Article Text

Abstract
Background: Specialist training in gastroenterology and hepatology is not standardised in different European countries.
Aim: The aim of this survey was to assess the different teaching and socioeconomic aspects of training programmes in Europe.
Methods: Seventy questionnaires were distributed to last year trainees or newly graduated gastroenterologists. Forty two respondents (60%) from 34 major training centres in 10 different European countries replied.
Results: Overall, the data revealed major diversity for all aspects analysed, between and within the different European countries. Both the duration of training (range 4–10.4 years) and workload (range 48.5–89.2 hours per week) differed markedly between countries. The average number of endoscopic procedures (gastroscopies, range 300–2600; colonoscopies, range 73–550; endoscopic retrograde cholangiopancreatographies, range 1–385) differed also. One third of last year trainees reported that they felt uncertain in some endoscopic procedure. The European trainee was on call for 5–6 nights a month on average (range 1–8). Monthly wages differed considerably between countries, ranging from 767 to 2180 Euro.
Conclusion: We found major differences in the professional aspects and socioeconomic conditions of gastroenterologist/hepatologist training in 10 different European countries, probably leading to differences in quality of training. In several countries or centres the average number of procedures was below the threshold issued by the European Board of Gastroenterlogy or the American Gastroenterological Association. Issuing a European diploma for gastroenterology is a valuable effort towards meeting this problem. Further studies are needed to re-evaluate the training programmes in Europe and to define threshold numbers and technical end points for assessment of endoscopic skills.
- training
- endoscopy
- teaching
- EBG, European Board of Gastroenterlogy
- B, Belgium
- D, Denmark
- E, UK
- F, France
- G, Germany
- GR, Greece
- I, Italy
- N, Netherlands
- NO, Norway
- S, Spain
- ERCP, endoscopic retrograde cholangiopancreatography
- AGA, American Gastroenterological Association
Statistics from Altmetric.com
- EBG, European Board of Gastroenterlogy
- B, Belgium
- D, Denmark
- E, UK
- F, France
- G, Germany
- GR, Greece
- I, Italy
- N, Netherlands
- NO, Norway
- S, Spain
- ERCP, endoscopic retrograde cholangiopancreatography
- AGA, American Gastroenterological Association
In the face of increasing changes and challenges in the current health care environment, medical educators in both the USA and Europe have initiated major efforts to anticipate and modify the training needs of the gastroenterologist and hepatologist of the future.1–4 One of the stated aims of the European Board of Gastroenterology (EBG), inaugurated at the first United European Digestive Disease Week in Athens in 1992, is to promote good practice in gastroenterology and hepatology in Europe and to harmonise the different methods of specialist training in different European countries.1 Also, since 1994 the EBG has awarded a European Diploma of Gastroenterology to individual candidates who satisfy a set of criteria for training, including a minimum number of specific gastrointestinal procedures. From the point of view of the European trainee, these aims by the EBG, namely to guarantee quality of training and to harmonise specialist training, are laudable and to be commended. However, while information on current training patterns is not a prerequisite for defining appropriate training aims, such information could be both useful and interesting. We therefore designed a survey that aimed to assess the clinical and technical particulars and also the workload and socioeconomic aspects of the training of physicians specialising in gastroenterology/hepatology in 10 different European countries.
METHODS
The questionnaire
We designed a 60 point questionnaire with mostly definite and a few open ended questions. The questionnaire was divided into four sections. The first section addressed general issues such as age, sex, marital status, number of departmental beds, and number of staff members and gastroenterology/hepatology trainees at a particular training hospital. The second section dealt with training as such, and was divided into seven subsections concerning: work on the ward, work in the outpatient clinic, endoscopic training, technical training in other specialised procedures, administrative workload, research and teaching, and night shifts. The third section aimed at the social and financial aspects of training. The fourth and last section posed questions on both the outlook of the trainee towards future job prospects and the number of graduates per year in a particular training centre. The participants were asked to answer the questionnaire representatively for their situation in a particular training centre. The respondent was free to provide his name and/or the name of the training centre.
Distribution of the questionnaires and data collection
The questionnaire was distributed to a total of 70 last year trainees or to specialists that had just completed their training in gastroenterology/hepatology, working in 10 different European countries. Excluding Belgium, the questionnaire was mailed to 13 physicians in nine different European countries (Denmark (D)=1, UK (E)=2, France (F)=2, Germany (G)=2, Greece (GR)=1, Italy (I)=1, Netherlands (N)=1, Norway (NO)=1, Spain (S)=2) who were asked to distribute a copy to four other last year trainees working at different large training hospitals within their own country. In Belgium, four other colleagues working in four different university hospitals were contacted directly.
In total, 42 respondents (60%) working in 34 different major training centres throughout Europe (B=5, D=5, E=8, F=5, G=5, GR=1, I=5, N=2, NO=1, S=5) returned the questionnaire. In each centre two gastroenterologists graduate per year on average.
Data analysis
Each returned questionnaire was labelled to indicate the country of origin and the training hospital (for example, D3 is a reply from the third training hospital in Denmark). Data are presented as raw data for each training hospital or as the average per country. Salaries in different currencies were converted to Euros. Due to the small number of respondents in the Netherlands, Norway, and Greece, these countries were not taken into account when the different countries were compared. However, their answers were used for calculating overall averages. The average of all 42 respondents is referred to as “Europe”.
RESULTS
Age and years of training
Mean age of the last year trainee was 33 years (range 28–41); mean age per country ranged from 29 to 39 years. The official duration of common trunk training and speciality training, as issued by national governments, is displayed in table 1. In most countries the duration of common trunk training did not exceed the duration of speciality training, except in Germany (five and three years, respectively). In France and Italy, common trunk training is not compulsory. The mean number of years of training reported by the respondents was 6.4, with a large variation between different countries (range 4–10.4). In the UK and Denmark in particular, the duration of training reported by the respondents differed from the official length of training.
Endoscopy training
Relationship between number of beds, number of trainees, and number of staff members in the training hospitals
The average number of beds per staff member in a European training centre was 5.18 (range 1.96 in Italy to 11.31 in Germany) (table 2). The mean number of staff members in the gastroenterology/hepatology department in a European training centre was 9.3 (range 2–25) (table 2). In most European countries a trainee had one or two staff members at his disposal at one specific moment during his specialisation (mean ratio assistants/staff members=0.75, range 0.25–1.55). During his entire training, the candidate was tutored by a larger number of staff members as a result of a system of rotations.
Relation between number of beds (beds), number of trainees (ass), and number of staff members (staff)
Training on the ward and in the outpatient clinic
On average, a last year trainee in Europe was in charge of 14.7 (range 0–30) hospitalised patients per week and saw 21 patients per week in the outpatient clinic (range 0–40) (table 3). No data are available on the proportions of new patients or follow up patients.
Training on the ward and in the outpatient clinic
On average, the European last year trainee spent 31.2 hours working on the ward and 9.8 hours examining patients in the outpatient clinic per week. Only in Germany was the trainee working either on the ward or in the outpatient clinic. In all other countries the trainee was employed on both the ward and outpatient clinic, and when he/she spent more hours on the ward, he/she spent less time in the outpatient clinic and vice versa.
Training aspects: endoscopy training
The total number of gastroscopies varied significantly between the different European countries (table 1). On average, a European trainee performed 1363 (range 20–4000) gastroscopies before graduating but a newly trained gastroenterologist in Italy, Spain, and Germany had clearly performed fewer gastroscopies. The average number of colonoscopies performed by a European trainee was 348 with considerable variations between countries (range 0–2500) (table 1). On average, a European trainee had performed 113 endoscopic retrograde cholangiopancreatographies (ERCPs) during endoscopy training but the screened centres in some countries did not provide training for this specialised procedure (range 0–1000) (table 1).
The number of therapeutic procedures was calculated using the total number of procedures and the estimated percentage of all endoscopic procedures that were therapeutic. On average, a European trainee performed 156 (11%) therapeutic gastroscopies, 61 (17 %) therapeutic colonoscopies, and 41 (36%) therapeutic ERCPs (table 1).
Training aspects: other specialised procedures
In this section of the questionnaire, we tried to assess the amount of training in other than the classical endoscopic procedures—that is, abdominal ultrasound, endoscopic ultrasound, radiology training, proctology, rectal manometry, oesophageal manometry, 24 hour pH metry, gastric and small intestinal manometry, interpretation of breath tests, interpretation of stool microscopy, and interpretation of biopsies. As several of these procedures were only applicable to a few training centres in a few countries, table 4 summarises only those specialised procedures that assistants regularly reported that they had received training. Training in stool sampling was only given on a regular basis in three training centres. Endoscopic ultrasound, gastric/small intestinal manometry, and rectal manometry were part of the basic training programme in, respectively, four, four, and seven of the 34 training centres.
Other specialised procedures included in the basic training programme
Regular training in abdominal ultrasound was provided in only four countries, and the average number of abdominal ultrasound scans performed by the end of the training varied considerably between countries (table 4) and between training centres in one country (for example, Spain 10–300, France 50–1500). Training in interpretation of radiology documents was given in approximately 50% of the European training centres. Less than 50% of all trainees in the different European countries received training in proctology. One third of assistants were trained in oesophageal manometry and 40% in 24 hour pH metry (table 4). Regular training in interpreting breath tests and biopsies was provided in 20–60% of training centres in European countries.
Training aspects: supervision of the trainee
Staff members directly supervised 21.3% (range 0–100%) of patients seen in the outpatient setting. The European average of supervised hours on the ward was 27% (range 0–100%) (table 3). Both the wide variability of these European averages and the broad range of averages for each country does not permit a comparison between the different countries. The same applies to supervision at the beginning of endoscopy training (table 5). On average, a European trainee was directly supervised during endoscopic procedures for 12 months. The dissimilarity between the various European countries was remarkable: in Italy, the trainee was supervised for 27 months on average, which constitutes 75% of total endoscopy training. In contrast, in Denmark, this period was limited to one month or 2% of endoscopy training. The disparity within particular countries was also striking. For example, in France, five respondents mention periods of direct supervision ranging from 0 to 24 months. Twenty one respondents mentioned the number of procedures they had to perform before they were granted autonomy in conducting the endoscopies. On average, 58 gastroscopies (range 27–97) and 63 colonoscopies (range 9–118) were directly and constantly supervised at the start of endoscopy training in Europe.
Direct supervision during endoscopy training
To investigate the grade of independence of the trainee, we enquired about the percentage of procedures that were directly supervised during the last year of training. The European average was 35% (range 8–85) (table 5). Clearly, at the end of training there was still a significant difference in autonomously performed procedures between the different countries and between the different training centres in one country.
Teaching aspects: research and teaching
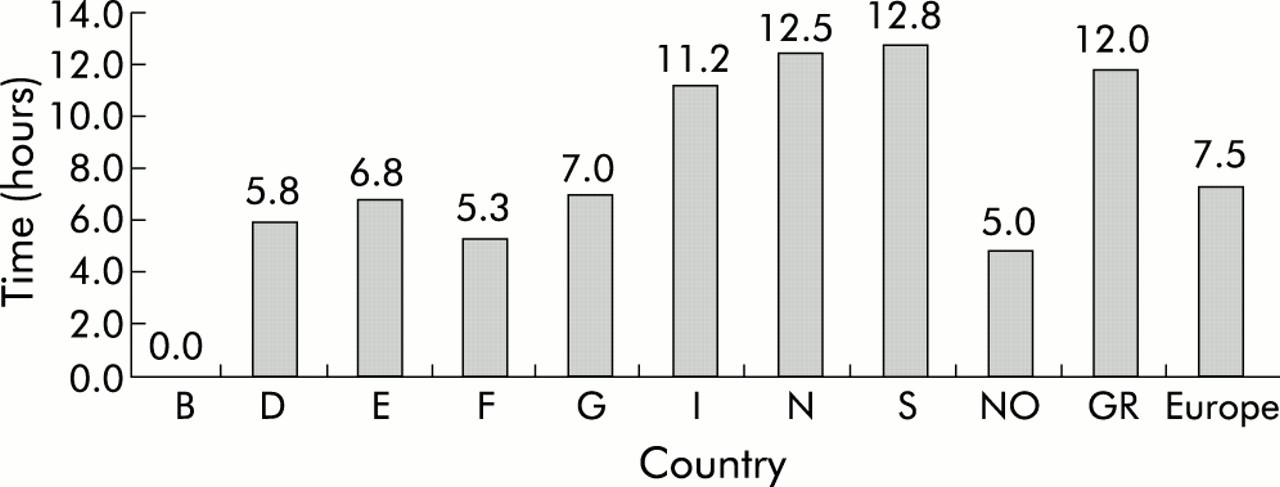
On average, a gastroenterology/hepatology trainee in Europe spent 7.5 hours per week on research (fig 1). In Belgium, five respondents from five different training centres reported no available time for research. The mean number of teaching rounds per week attended by a European trainee was three. The average numbers were comparable in most countries. The mean number of teaching rounds given by a trainee varied considerably (mean 8, range 3.4–20.3) (fig 2).

Average number of hours spent on research per week in the different European countries. B, Belgium; D, Denmark; E, UK; F, France; G, Germany; I, Italy; N, Netherlands; S, Spain; NO, Norway; GR, Greece.

Average number of teaching rounds attended per week and given per year in the different European countries. B, Belgium; D, Denmark; E, UK; F, France; G, Germany; I, Italy; N, Netherlands; S, Spain; NO, Norway; GR, Greece.
Teaching aspects: fields that were perceived to be undertrained
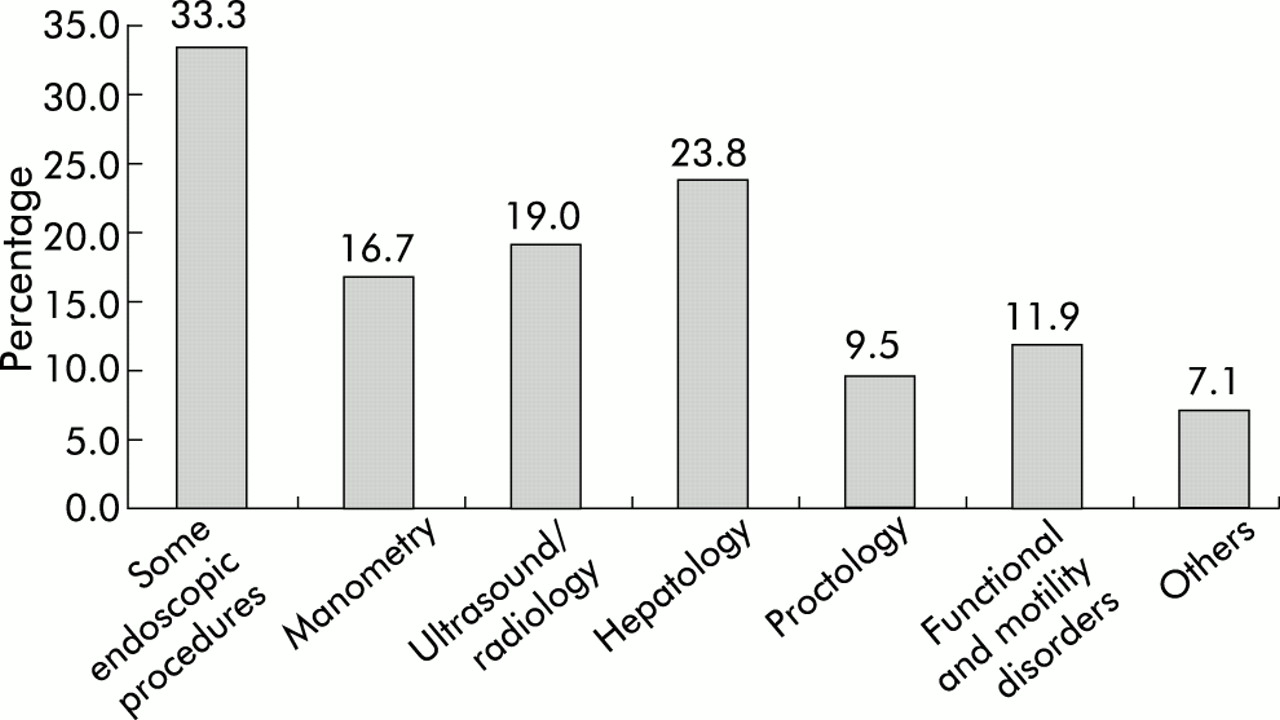
This part of the questionnaire, asking respondents in which field of gastroenterology/hepatology they subjectively felt undertrained, was answered by 34 of the 42 respondents (fig 3). Remarkably, one third of last year trainees feel undertrained in some diagnostic endoscopic procedure, including ERCP, colonoscopy, or a therapeutic procedure such as sclerotherapy. One quarter of graduates felt uncertain in the field of hepatology. Almost 10% judged their training in proctology as insufficient to achieve proficiency. Finally, in the field of specialised procedures, 16.7% felt undertrained in manometry and 19% in radiology, including abdominal ultrasound.

{kind=link}
{kind=link}
{kind=link}
Fields in which last year trainees felt undertrained.
Socioeconomic aspects of training: workload, wages, night shifts, family status, and job prospects
On average, a European trainee in gastroenterology worked for 70 hours a week, which constituted 59 hours of hospital work (85%), including night shifts, and 11 hours of administrative work (15%), including dictating letters, writing up orders, documenting hospital stay, etc. (table 6). Distinct differences between the total workload in the different European countries were apparent, with a remarkably higher total workload in Belgium: 89.2 hours per week on average. A single Greek respondent reported 95 working hours per week. The administrative workload ranged from 5% to 23% of the time (table 6).
Socioeconomic aspects of gastroenterology training in Europe: workload, wages, and family status
On average, the European trainee was on call for 5–6 nights a month, of which he had to spend 2–3 nights in the hospital and three nights at home (table 6). The ratio between inhouse and home on-calls varied between the different countries but the total number of night shifts was comparable for most countries.
The salary of a European last year gastroenterology trainee was an average of 1669 Euro per month, with striking differences between countries (range 767–2234 Euro). The ratio between the average salary and average total workload was rather low (on average 5.97 Euro per hour) and was most profitable in Denmark where the trainee earned 10.9 Euro per hour (table 6). Solid prospects for a job after the last year of training varied from one third of graduates in the UK to 100% for Denmark and the Netherlands.
DISCUSSION
To our knowledge, this is the first attempt at assessment of the technical and clinical particulars and socioeconomic conditions of trainees in gastroenterology/hepatology in different European countries. The answers provided by 42 trainees in 10 different countries, working in 34 major training centres, clearly showed that there are important differences in almost all aspects of training within and between countries.
The average number of gastroscopies and colonoscopies performed by a last year trainee at the end of endoscopy training varied markedly between the different countries. Following the efforts of the American Gastroenterological Association (AGA),2,11 the EBG established primary goals for assessment of the technical skills of the applicant for the diploma in 1994, to promote good practice in gastroenterology.1 The minimum number of gastroscopies necessary for achievement of the diploma was set at 300 diagnostic and 30 therapeutic procedures.1 The threshold number for colonoscopies to qualify for the European diploma was 100 total colonoscopies and 50 therapeutic procedures, such as polypectomy and haemostatic techniques.1 Competence in endoscopy implies the attainment of both the technical skills with the endoscope and the cognitive ability to evaluate the findings and to develop an effective treatment plan.5,6 Assessment of this competence is not easy and although a minimal threshold of procedures is one way to meet this problem, this approach does not take into account the cognitive ability of the trainee. The AGA set the threshold number of procedures for endoscopic skills at 100 gastroscopies and 35, later 40, therapeutic procedures.4,6 Only a few studies have attempted to provide an objective evaluation of the technical skills of young gastroenterology trainees according to the number of endoscopies they performed.5,7,8 Cass and colleagues demonstrated a two phase learning curve in oesophagogastroduodenoscopy both for oesophageal intubation and for reaching the pylorus. The intubation rate reached 90% after 50 endoscopies but this rate dropped to 75% after approximately 100 procedures with the introduction of more complicated cases. Cass and colleagues concluded that more than 100 supervised procedures were necessary to achieve technical competence9 and not just 100 procedures. Marshall evaluated the technical skills of colonoscopies by combining the achievement of a certain end point (reaching the caecum) with a time limit (30 minutes).5 He concluded that the threshold of 100 colonoscopies, as proposed by the AGA and EBG, may be low as in his study the first year trainee had an overall success rate of 54% of cases in contrast with a second year assistant where this was 86%. The latter had performed 328 colonoscopies on average whereas the former had carried out 149 colonoscopies. Cass and colleagues9 also found that over 100 colonoscopies were required before the trainee was able to reach the caecum in 90% of endoscopies. Church10 found that the rate of reaching the caecum did not rise above 62% for procedures 76–100. The Conjoint Committee for Recognition of Training in Gastrointestinal Endoscopy of Australia emphasised both the achievement of a threshold (200 gastroscopies, 100 colonoscopies, and 200 ERCPs) and registration of the success rate in a log book.12,13 We did not explicitly ask if trainees had to register the number of procedures and their success rate in a log book. Regarding supervision at the beginning of endoscopy training, the EBG does not provide specific guidelines or threshold numbers before autonomy in performing endoscopies can be granted: “The practical skills . . . should be acquired under appropriate supervision within the training period”.1 A similar reasoning is followed by the AGA: “When performing endoscopic procedures early in training, each trainee should be observed regularly by a supervisor. . . . Simpler procedures may require fewer observations, whereas those that are technically complex may require more”.4 Decisions on decreasing the level of direct supervision are left to the supervisor. In Australia, the supervisor has to declare that the trainee is competent, both in technical and cognitive skills, on completion of the training, before privileges are granted to perform endoscopic procedures independently.12
Considering these studies and guidelines, endoscopy training seemed to be inadequate in the centres we surveyed in at least four countries. As our survey demonstrated, supervision varied markedly between centres in different European countries and between different training centres in a single country. Subjectively, endoscopy training did not always seem to be satisfactory as one third of trainees reported to be lacking in confidence for some endoscopic procedures.
The basic training programme also varied considerably between the different countries. Some procedures that were compulsory for the basic diploma of the EBG were not included in the programmes of some training centres, whereas some optional subjects seemed to be scheduled on a regular basis in other centres. Abdominal ultrasound, obligatory in the EBG curriculum, seemed to be a regular part of gastroenterology training only in France, Germany, Italy, and Spain, the latter not reaching the reference threshold of 300 ultrasounds.1 Optional training in ERCP is a basic endoscopic procedure in most European countries except for France, Italy, and Spain. Although the technique is being taught, the EBG threshold of 150 ERCPs was reached only in the UK. The European average itself was only 113. As trainees remain 20% behind the ability of their supervisors after 100 ERCPs and therefore more than 100 ERCPs are needed to approach their skills,14 ERCP training was inadequate throughout Europe during the basic gastroenterology training, except in the UK. Manometric investigations and pH metry were also optional subjects in the EBG curriculum. They were sporadically provided as a basic training technique in several training centres throughout Europe, especially in Germany. In contrast with ERCP training, oesophageal manometry and pH metry training were in line with the EBG reference standard of 50 procedures.
Both the AGA and EBG described the requirements of facilities and resources essential for accrediting a training centre, without giving definite specifications on numbers of beds, staff members, or patient turnover.1,4,15 In Europe, a training centre can only be approved after a visit by two gastroenterologists appointed by the EBG. In practice, the make up of the training centres in the different European countries varied markedly. Whether the different structures in the training hospitals have any effect on the quality of training is hard to assess. Apparently, most trainees seemed to gather enough and comparable clinical experience both in the outpatient clinic and on the ward.
In the field of research the EBG requires at least two publications in recognised journals and two oral presentations.1 The AGA emphasises that “a major contributor . . . is active participation in one or more research projects, ideally followed by presentation . . . at a national meeting and publication of a paper . . .”.4 We did not specifically enquire about the number of presentations or publications but we found that in most European countries trainees were able to spend 7.5 hours a week on research activities. In the Italian and Spanish centres, this was extended to more than 11 hours per week. In contrast, in Belgium, the gastroenterology trainee was not allowed any extra time for research purposes.
Regarding socioeconomic aspects, the data obtained reflected the disposition of our society towards the making of a specialist: on average, a 70 hour week with an hourly salary that is generally paid to employees of lower expertise and responsibility.
In conclusion, gastroenterology training differed markedly in European training centres. Although the EBG does “not seek complete uniformity of training”,1 the current dissimilarities between the 34 training centres in 10 different countries in this survey can hardly be regarded as demonstration of harmonised European training. Even though this survey was not all encompassing due to a limited sample size and the fact that it was organised by only one training centre, it reflects the training of several specialists in gastroenterology/hepatology working in Europe. Therefore, it would be useful to re-evaluate our findings in a larger multicentre study, ideally coordinated by the EBG. This survey could then be combined with further studies to define threshold numbers and technical end points to assess competence in endoscopic procedures and cognitive skills.
The disparity in the training of young gastroenterologists results in differences in quality between graduates which may hamper clinical competence of certain specialists at the beginning of their career. In this respect issuing a European diploma for gastroenterology is a valuable effort towards promoting good practice in European gastroenterology but without any enforcement or greater public awareness its chance of influencing structural changes in individual countries may be slim.
Acknowledgments
We would like to acknowledge Dr N Thorsgaard, secretary of the European Board of Gastroenterology, for providing data on the official duration of speciality and common trunk training in Europe.
Supplementary materials
Web-only long version of:
A survey on gastroenterology training in Europe