Article Text

Abstract
Background: Refractory coeliac sprue (RCS) with an immunophenotypically aberrant clonal intraepithelial lymphocyte (IEL) population is considered a cryptic form of intestinal T cell lymphoma.
Aims: To investigate the distribution of the abnormal and monoclonal IEL population in the digestive tract of RCS patients.
Patients and methods: We compared the frequency of lymphocytic gastritis (LG) and lymphocytic colitis (LC), together with IEL phenotype and T cell clonality, in gastric and colonic samples from 15 adults with RCS (all with aberrant CD3 intracytoplasmic+ surface− CD8− clonal IELs on duodenojejunal biopsies), 18 patients with active coeliac disease (ACD), and 10 patients with coeliac disease (CD) on a gluten free diet (GFD-CD) by means of immunohistochemistry and multiplex polymerase chain reaction amplification of the T cell receptor γ gene (TCR-γ) rearrangement. Blood samples of nine RCS patients were also tested for clonality.
Results: LG was found in 9/14 (64%), 11/18 (61%), and 3/10 (30%) patients with RCS, ACD, and GFD-CD, respectively, while LC was found in 6/11 (55%), 3/4 (75%), and 2/3 (66%) patients. Contrary to CD, all samples from patients with LG and LC showed an aberrant IEL phenotype. Monoclonal TCR-γ rearrangements were detected in 8/13 (62%), 8/10 (80%), and 4/9 (44%) of gastric, colonic, and blood samples, respectively, from RCS patients, while in CD patients such rearrangements were only found in 2/25 (8%) gastric samples.
Conclusion: The immunophenotypically aberrant monoclonal IEL population present in the small intestine of patients with RCS frequently disseminates to the blood and the entire gastrointestinal epithelium, suggesting that this is a diffuse gastrointestinal disease.
- enteropathy-type intestinal T cell lymphoma
- lymphocytic gastritis
- lymphocytic colitis
- coeliac disease
- refractory sprue
- T cell receptor gene rearrangement
- ACD, active coeliac disease
- CD, coeliac disease
- GFD, gluten free diet
- GFD-CD, CD on a GFD
- EITCL, enteropathy-type intestinal T cell lymphoma
- IEL, intraepithelial lymphocyte
- LC, lymphocytic colitis
- LG, lymphocytic gastritis
- PCR, polymerase chain reaction
- RCS, refractory coeliac sprue
- TCR, T cell receptor
Statistics from Altmetric.com
- enteropathy-type intestinal T cell lymphoma
- lymphocytic gastritis
- lymphocytic colitis
- coeliac disease
- refractory sprue
- T cell receptor gene rearrangement
- ACD, active coeliac disease
- CD, coeliac disease
- GFD, gluten free diet
- GFD-CD, CD on a GFD
- EITCL, enteropathy-type intestinal T cell lymphoma
- IEL, intraepithelial lymphocyte
- LC, lymphocytic colitis
- LG, lymphocytic gastritis
- PCR, polymerase chain reaction
- RCS, refractory coeliac sprue
- TCR, T cell receptor
Coeliac disease (CD) is an autoimmune gluten sensitive enteropathy with malabsorption due to characteristic histological lesions of the small intestine, including villous atrophy, crypt hyperplasia, and elevated numbers of intraepithelial lymphocytes (IELs).1 This increase in the number of IELs can also be observed in the stomach (lymphocytic gastritis (LG)) and colon (lymphocytic colitis (LC)) of patients with CD,2–5 suggesting that intraepithelial T cell infiltration occurs at all levels of the gastrointestinal tract in CD.
Refractory coeliac sprue (RCS) is the most frequent cause of refractory sprue syndrome, a heterogeneous entity6 (C Cellier, personal communication) defined clinically by severe symptomatic villous atrophy of the small intestine mimicking CD but with no initial or secondary improvement after a strict gluten free diet.7,8 RCS shares genetic, biological, and histological features with CD.9,10 IELs are also morphologically normal and abnormally abundant in RCS but, in contrast with CD, they harbour clonal T cell receptor γ (TCR-γ) rearrangements and have an aberrant immunophenotype, possessing surface CD103 and intracytoplasmic CD3 (iCD3ε) but lacking surface CD3-TCR complexes (sCD3ε−, CD8−, TCR−).9,10
This clonal population is easily detected by analysing DNA extracted from intestinal biopsy specimens, and the aberrant phenotype can be detected with a simple immunohistochemical method on formalin fixed paraffin embedded biopsy samples.9–11 Detection of such an aberrant clonal IEL population in patients with manifestations of RCS is associated with poor outcome and a higher risk of overt T cell lymphoma than in CD.10 This has led to RCS being considered a cryptic form of enteropathy-type intestinal T cell lymphoma (EITCL).6,10,12–14
The ability of this abnormal monoclonal IEL population to disseminate in RCS has been suggested by detection of a monoclonal T cell population in the blood and colon of four RCS patients.9,10 A circulating monoclonal T cell population was associated in one patient with a high percentage of circulating CD103+ CD3− lymphocytes. Dissemination of the abnormal monoclonal IEL population to the gastrointestinal tract has not been extensively investigated. One recent study showed involvement of the gastric mucosa in two of six patients with LG but phenotyping and molecular studies were not done.15 Reports concerning the colonic mucosa of RCS patients4,9,15–17 have shown an incidence of LC of between 0% (0/8 patients) and 75% (3/4 patients).16 Only three reports described an abnormal percentage of CD8− IELs in the nine cases of LC analysed,4,9,17 and only one described a monoclonal T cell population.17
To determine whether RCS is indeed a diffuse gastrointestinal disease, we investigated the ability of the immunophenotypically aberrant monoclonal IEL population to disseminate to the gastric and colonic mucosa in a large series of patients. Patients with active coeliac disease (ACD) and those with CD on a gluten free diet (GFD-CD) were studied as controls.
PATIENTS AND METHODS
Samples
Centralised biopsy samples were obtained from the pathology department of Necker-Enfants Malades Hospital; they had been collected from patients with RCS and CD at Georges Pompidou Hospital and by the French Coeliac Disease Study Group. All patients investigated here had been enrolled in a prospective study of lymphoma onset and gave informed consent, in keeping with the Helsinki declaration. The study was approved by the ethics committee of Necker-Enfants Malades Hospital in 1997.
Patients with RCS
Fifteen adults (12 women and three men), mean age 51 years (21–73), followed between 1992 and 2001 were studied. Ten of the 15 patients have been described in detail elsewhere.9,10 Patients were only included in this study if stored frozen samples of gastric and/or colonic mucosa were available. Mean time between CD diagnosis and RCS diagnosis was 4.9 years (1.3–13.6). Eleven patients had initial clinical and histological improvement after gluten withdrawal after a mean of 6.2 years (range 2–13.6).
All five new patients fulfilled Trier’s criteria for refractory sprue7,18 and failed to improve clinically and histologically, either initially (n=3) or subsequently (n=2), despite following a strict GFD for at least six months. At diagnosis (before starting a GFD), circulating antigliadin and/or antiendomysium IgA and/or IgG antibodies were detected in three of five patients tested. All five patients expressed the HLA-DQ2 allele, as shown by amplification of the DQB1 gene (InnoLipa, Abott, France). One patient had hyperlymphocytosis, 83% of circulating lymphocytes bearing the same phenotype as small intestine IELs (CD103+, sCD3ε−, iCD3ε+, CD2+, CD8−, CD4−, CD56−). Treatment consisted of steroids, total parenteral nutrition (n=3), anti-tumour necrosis factor (n=1) or hydroxy urea (n=1). One patient developed EITCL, and five patients died of severe malabsorption.
All 15 patients had duodenal biopsy, 10 had jejunal biopsy during push enteroscopy, 13 had gastric biopsy, and 10 had colonic biopsy. Blood samples were collected from nine patients. Histological analysis of duodenal and jejunal biopsy specimens showed patchy villous atrophy ranging from type 3a to type 3c of Marsh’s modified classification (Marsh grade II to IV).19 The IEL phenotype was abnormal in all duodenojejunal samples, with a mean proportion of CD3+CD8− cells ranging from 91% (60–100%) to 94% (55–100%) in duodenal and jejunal biopsies, respectively. No overt T cell lymphomas were observed. All 15 duodenal and 10 jejunal biopsies had a monoclonal TCR-γ gene rearrangement.
Patients with coeliac sprue
Twenty eight patients with CD studied from 1996 to 1999 were separated into two groups according to their diet (normal or gluten free) and intestinal histological lesions.
Patients with active coeliac disease (ACD)
Eighteen patients (12 women and six men) were studied, three just after diagnosis and 15 after a mean of 8.4 years (1–30) on a normal or near normal gluten containing diet. Mean age at biopsy was 34 years (19–74) and mean age at diagnosis was 16 years (range 1–74). All 11 patients tested had the HLA-DQ2 phenotype. Of the 13 patients tested at the time of biopsy, two were positive for antiendomysium antibodies, three were positive for antigliadin antibodies, and eight were positive for both antibodies. All 18 patients had gastric and duodenal biopsies, and 11 had push enteroscopy with jejunal biopsies. Four patients had colonic and rectal biopsies to explore diarrhoea or profound anaemia. Histological and immunohistochemical studies of duodenal and jejunal biopsy specimens always showed partial to subtotal villous atrophy (types 3a to 3c)19 and normal proportions of CD3+ CD8− IELs (2–44%, mean 11% in the duodenum; 5–43%, mean 26% in the jejunum). A polyclonal TCR-γ gene rearrangement was found in all 18 duodenal specimens and in all 11 jejunal specimens studied.
Patients with coeliac disease on a gluten free diet (GFD-CD)
Ten patients (seven women and three men) who had been on a strict GFD for a mean of 5.6 years (0.75–20) were studied. Mean age at biopsy was 37 years (range 17–73) and mean age at diagnosis was 30 years (range 1–54). All nine patients tested had the HLA-DQ2 phenotype. All five patients tested for antiendomysium antibodies at the time of biopsy were negative. All 10 patients had gastric and duodenal biopsies, and four had push enteroscopy with jejunal biopsies. Three patients had colonic or rectal biopsies for persistent diarrhoea. Histological analysis of duodenal and jejunal biopsy specimens showed normal villi (type 1 to type 2) in five cases19 and normal villi to partial villous atrophy (type 1 to type 3a) in five cases. The IEL phenotype was normal in all duodenal and jejunal specimens, with a proportion of CD3+ CD8− IELs between 8% and 40% (mean 25%) and 8% and 32% (mean 21%), respectively. All 10 duodenal and four jejunal samples showed polyclonal TCR-γ gene rearrangement.
Histology and immunohistochemistry
Formalin fixed paraffin embedded samples were used for standard histological and immunohistological analysis.
IELs were counted by standard histological and immunohistochemical analysis. LG was defined by the presence of 25 or more IELs per 100 gastric columnar epithelial cells (surface and foveolar)2 and LC was defined by increased (>20%) lymphocytic infiltration of the superficial colonic epithelium.20
Immunohistochemical analysis was performed on Superfrost slides using 5 μm sections of 10% formalin fixed paraffin embedded samples, with a three stage indirect immunoperoxidase technique described elsewhere.11 We used a rabbit polyclonal antibody directed against human CD3 (A0452) and a mouse monoclonal antibody directed against human CD8 (C8/144B, M703), both from Dako A/S (Glostrup, Denmark). Samples were pretreated with microwaves (3×5 minutes) for antigen retrieval in a 10 nmol/l citrate buffer, pH 6.0.
The percentage of labelled IELs was established on well oriented serial sections by two independent observers (VV and NPMDS) who counted 200–500 epithelial cells per section/patient. When IEL numbers were significantly increased, the percentage of CD3 positive CD8 negative cells was deduced from the percentage of CD3+ IELs and that of CD8+ IELs, as follows:
The proportion of CD3+CD8− IELs was considered abnormal when higher than 52%.10
Molecular studies
Samples of gastric, duodenal, jejunal, and colonic mucosa used for molecular analysis were snap frozen in liquid nitrogen and stored at −80°C. DNA was extracted with phenol-chloroform from entire cryopreserved biopsy specimens pulverised with a frozen mortar, and from peripheral lymphocytes (0.5–1×106), as previously described.9,10
TCR rearrangements were identified by amplifying TCR-γ V-J junctional regions in multiplex polymerase chain reactions (PCRs) using two distinct mixes and high resolution fluorescence analysis, as described in detail elsewhere.9,10,21 PCR products were sized by means of high resolution analysis on an ABI PRISM 310 genetic analyser (Perkin-Elmer Applied Biosystems, Warrington, UK). In parallel, PCR products were run on 10% polyacrylamide gels, stained with ethidium bromide, and viewed under ultraviolet light. Clonality was defined by the presence of one or two dominant bands.
Statistical analysis
For each biopsy site, results were compared between the RCS group and each CD control group (ACD and GFD-CD). The prevalence of LG and LC was compared using Fisher’s exact test. Mean numbers of CD3+ IELs, calculated percentage of CD3+CD8− IELs, and the percentage of samples bearing monoclonal TCR-γ gene rearrangements were compared using Wilcoxon scores (a non-parametric test). Differences were considered significant when p<0.05.
In RCS, the relation between detection of monoclonal TCR-γ rearrangement and the presence or absence of LG or LC was studied on gastric and colonic samples only. The positive predictive value of TCR-γ analysis was defined as the probability of having LG or LC when the TCR-γ gene rearrangement was monoclonal; the negative predictive value was defined as the probability of having normal gastric or colonic samples (with no IEL expansion) when the TCR-γ gene rearrangement was polyclonal.
RESULTS
Histological findings
Histological aspects of gastric and colonic samples in RCS and in the two groups of CD are shown in table 1. The mucosal architecture of the gastric and colonic biopsy samples was normal in the three groups. LG was present in 64% (9/14), 61% (11/18), and 30% (3/10) of patients in the RCS, ACD, and GFD-CD groups, respectively; LC was present in 55% (6/11), 75% (3/4), and 66% (2/3) of patients, respectively. No signs of overt T cell lymphoma or collagenous colitis were observed.
Histological aspects of gastric and colonic samples in patients with refractory coeliac sprue (RCS) and two groups of patients with coeliac disease (CD)
Immunohistochemical findings
The percentages of CD3+, CD8+, and CD3+CD8− IELs in duodenal, gastric, and colonic samples are shown in fig 1. Immunostaining patterns are illustrated in fig 2.
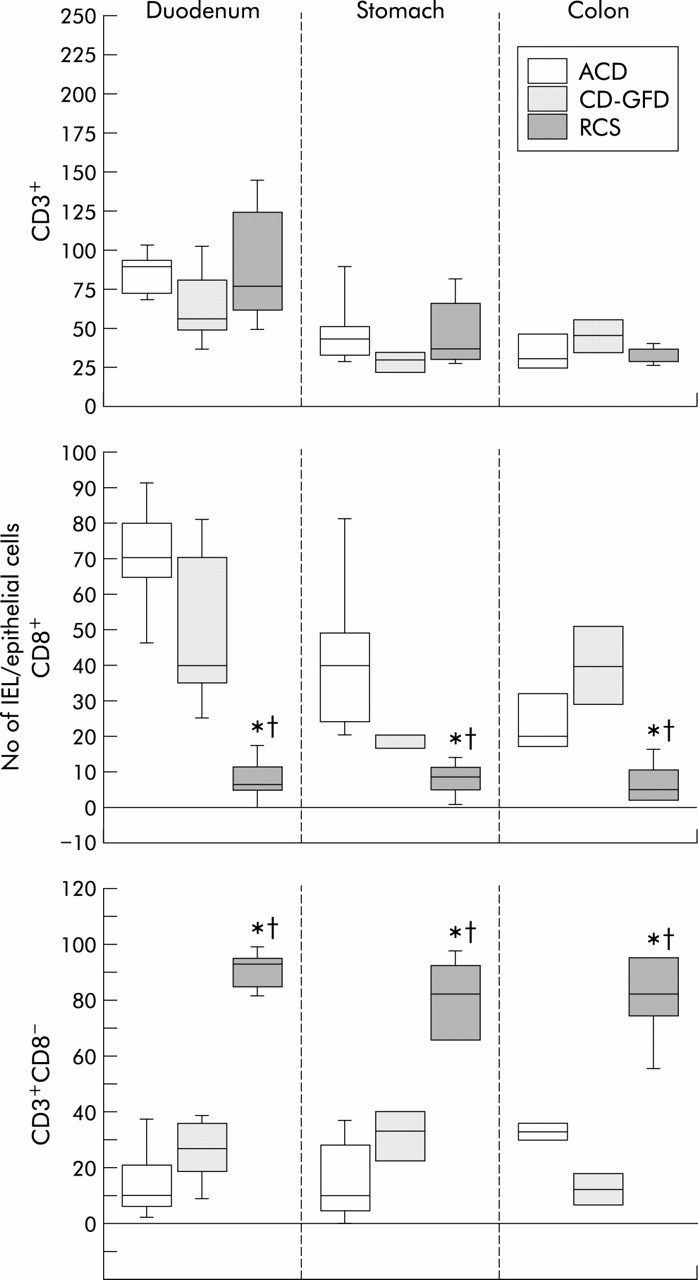
Intraepithelial lymphocyte (IEL) numbers (medians (interquartiles)) labelled with anti-CD3 (top) and anti-CD8 (middle), and calculated numbers of IELs expressing CD3 but not CD8 (CD3+CD8−) (bottom) in patients with acute coeliac disease (ACD), coeliac disease on a gluten free diet (GFD-CD), and refractory coeliac sprue (RCS), in duodenal, gastric, and colonic samples. Statistical analysis was based on non-parametric Wilcoxon scores. Note that the scale of the y axis is different in the three figures and depends on the mean number of IELs labelled by each antibody. RCS patients had significantly lower numbers of CD8+ IELs and significant higher numbers of calculated CD3+CD8− IELs. Significant difference (p<0.05) in the mean number of labelled IELs: *between patients with ACD and RCS; †between patients with GFD-CD and RCS.

Immunohistochemical labelling with anti-CD3 (A, C, E, G) and anti-CD8 (B, D, F, H) in gastric (A, B, E, F) and colonic (C, D, G, H) biopsy samples from a patient with refractory coeliac sprue (RCS) (A–D) and a patient with active coeliac disease (ACD) (E–H), showing increased numbers of intraepithelial T lymphocytes in RCS (mostly positive for CD3 (A, C) but negative for CD8 (B, D)) and in ACD (mostly positive for both CD3 (E, G) and CD8 (F, H)). Original magnification ×200.
CD3 staining confirmed the rates of LG and LC obtained by histological analysis of gastric and colonic samples in the three groups. We found no significant difference between CD3+ IEL numbers in gastric and colonic samples from RCS, ACD, and GFD-CD patients. In contrast, median percentage of CD3+ CD8− IELs in LG and LC samples was significantly higher in the RCS group than in either of the two CD groups. Gastric and colonic samples from RCS patients with LG and LC always contained IELs with an abnormal phenotype, and the median proportion of CD3+CD8− IEL ranged from 54% to 100% (mean 83%) (fig 1).
Molecular analysis
Results of TCR-γ gene rearrangement analysis for the four biopsied sites and the three patient groups are summarised in tables 2 and 3. Figure 3 (A–C) shows cases of monoclonal and/or polyclonal TCR-γ gene rearrangements in RCS and CD.
Percentage of T cells with monoclonal T cell receptor γ (TCR-γ) gene rearrangements in patients with refractory coeliac sprue (RCS) and two groups of patients with coeliac disease (CD) (active coeliac disease (ACD) and coeliac disease on a gluten free diet (GFD-CD)) in gastric, colonic, and blood samples
Results of T cell receptor γ (TCR-γ) gene rearrangement analysis in gastric and colonic samples from patients with refractory coeliac sprue (RCS), according to the presence or absence of lymphocytic gastritis and lymphocytic colitis

{kind=link}
{kind=link}
{kind=link}
GeneScan analysis of polymerase chain reaction (PCR) T cell receptor γ (TCR-γ) amplicons from DNA extracted from gastric, duodenal, jejunal, and colonic samples (A, C) and blood, duodenal, and gastric samples (B) from two patients with refractory coeliac sprue (RCS) (A, B) and one patient with active coeliac disease (ACD) (C). Both patients with RCS had biallelic monoclonal amplicons of the same length at all sites studied (in (A), a V9-J11 biallelic rearrangement of 228 and 238 base pairs and in (B), a biallelic rearrangement Vf1+V10 of 245 base pairs (top) and a V9-JII of 110 base pairs (bottom)). The patient with ACD had a polyclonal TCR-γ gene rearrangement in Vf1-V10 multiplex PCR (C1) and V9-V11 multiplex PCR (C2).
We found a monoclonal TCR-γ rearrangement in 8/13 (62%) and 8/10 (80%) of gastric and colonic samples, respectively, from RCS patients, but in only 2/25 (8%) and 0/7 (0%) samples overall in the two CD groups (p<0.05). All monoclonal bands detected in gastric and colonic samples from RCS patients had the same length as those found in corresponding duodenojejunal samples (fig 3A). Interestingly, among RCS patients, all but one of eight patients with LG and all six patients with LC had a monoclonal population compared with only 1/4 and 2/4 gastric and colonic samples from patients without LG and LC, respectively. Among the eight patients with a monoclonal population in the colonic mucosa, six gastric samples yielded the same monoclonal band and one yielded a polyclonal band (the last sample was not studied).
Investigation of TCR-γ gene rearrangements in blood cells revealed a monoclonal band identical in size to that of duodenojejunal, gastric (fig 3B), or colonic samples in four (44%) of nine RCS patients. We have previously described two of the four monoclonal blood samples studied here10 and one of the polyclonal blood samples.10 All four patients with a circulating monoclonal population had monoclonal LG and/or LC, while only two of the five patients with a circulating polyclonal population had monoclonal LG and/or LC.
In the two CD groups, two patients with monoclonal patterns of the TCR-γ gene rearrangement were found in one gastric sample from each CD group and were not associated with a monoclonal population in the duodenal and jejunal samples tested. The first patient (with ACD) had a minor Vf1 monoclonal TCR-γ rearrangement and LG. The second patient (with GFD-CD) had a Vγ9 monoclonal TCR-γ rearrangement and was free of LG (not shown).
DISCUSSION
This study confirms that CD is associated with diffuse epithelial T cell infiltration at all levels of the gastrointestinal tract. However, we found a higher incidence of LG and LC in patients with ACD and GFD-CD than previously described (10–45% LG and 19–31% LC).2–5 The IEL phenotype was normal in CD patients with LG and LC, in keeping with previous studies.22–24 The only two samples yielding monoclonal profiles in CD patients were from the stomach, and may have been due to the limited diversity of the T cell repertoire in human IEL.25
After excluding overt intestinal lymphoma, detection of an aberrant IEL phenotype (iCD3ε+ chain but no sCD3ε, TCR, CD4, or CD8), coupled with a monoclonal T cell rearrangement, confirms a diagnosis of RCS.10 In the present study, the monoclonal phenotypically abnormal IEL population observed in the duodenal and jejunal mucosa of RCS patients was also found in the stomach and colon. The prevalence of LG (64%) and LC (55%) in our RCS patients, based on gastric and colonic biopsy, was higher than reported by Robert et al (respectively, 33% (2/6) and 0% (0/8)).15 The percentage of CD3+CD8− IELs was always abnormal (>52%) in samples from RCS patients with LG and LC, and was significantly higher than in either CD group, as previously observed in duodenojejunal samples.9–11 The calculated proportion of CD3+ CD8− IELs in RCS patients was similar to that found by Bagdi et al using a double anti-CD3 and anti-CD8 staining method.13
We found a link between monoclonal TCR-γ rearrangements and the presence of LG or LC in RCS patients. Seven of eight gastric samples from RCS patients with LG were associated with a monoclonal T cell population (positive predictive value 87.5%) whereas four of the five gastric samples from RCS patients without LG had a polyclonal gene rearrangement (negative predictive value 80%).
In the colonic mucosa of RCS patients, all six cases of LC were associated with a monoclonal T cell population, and the positive predictive value of TCR-γ analysis was 75% (6/8). In contrast, 50% (2/4) of colonic samples from RCS patients without LC had a polyclonal gene rearrangement (negative predictive value 100%). The difference between the size of the abnormal population detected by molecular and immunohistochemical methods is probably due to the better sensitivity of the molecular approach.
The monoclonal population detected in RCS was stable. Indeed, the monoclonal T cell population persisted in seven patients biopsied 2–4 times at duodenal and jejunal sites during a period of 1–6 years (mean 3.3 years), and in three patients biopsied twice at a gastric site during a period of 1–2 years. A polyclonal population was detected on three occasions in gastric samples from the same patient (not shown).
A link between gastric and colonic extension was observed. Diffusion of the abnormal monoclonal population was detected simultaneously in colonic and gastric samples from six RCS patients on the basis of TCR-γ gene rearrangement, and in five patients on the basis of IEL counts and immunohistochemistry. A link between LG and LC has previously been observed in 38% (5/13) to 50% (2/4) of patients with CD.3,5 Comparison of clonality in contemporary blood and gastrointestinal samples showed concordance in 7/9 patients (78%); four of these cases were monoclonal and three were polyclonal. None of the patients had a monoclonal circulating profile or a polyclonal gastrointestinal profile while the reverse situation was seen in two cases. These data suggest that gastric and colonic monoclonal profiles do not result from contaminating circulating lymphocytes in intestinal samples. This is confirmed by the correlation between TCR-γ clonality and histological findings. Among the five patients with a high percentage of circulating CD103+CD3− lymphocytes (20–83%, mean 39%), one of whom also had hyperlymphocytosis, four had a monoclonal blood sample.
RCS is associated with a poor outcome and appears to carry a higher risk of ulcerative jejunitis and EITCL compared with CD.10,26 The latter is aggressive, and is the most common primary gastrointestinal T cell tumour arising from intraepithelial T cell lymphocytes.27,28 Several molecular studies have shown the link between RCS and subsequent EITCL. Identical clonal rearrangements are found in the duodenal mucosa of patients with RCS who subsequently develop overt T cell lymphomas, and also in patients who develop ulcerative jejunitis.6,9,10,12,13,17 Moreover, phenotypic abnormalities identical to those found in RCS have been demonstrated in IEL distant from EITCL.6,29 EITCL essentially arise in the small intestine but other sites have been described, such as mesenteric lymph nodes, skin, and liver.9,10,26 Only very rare cases of EITCL involving the stomach and colon have been described30–32 and most were associated with or contiguous to a site in the small intestine.26,33 The lack of relevant clinical and pathological data in the rarely reported cases of primary gastric or colorectal T cell lymphoma makes it impossible to determine the exact incidence of EITCL. Evidence of such a case has been reported in a CD patient who developed multiple refractory gastric ulcers associated with a small intestinal lymphoma,34 while an RCS patient developed intestinal overt lymphoma associated with ulceration throughout the gastrointestinal tract, including the stomach.17 Moreover, two reports describing four cases of gastric T cell lymphoma suggested that the tumour cells were derived from IELs, on the basis of CD103 expression or marked epitheliotropism.35,36
Therefore, although gastric and colonic EITCL is rare, the presence of an abnormal monoclonal IEL population in gastric and colonic biopsy samples from RCS patients requires close follow up to detect subsequent development of overt T cell lymphoma. The presence of a monoclonal aberrant T cell IEL population disseminated throughout the gastrointestinal epithelium in RCS reinforces the hypothesis of malignancy in this setting. Mechanisms of diffusion and expansion of this population have been poorly understood until now. A recent study suggests that interleukin 15 may play a key role in IEL expansion in RCS (Mention et al, submitted).
In conclusion, this study shows that the monoclonal phenotypically aberrant IEL population present in the small intestine of patients with refractory coeliac sprue frequently disseminates to the gastric and colonic mucosa and to the blood. Molecular evidence that morphologically benign IELs in the gastric and colonic mucosa may harbour a monoclonal T cell population suggests that RCS is a diffuse gastrointestinal process.
Acknowledgments
We thank J-P Monnet for his technical assistance, the French Coeliac Disease Study Group for recruitment of refractory sprue patients, Professor JC Delchier for providing data on a patient with RCS, and E Delabesse for his help with molecular studies. This work was supported by the PHRC AOM96082 and the Fondation Grâce de Monaco.