgical involvement (23.7 (10.4) cm v 22.2 (12.5) cm, respectively).

Correlation between ultrasound (US) and x ray extent (A), and between disease extent measured at surgery and at US (B) in patients with small bowel Crohn's disease localisation only.
Accuracy of US in detecting strictures
One or more small bowel strictures were diagnosed by x ray in 75 of the 211 non-operative CD patients (35.5%); bowel US correctly detected the presence of strictures in 59 of these patients with only three false positive results (sensitivity 79%, specificity 98%). Of the 85 patients who underwent surgery, one or more strictures were shown in 79 patients (93%): these were located in the small bowel alone (including the ileocaecal valve or anastomosis) in 70 cases (82%) and in the colon in nine patients (three of the latter also had a concomitant ileal stenosis). US detected the presence of small bowel stenoses in 63 of these patients with no false positive results being reported (sensitivity 90%, specificity 100%) (table 3). Positive and negative predictive values of bowel US in the detection of strictures were 95% and 89% in non-operative CD and 100% and 68% in operative CD patients, respectively.
Sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values of ultrasound in detecting one or more small bowel strictures at x ray, evaluated in 211 patients undergoing conservative management (non-operative Crohn's disease (CD)) and in 85 patients undergoing surgery (operative CD)
Regarding the number and location of small bowel stenoses at laparotomy, 59 patients had a single stricture (all but one located in the ileum or at the ileocolonic anastomosis) whereas 11 patients had two or more ileal strictures (five had two stenoses, two patients had three, two had four, and two had six strictures).
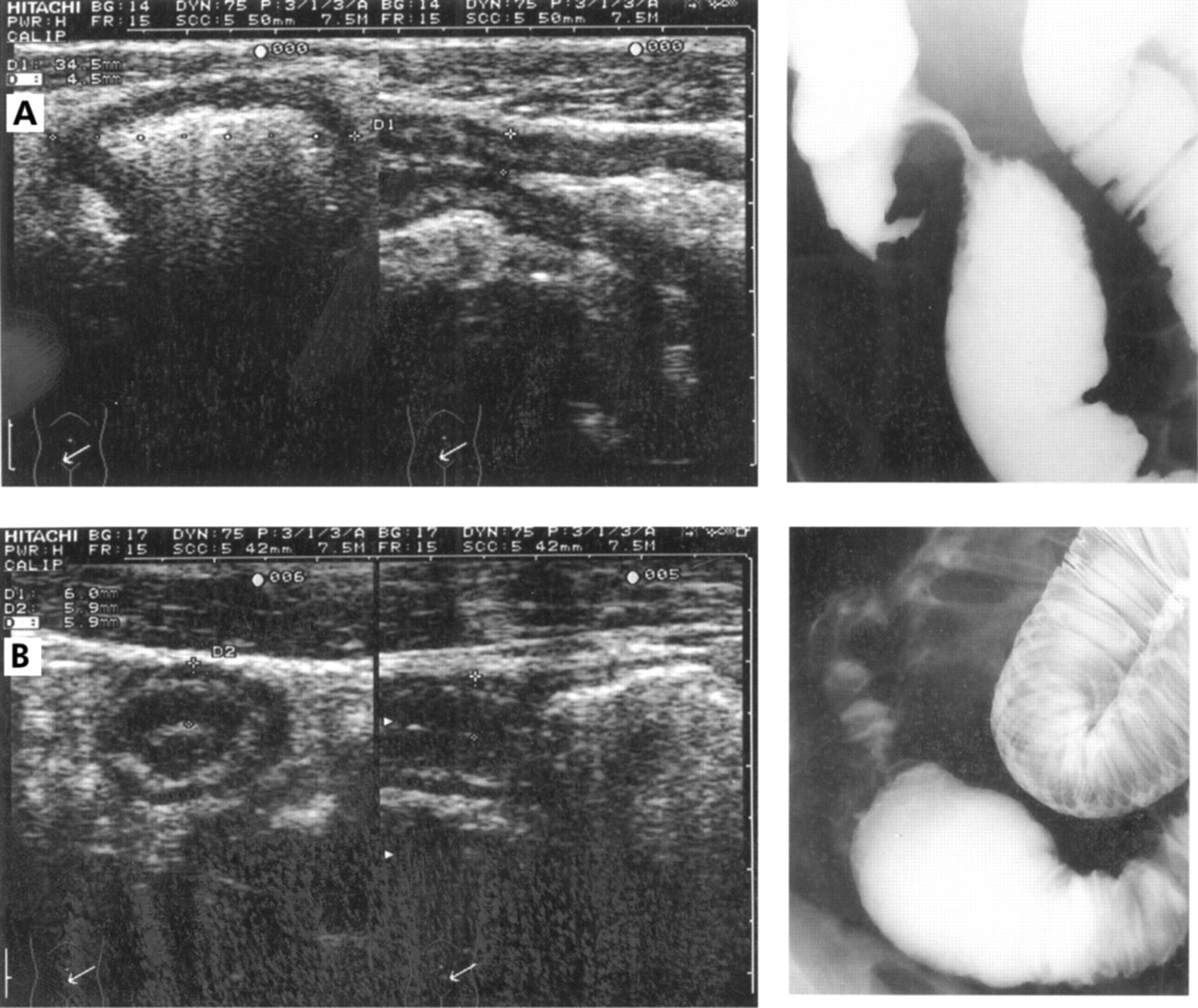
Two examples of ileal stenoses detected at US, with different degrees of prestenotic dilatation, and the corresponding x ray pictures are shown in fig 2A and B.

{kind=link}
{kind=link}
Ultrasound and x ray appearance of two ileal stenoses with different degrees of prestenotic dilatation.
Relationships between disease activity and US findings
Systemic inflammatory markers (namely, C reactive protein serum levels) and CDAI did not significantly differ in the groups of stenotic patients managed medically and surgically. Indeed, C reactive protein levels and CDAI values were 2.9 (2.7) mg/ml and 175.1 (69.5) in non-operative CD and 3.0 (3.6) mg/ml and 179.1 (80.7) in operative CD patients, respectively.
Despite the fact that there was a tendency towards higher BWT values in patients with increased CDAI (mean BWT in CD patients with CDAI >150 was 7.6 (1.8) mm v 7.2 (1.5) mm in those with CDAI ≤150), no significant correlation was found between BWT and CDAI both in the operative CD series (r=0.10, p=0.6) and non-operative CD patients (r=0.02, p=0.9).
DISCUSSION
Barium x ray studies remain the most effective means of evaluating patients with known or suspected CD involving the terminal ileum or more proximal segments of the small bowel. It provides excellent visualisation of the bowel mucosa and can demonstrate any abnormal surface patterns and may reveal intestinal complications such as strictures and fistulae4–6; in addition, it can be used to evaluate the exact number of stenoses as well as their extent, which is useful in patients who are candidates for surgery, to plan the most appropriate procedure (that is, stricturoplasty or resection). On the other hand, barium studies provide limited information on the extent of transmural and peri-intestinal abnormalities, imply radiation exposure, which makes their use contraindicated in children and women of childbearing age, are not feasible in all patients (that is, those with acute obstruction), and are not easily repeatable.
Despite the wider availability of high resolution US over the last decade which has greatly improved the diagnostic accuracy of this procedure in the assessment of bowel diseases,8–11 uncertainty still persists as to its strengths and limitations, as well as its place in relation to other imaging techniques in localising and evaluating the extent of intestinal CD.21 Indeed, to date, few studies have evaluated the accuracy of bowel US in detecting CD lesions seen at x ray or endoscopy. In a small series of patients, Brignola and colleagues22 showed a relatively low sensitivity of US (73%) in revealing x ray lesions with a specificity of 93%. In contrast, in a previous study by our group, we reported good sensitivity and specificity of US for assessing intestinal CD localisation (89% and 94%, respectively 12). Our present results are even better than those observed in the past, with overall sensitivity rising to 93% and specificity of 97%, probably due to the increased experience of the operators. As previously reported by others,18 disease of the terminal ileum was the most easily detected site, with a sensitivity reaching 97%, the left and transverse colon being the most difficult locations to be diagnosed (sensitivity 89% and 90%, respectively).
Concerning the accuracy of US in determining the length of ileal involvement, to date no study had prospectively compared US with small bowel enema and intraoperative findings as in the present investigation. In a very large series of patients, we found that the use of a high resolution probe (7.5 MHz) allowed accurate measurement of pathologically thickened small bowel wall which strictly correlates with CD extent measured both at x ray and surgery. Thus, on the whole, the data suggest that bowel US may constitute a valid alternative to more invasive procedures (that is, small bowel enema) both in the detection of bowel involvement and in assessing progression over time of existing lesions; this makes the examination particularly appealing in the staging of already confirmed disease as well as in the follow up of CD patients. The only limitation of US is in the detection of superficial and rare mucosal intestinal lesions (such as aphthous ulcers or minute pseudopolyps) as they do not cause significant thickening of the bowel wall, which constituted the main reasons for our false negative results.
Concerning the usefulness of US in detecting strictures, until now this had been evaluated prospectively only in one small surgical series of CD patients by Gasche and colleagues.15 These authors, studying a highly selected group of 33 complicated CD patients who underwent surgery, reported 91% sensitivity and 100% specificity for US in the diagnosis of strictures compared with surgicopathological findings. In a retrospective surgical series, Ko et al reported a sensitivity of 89% for US in documenting small bowel strictures not due to CD.23 This study however has been criticised as all patients had intestinal obstruction and underwent surgery and thus US false positive diagnoses could not be made. In addition, the cause of obstruction was varied and was diagnosed in only 20% with US. Ours is the first prospective study in a large series of consecutive CD patients (both complicated and uncomplicated) where bowel US was compared with small bowel enteroclysis and surgical findings in the detection of jejunal and ileal strictures. To avoid bias by selecting only the most severe forms of disease—that is, those more likely to have detectable lesions at US—we divided the study population into two different groups (operative and non-operative CD) and evaluated the performance of US separately in these two groups.
It is worth noting that even in the operative CD cases, we considered barium x ray rather than intraoperative findings as the reference method for bowel strictures. This approach was adopted to more easily compare the techniques in the two different series of patients and also because the indication for elective surgery in these patients usually relies on x ray findings rather than on the clinical condition.24 In the present series, we found US to be helpful in confirming the presence of small bowel obstruction as a correct diagnosis of strictures was shown in 90% of the operative CD cases, a value similar to that reported by Gasche and colleagues15 who also investigated severe and complicated CD patients. One could argue that these impressive results of US in detecting strictures may be due to the seriousness of the stenoses in this highly selected CD population requiring surgery who are therefore more likely to have detectable disease at US compared with those undergoing conservative management. Indeed, small bowel strictures were present in 82% of these patients, a much higher rate than that observed in the general CD population. For this reason, we used the 211 non-operative CD patients studied by US as a “control series”. Indeed, they provided a better indication of the value of US in a less selected population where the established “gold standard” is generally considered small bowel enteroclysis or traditional barium follow through.4 In the latter series of patients, with less severe disease, the sensitivity and specificity of US in the detection of strictures were 79% and 97%, whereas the positive and negative predictive values of US examination were 95% and 89%, respectively. This high diagnostic accuracy concurs well with that previously reported in a smaller series by our group14 and did not markedly differ from those found in patients requiring surgery, thus suggesting that US is a reliable tool in detecting this type of complication.
Concerning the possibility of differentiating fibrotic from inflammatory strictures at US, we found no (as in the present study) or a weak correlation12 between US parameters (namely, BWT) and CDAI or serological parameters of inflammation. This probably reflects the fact that many other factors, other than disease activity, are also responsible for BWT, such as submucosal oedema, cellular infiltration, and fibrosis. Our results concur with those recently reported by Futagami and colleagues25 who found a weak correlation between an ultrasonographic index of Crohn's disease (based on wall thickness and echostratification) and CDAI or biological parameters of inflammation. As the colour Doppler technique (showing hypervascularisation in the thickened bowel wall) could theoretically enable more accurate examination of inflammatory bowel pathology, future large studies should test whether this method could provide important supplementary information in evaluating the local activity of CD in patients with strictures.
In conclusion, findings emerging from the present study show that in expert hands bowel US is an accurate technique for assessing CD extent and anatomical location within the bowel; in addition, it has proved to be very helpful in the detection of small bowel strictures associated with CD, especially in those patients with severe disease who are candidates for surgery; indeed, 90% of stenoses, documented by small bowel enema and subsequently confirmed at operation, are correctly diagnosed by the sole use of high resolution US. In the light of the lack of radiation exposure, ready availability, repeatability, and low cost, we consider that bowel US should be used as the primary investigation, even before performing conventional x ray studies, in those CD patients with suspected complications such as strictures; US may well be used instead of contrast radiology whenever the latter is contraindicated. Finally, it should be borne in mind that this technique is highly operator dependent, requiring great experience and time to achieve accuracy rates comparable with those published in the literature.