Article Text

Abstract
Non-steroidal anti-inflammatory drugs (NSAIDs) are well recognised as causing peptic ulceration and ulcer complications. However, several critical issues, including the amount of both gastrointestinal and non-gastrointestinal disease affected by NSAIDs, their interaction with ancillary risk factors, and how to optimise management in subgroups, remain poorly understood. In this article, strategies for subgroups that take account of non-specific gastrointestinal risks, minimisation of residual risk, and the importance of non-gastrointestinal toxicity are suggested, and areas for research identified.
- non-steroidal anti-inflammatory drugs
- ulcers
- proton pump inhibitors
- misoprostol
- COX-2 inhibitors
- aspirin
- myocardial infarction
- NSAIDs, non-steroidal anti-inflammatory drugs
- COX, cyclooxygenase
- PPI, proton pump inhibitor
- NNT, number needed to treat
Statistics from Altmetric.com
- non-steroidal anti-inflammatory drugs
- ulcers
- proton pump inhibitors
- misoprostol
- COX-2 inhibitors
- aspirin
- myocardial infarction
- NSAIDs, non-steroidal anti-inflammatory drugs
- COX, cyclooxygenase
- PPI, proton pump inhibitor
- NNT, number needed to treat
SUMMARY
The gastrointestinal consequences of non-steroidal anti-inflammatory drugs (NSAIDs) are the best recognised iatrogenic problem in clinical medicine. Although considerable, these gastrointestinal problems are overestimated in many studies, partly because association and cause are not always distinguished. An attributable rate of hospitalisation greater than 1 per 100 patient years is unlikely, even in patients over 60 years of age. Conversely, non- gastrointestinal adverse events, including fluid retention and its consequences, have until recently been relatively neglected. Selective inhibitors of the inducible cyclooxygenase (COX)-2 enzyme are important new therapies which, by sparing COX-1, undoubtedly reduce the risk of upper gastrointestinal bleeding caused by NSAIDs, and may abolish it, leading to extremely low event rates in patients without other risk factors. Recommendations to use COX-2 inhibitors in high risk patients unduly discounts this ability to minimise residual risk in low risk patients and may be misplaced if the potential of proton pump inhibitor (PPI) prophylaxis to reduce non-specific as well as NSAID specific risk is shown to lead to lower overall event rates in such individuals. In this article, strategies for subgroups that take account of non-specific gastrointestinal risks, minimisation of residual risk, and the importance of non-gastrointestinal toxicity are suggested, and areas for research identified. The possibility that ibuprofen ⩽1200 mg daily may offer comparable overall safety, especially when combined with a PPI for defined patients, warrants formal evaluation. The extent and nature of NSAID or COX-2 inhibitor interactions with aspirin in influencing both cardiovascular and gastrointestinal outcomes needs clarifying.
INTRODUCTION
Non-steroidal anti-inflammatory drugs (NSAIDs) are well recognised as causing peptic ulceration and ulcer complications. The advent of effective protective therapies, such as co- prescription of misoprostol or PPIs or use of safer NSAIDs, including COX-2 inhibitors, makes this information of practical importance. However, several critical issues, including the amount of both gastrointestinal and non-gastrointestinal disease affected by NSAIDs, their interaction with ancillary risk factors, and how to optimise management in subgroups, remain poorly understood. No protective strategy has yet demonstrated an overall reduction in death or critical life threatening event rates. To achieve this may require application of different approaches, taking account of all toxicities, to different subgroups of patients. In this article, we will try to provide best evidence assessment of the risks of NSAIDs and the net benefits of protective strategies, both overall and in subgroups, in an attempt to define strategies that could lead to net health benefit.
AMOUNT OF GASTROINTESTINAL DISEASE ATTRIBUTABLE TO NSAID USE
Estimates from epidemiological studies
Estimates of the amount of disease attributable to NSAIDs have varied widely. This may be because distinctions are not made between causal and non-causal associations or because estimates based on events observed in high risk populations are assumed to apply generally. Bleeding accounts for most serious ulcer pathology. Based on a widely quoted population study,1 it can be estimated that there are 8528 hospitalisations for gastric and duodenal ulcer bleeding per annum in the UK.2 Based on estimates that between 20% and 25% are causally associated with intake of non-aspirin NSAIDs, and approximately 10% more with aspirin used for cardiovascular prophylaxis, these figures suggest that (aspirin and non-aspirin) NSAIDs cause approximately 3500 hospitalisations for and 400 deaths from ulcer bleeding per annum in the UK in those aged 60 years and above.2
“NSAIDs cause approximately 3500 hospitalisations for and 400 deaths from ulcer bleeding per annum in the UK in those aged 60 years and above”
There are approximately 10 million people aged 60 years and over in the UK and about 15% (1.5 million) take NSAIDs at any time, thus implying an annual attributable rate of hospitalisation of 0.23% and of death of 0.027% for NSAID induced ulcer bleeding (table 1). Another population based study estimated that one episode of ulcer bleeding attributable to NSAIDs occurred in the elderly per 2828 prescriptions,3 implying that just over 4000 hospitalisations per annum are causally related, based on 12 million NSAID prescriptions per annum in the elderly. If one prescription is taken to last one month, a rate of ulcer bleeding of 0.4/100 patient years in the elderly can be deduced (table 1).
Estimated rates of hospitalisation and death from non-steroidal anti-inflammatory drug (NSAID) attributable gastrointestinal disorders
Mortality statistics within the UK attribute just under 3500 gastric and duodenal ulcer deaths per annum in those over 60 years to peptic ulcer and its complications of all types.4 If 20–25% are due to non-aspirin NSAIDs, the implied death rate due to these drugs is between 700 and 900 per annum. This is somewhat higher than estimates from population based studies but includes perforation, sudden death with bleeding in the community, and any oesophageal ulcer deaths attributable to NSAIDs. Overall, it seems that NSAID induced ulceration may cause no more than 1000 deaths per annum in the UK and that quoted event rates of 1–4% per annum and theoretical calculations of 2000 deaths per annum5 are overestimates.
For reasons that are unclear, higher estimates come from the USA where 1.25 excess gastrointestinal hospitalisations per 100 patient years has been calculated for NSAID users in the Tennessee Medicaid Program (table 1).6 One reason could be that patients are more readily admitted for ulcer associated events with a lower mortality in the USA than in the UK. However, there is no direct evidence that this is so, and UK figures applied pro rata would imply no more than 5000 deaths caused per annum in the USA while “conservative estimates” of “at least 16 500” NSAID associated deaths have been calculated.7,8 It is difficult to believe that these estimates are in fact conservative, even allowing for high rates of non-causal association, as only 6500 deaths per annum are recorded with peptic ulcer as the primary cause, and another 11 000 where it has been the secondary diagnosis.9,10
Estimates from clinical trials
Three large cohort studies have been fairly consistent in estimating the total risk of hospitalisation for gastrointestinal complications associated with NSAID use as between 1.3 and 2.2 events per 1000 patient years. However, not all of these NSAID associated events are caused by NSAIDs. Differences in rates of hospitalisation for patients on NSAIDs compared with coxibs may approximate to those caused by NSAIDs if coxibs do not cause ulcers. In the VIGOR study, this excess was 0.7 events per 100 patient years (table 1).11 Values from CLASS12 are of a similar magnitude but less informative because of concomitant aspirin use and uncertainty about the status of the published data which encompass only part of the study.13–15 Overall clinical trials, in populations both within and outside of the USA, yield estimates of risk that are quite similar to those from epidemiological studies from the UK.
AMOUNT OF NON-GASTROINTESTINAL DISEASE ATTRIBUTABLE TO NSAID USE
As well as their effects on the upper gastrointestinal tract, NSAIDs can also cause lower intestinal haemorrhage or perforation16 and may exacerbate colitis.17 In addition, common non-gastrointestinal adverse effects include the consequences of salt and water retention, renal failure, provocation of bronchospasm, and hypersensitivity reactions. Of these, the propensity of non-selective and selective NSAIDs to induce salt and water retention has received increasing attention,18–22 as has speculation about antiplatelet effects.23,24
Salt and water retention
Although NSAIDs affect renal blood flow, their most consistent effect is in enhancing renal sodium reabsorption as a result of cyclooxygenase (largely COX-2) inhibition predisposing to hypertension and oedema.20 Large meta-analyses suggest that NSAID treatment elevates blood pressure by an average of 3–5 mm Hg (fig 1).25,26 The Framingham studies and others examining the annual risk of cardiovascular events suggest that these increase in a linear fashion by approximately 4/1000 per 5 mm Hg rise in blood pressure,27 implying a substantial effect of NSAIDs, which is supported by a case control study of patients admitted with heart failure.28 Applied to the 1.5 million NSAID users aged 60 years and over in the UK, these figures would suggest that NSAIDs might cause as much cardiovascular disease as a consequence of drug induced hypertension as they do ulcer complications.
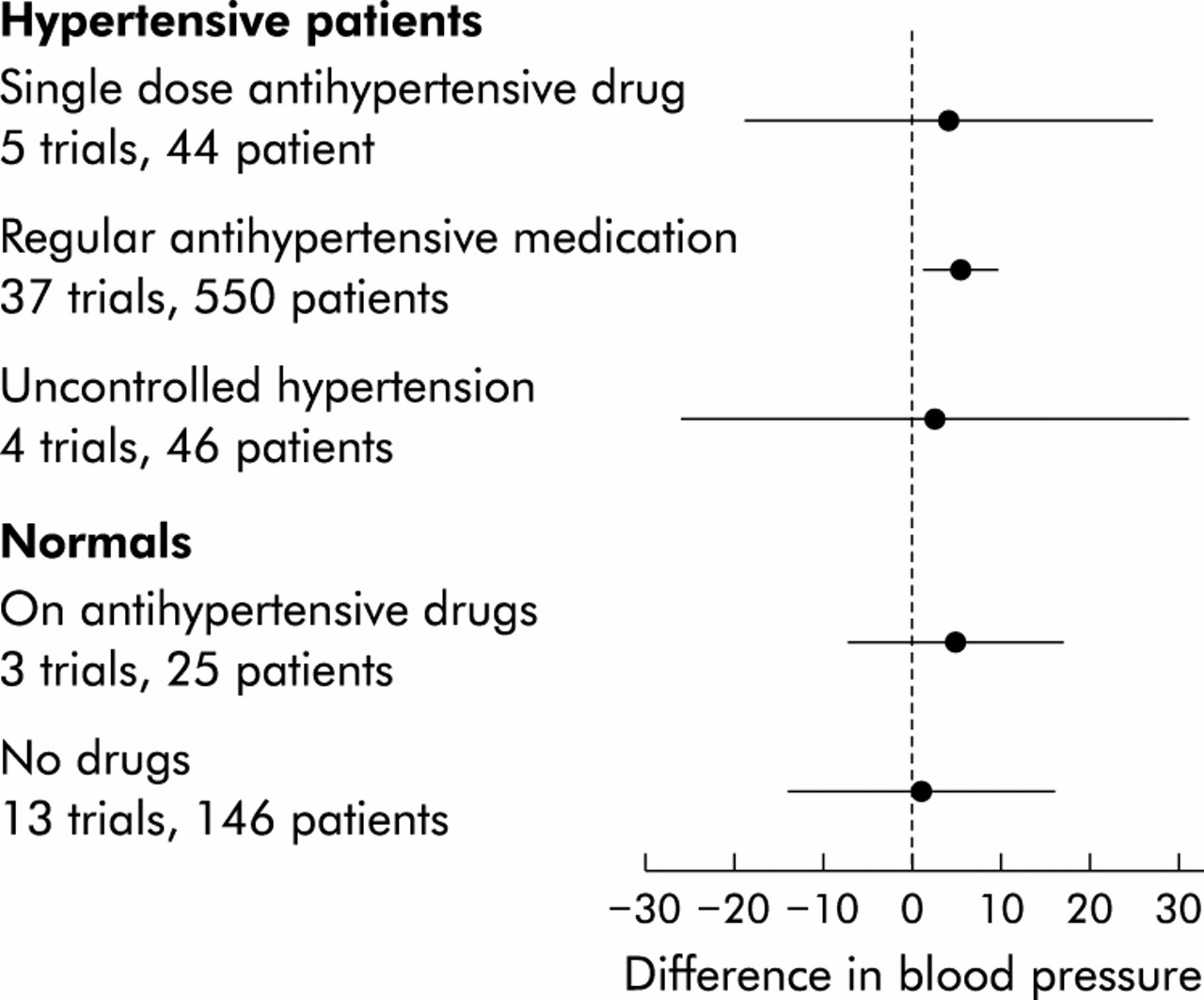
Effects of non-steroidal anti-inflammatory drugs on blood pressure (relative risk and 95% confidence intervals), based on Johnson and colleagues25(reproduced with permission). The largest body of data concern hypertensive patients.
Effect of aspirin and non-aspirin NSAIDs on thrombotic complications of vascular disease
As a result of prolonged profound irreversible inhibition of platelet thromboxane, aspirin is well recognised as reducing thrombotic complications of vascular disease.29,30 Non- aspirin NSAIDs also inhibit platelet thromboxane, usually less potently, reversibly, and for a shorter time than aspirin.24 NSAIDs also inhibit vascular prostacyclin synthesis, making it difficult to predict what effect they would have on thrombosis.18,31 Results of studies on the relationship between NSAIDs and myocardial infarction conflict,32–39 but it seems that any overall effect of NSAIDs on thrombotic disease may at best be small. This net effect could arise because NSAIDs generally have insufficient antiplatelet activity to prevent coronary thrombosis or because limited antithrombotic activity counterbalances adverse effects on vascular prostacyclin and blood pressure.
Interactions between aspirin and non-aspirin NSAIDs
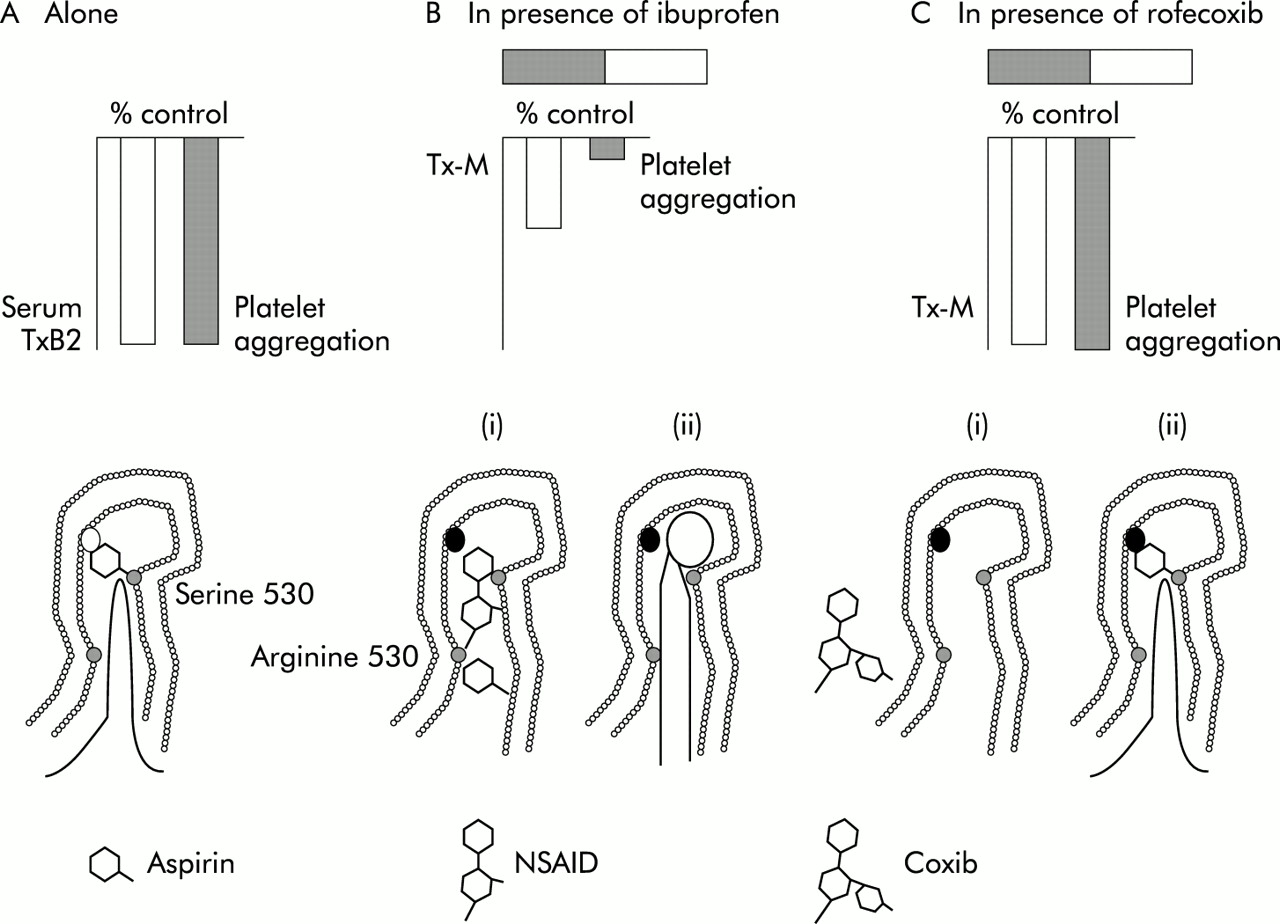
Potentially more important is the recent report that ibuprofen, and possibly other NSAIDs, can abolish the ability of aspirin to inhibit platelet aggregation.40 Mechanistically this may arise because ibuprofen binds (reversibly) to platelet cyclooxygenase long enough to impede access of aspirin to the site that it normally acetylates, to inhibit platelet cyclooxygenase irreversibly (fig 2). Because a substantial number of patients take both aspirin and NSAIDs, it will be important to test directly the implication of this pharmacodynamic study, that patients might lose the cardioprotective effects of aspirin when taking at least some NSAIDs.
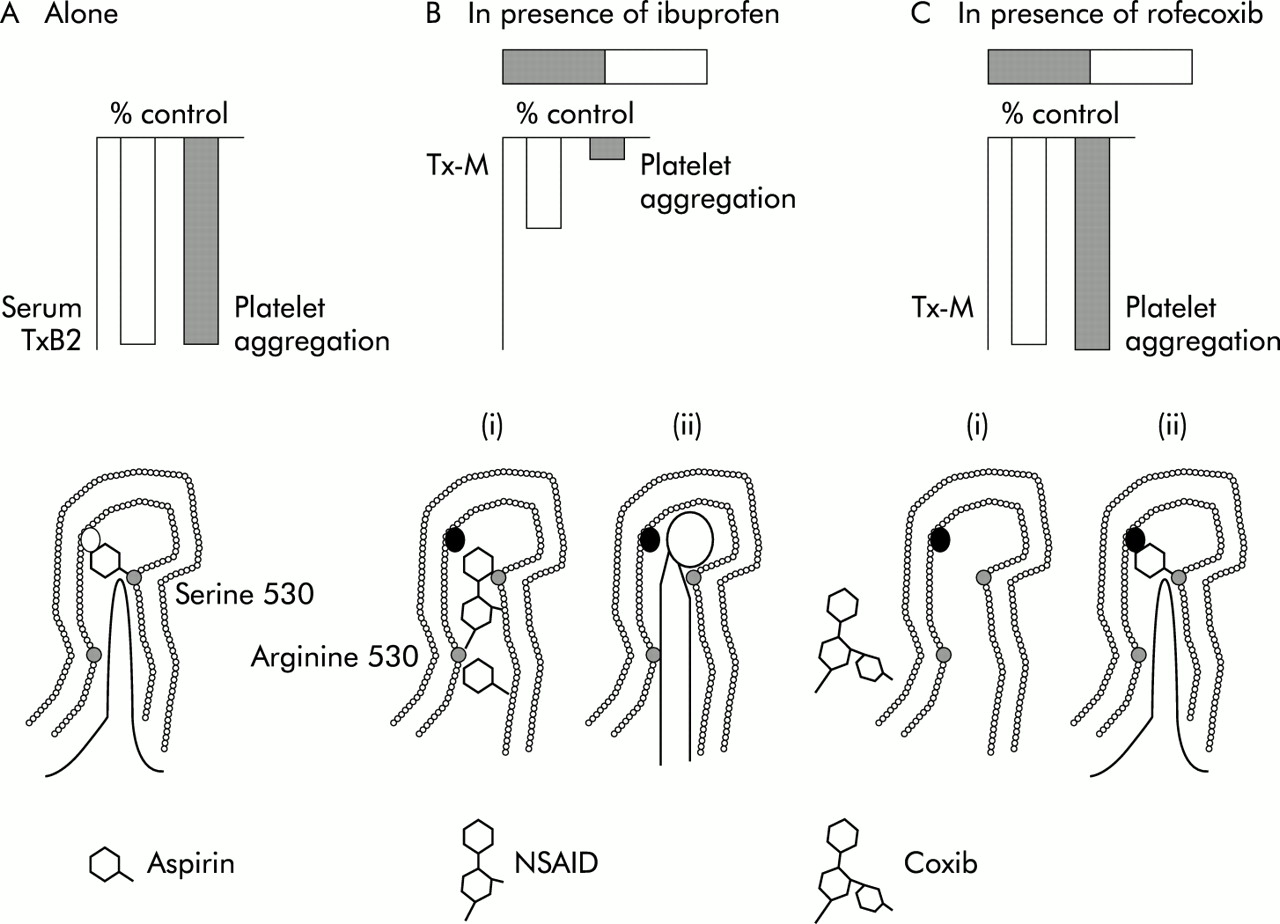
Interaction between aspirin, ibuprofen, and rofecoxib, based on Catella-Lawson and colleagues.63 (A) Aspirin 81 mg reduces serum thromboxane (TxB2) by ⩾98% and platelet aggregation by 98% (at 24 hours). It does this by binding irreversibly to serine 530 and blocking entry of arachidonic acid (bottom panel). (B) When ibuprofen 400 mg is given two hours before aspirin, serum thromboxane is only reduced by 53% at 24 hours and platelet aggregation is not affected, probably because ibuprofen, by reversibly binding to arginine 120, temporally impedes access of aspirin to serine 530 (bottom panel (i)). As a result, thromboxane can subsequently be synthesised allowing normal platelet aggregation (bottom panel (ii)). (C) After rofecoxib 25 mg, the effect of aspirin is unchanged. This may be because rofecoxib, because of its selectivity, means it does not access platelet cyclooxygenase and cannot impede aspirin in the same way as ibuprofen (bottom panel (i)). Consequently, aspirin can bind to serine 530 (bottom panel (ii)). NSAID, non-steroidal anti- inflammatory drug.
PROTECTIVE STRATEGIES
These concern either co-prescription of a protective drug such as misoprostol or a PPI, or substitution of a drug with reduced toxicity. Previously, paracetamol and ibuprofen were regarded as the safer drugs for consideration41 but recent attention has highlighted COX-2 selective inhibitors that combine high potency with substantial gastrointestinal safety.
COX-2 INHIBITORS
Many have focused on the question of who should receive selective COX-2 inhibitors in preference to non-selective NSAIDs. Consensus statements have consistently recommended that selective COX-2 inhibitors should be used in patients with high but not low risks of gastrointestinal complications.42–44 However, whether this is appropriate depends on how different is the overall safety of selective and non-selective agents, the degree to which high risk patients contribute to the overall burden of NSAID induced gastrointestinal complications, and the extent to which their increased risk is NSAID specific as opposed to a general risk that would still continue to apply without NSAIDs.
Impact of COX-2 inhibitors on gastrointestinal disease
In 3–6 month endoscopy studies, the selective COX-2 inhibitors rofecoxib and celecoxib have been associated with a fourfold reduction in ulcers detected by endoscopy, even at high dose, by comparison with normal doses of standard NSAIDs.40,45–50 Broadly similar results have been seen with newer COX-2 inhibitors.51,52 High doses of rofecoxib and celecoxib have been subject to large scale prospective outcomes studies. In the VIGOR study, clinically significant ulcers were reduced by 54% and ulcer complications by 57%,11 a result compatible with estimates from large scale analysis of osteoarthritis trials.53
“Rofecoxib and celecoxib have been associated with a fourfold reduction in ulcers detected by endoscopy, even at high dose, by comparison with normal doses of standard NSAIDs”
Assessment of celecoxib is more complicated. Combined analysis of complications in endoscopic studies suggested substantial reductions,49 as did an initial publication of partial data from the CLASS study.12 The final negative result for the trial as a whole13–15 is likely to have arisen because of problems of trial design rather than lack of safety. Recent data suggest that the incidence of clinical lower gastrointestinal events is also reduced with COX-2 inhibitors54 (Laine et al 2002, Annals Intern Med (submitted)).
Impact of COX-2 inhibitors on non-gastrointestinal disease
Selective COX-2 inhibitors cause sodium and water retention, hypertension, and oedema, with effects broadly similar to those of non-selective NSAIDs when compared at equivalent doses.18,19,21,22,55 Suggestions that celecoxib lacks these mechanism dependent effects56 seem likely to arise because of dose confounding and/or differences in absorption characteristics and half life.55
Thrombotic complications of vascular disease
The summary bases for approval of celecoxib and rofecoxib showed no increases in cardiovascular event rates in osteoarthritis patients (about 4000 patients for each drug).57,58 However, in the VIGOR study, patients receiving rofecoxib 50 mg (a supratherapeutic dose) had a significantly higher rate of cardiovascular events than those receiving naproxen 1g daily,11 an ad hoc finding whose uncertain significance has overshadowed the important gastrointestinal primary end point of the study.59 Plausible explanations include an antithrombotic effect of naproxen (which differs from other NSAIDs in consistently achieving platelet inhibition that is sufficiently prolonged and profound to be truly aspirin- like60), a prothrombotic effect of unopposed inhibition of prostacyclin derived from endothelial COX-2 by a supratherapeutic dose of rofecoxib,18 or susceptibility of rheumatoid arthritis patients to the adverse cardiovascular events of the drug. There are no firm data that distinguish these possibilities, although this has not inhibited a flurry of unjustifiable speculation23,59 and controversy.61 Some studies38,39 support a protective effect of naproxen, others35 do not. No studies of normal (as opposed to supratherapeutic) doses of selective COX-2 inhibitors, including placebo comparisons, suggest that the rate of myocardial infarction is increased (fig 3).59 It will take time for the issues to be effectively addressed, for instance through comparison of cardiovascular adverse event rates in placebo controlled trials of COX selective NSAIDs in treating Alzheimer’s disease or those at risk of gastrointestinal cancer.

{kind=link}
{kind=link}
{kind=link}
Vascular events on rofecoxib (relative risk and 95% confidence intervals) compared with placebo, non-naproxen non-steroidal anti-inflammatory drugs (NSAIDs), and naproxen, assessed by the Antiplatelet Trialists’ Collaboration (APTC) end point (cardiovascular haemorrhagic and unknown death, non-fatal myocardial infarction, and non- fatal stroke). The increased rate seen in the VIGOR trial with rofecoxib 50 mg compared with naproxen is not seen for therapeutic doses of rofecoxib compared with either placebo or other NSAIDs. Reproduced from Konstam and colleagues59 with permission.
Interactions between COX-2 inhibitors and low dose aspirin
The CLASS study is of interest because in the 21% of patients who took low (ish) doses of aspirin (325 mg or less) an advantage of reduced peptic ulcer rates for celecoxib was not demonstrable over its NSAID comparator.12 It is unclear whether what was found represents the play of chance, distortion by post hoc analysis, intrinsic toxicity of aspirin, or synergism between COX-1 and COX-2 inhibition.62 Parallel data on rofecoxib are not available. The small size of the dataset within CLASS should have deterred over-interpretation, but has not. Moreover, because of their selectivity, coxibs are unable to enter the platelet COX-1 channel, and rofecoxib appears to lack the ability of ibuprofen to interfere with the antiplatelet activity of aspirin, a mechanistic difference that could be advantageous.40,63
ALTERNATIVES TO COX-2 SELECTIVE INHIBITORS
An impressive aspect of the data on COX-2 inhibitors is that full and supratherapeutic doses have been shown to have less gastrointestinal toxicity than full doses of non-selective NSAIDs. It has not been proved that overall safety is increased, nor that gastrointestinal safety is better than lower doses of non-selective NSAIDs. As ibuprofen is commonly used at low doses (⩽1200 mg/day), the data on COX-2 selective inhibitors need consideration in relation to the overall value of ibuprofen as well as paracetamol, both being generally considered relatively safe.
Paracetamol
Paracetamol has usually been regarded as safe within the gastrointestinal tract but it has demonstrable, although weak, ability to inhibit prostaglandin synthesis.64,65 A well recognised association with ulcer complications was assumed to represent consumption in response to gut symptoms,66 an assumption supported by the temporal relationship between ingestion and ulcer bleeding.67
“Paracetamol has usually been regarded as safe within the gastrointestinal tract but it has demonstrable, although weak, ability to inhibit prostaglandin synthesis”
Recent data generated in an automated database has been used to suggest that paracetamol has dose dependent toxicity in the gut.68 These data are weakened by not including self purchased paracetamol, which accounts for most use, and the suggestion that paracetamol is harmful runs counter to other epidemiological evidence (table 2),66,67,69 seems to have been generated as a byproduct of an examination of the safety of newer NSAIDs (where paucity of data prevented conclusions), and may yet have arisen because of confounding of drug use and indication for treatment. Nevertheless, although paracetamol is probably safer than NSAIDs, this is currently sub judice.
Dose dependent risks for paracetamol and selected non-steroidal anti-inflammatory drugs for upper gastrointestinal bleeding
LOWER TOXICITY NSAIDS
Many epidemiological studies show that ibuprofen use is associated with a halving of ulcer complication rates compared with average expectation for NSAID users.41 This reflects relatively low potency and formulation that allows prescription of low doses, but the short half life of ibuprofen combined with its acidic nature can achieve selective trapping within joints70,71 and so contribute additionally to a good efficacy to safety ratio. At doses of ⩽1200 mg/day, gastrointestinal risks may not be significantly increased above background (table 2),69 although this advantage is lost at higher doses.
Although a post hoc analysis of CLASS suggested diclofenac did not differ from celecoxib in risk58,72 epidemiological studies do not clearly support a separation from NSAIDs as a whole.41 As the effects of NSAIDs on sodium retention are dose dependant, low doses of ibuprofen may cause less hypertension and oedema.73 The reduction of risk during routine clinical use of ibuprofen is such that comparisons of safety (both gastrointestinal and non-gastrointestinal) and efficacy of reduced doses of ibuprofen (⩽1.2 g daily) with COX-2 inhibitors seem worth considering.
Avoiding NSAIDs with more harmful gastrointestinal toxicity profiles
Restricting prescribing of particularly toxic NSAIDs could achieve as much as encouraging choice of lower risk drugs. Use of azapropazone was restricted in the UK in 1994 because of observed toxicity, and a similar approach could be taken with other drugs perceived as being high risk. Although analysis of spontaneous adverse reaction reports suggested in the past that piroxicam did not differ materially from other NSAIDs in ulcerogenicity,74 there is consistent evidence from the UK and elsewhere that it is particularly likely to cause ulcer complications (table 2).41,75 Unequivocal decisions about other drugs, such as ketoprofen,75 are hindered by widely varied assessments of toxicity,41 which may result from differing dose levels generally employed.
CO-PRESCRIPTION OF GASTROPROTECTIVE DRUGS
Misoprostol
Much endoscopic evidence shows that misoprostol protects against gastroduodenal damage from NSAIDs.76 The clinical relevance of these findings is underpinned by the direct demonstration in the MUCOSA study that hospitalisation for ulcer complications was also reduced by 40%.77 Unfortunately, a high frequency of symptomatic adverse gastrointestinal events limits use of misoprostol.
PPIs
In endoscopic studies, PPIs are very effective in healing NSAID associated gastric and duodenal ulcers, and in preventing relapse.78–80 When used in patients continuing to take naproxen or aspirin after hospitalisation for ulcer bleeding, PPIs reduce later ulcer bleeding by 4–6-fold more compared with Helicobacter pylori eradication.81,82 Limited endoscopic, but not outcome, data suggest similar protection in patients without initial ulcers.83,84 A weakness of PPIs is that they are unlikely to reduce lower gastrointestinal risks.
Avoiding H2 receptor antagonists
Normal doses of H2 antagonists do not effectively prevent NSAID induced gastric ulcers.85 Indeed, those on H2 antagonists have an increased rate of ulcer bleeding, possibly because of masking of warning symptoms.86 With falling cost of PPIs, there will be little justification for use of H2 antagonists, even for dyspepsia, in NSAID users.
APPROACH TO MANAGEMENT OF SUBGROUPS
Consensus statements and economics
Five circumstances under which use of COX-2 selective inhibitors is recommended by the National Institute for Clinical Excellence (NICE) in the United Kingdom44 are: prolonged use of standard NSAIDs at maximum recommended doses; patients aged 65 years and over; patients with previous ulcer complications; patients whose co-medications (for example, corticosteroids, anticoagulants) increase the likelihood of upper gastrointestinal adverse events; and where there is serious comorbidity.
“Restrictions on use of selected COX-2 inhibitors arise because of their cost”
A broadly similar approach is taken by other consensus and guideline recommendations.42,43 Restrictions on use of selected COX-2 inhibitors arise because of their cost. Similar considerations apply to PPIs, but a fall in price is likely to make a non- selective NSAID plus a PPI cheaper than a COX-2 inhibitor, making comparative judgements between the two strategies timely. Additionally, lower prices would make the combination of a PPI and a COX-2 inhibitor a cost effective strategy for very high risk patients as these are generally at risk even when not taking NSAIDs.87
OBTAINING OVERALL POPULATION BENEFIT: RISK REDUCTION AND RESIDUAL RISK
Consensus methods applied to NSAID prescribing can, by focusing on high risk groups, result in strategies that reduce the number needed to treat (NNT) to achieve benefit. However, highly focused strategies leave large numbers of patients perceived as at lower risk unprotected and overall population benefit is small. Moreover, most of the accessory factors that raise risk in patients taking NSAIDs also do so in patients that do not use these drugs87 so that the continued impact of ancillary non-drug risk factors may still leave NSAID users at unacceptably high residual risk even when switched to safer alternatives. It follows that any satisfactory protective strategy must take account of overall risks in both users and non-users of NSAIDs and the reasons why some patients are at particular risk. Such strategies are likely to include the use of PPIs, and of low dose standard NSAIDs as well as of COX-2 inhibitors.
Management of patients without ancillary risk factors
Low risk patients are not generally considered as targets for use of selective COX-2 inhibitors. Yet from the point of view of residual risk, they are most logically the recipients of such treatment as their risk of ulcer disease, when using non-selective NSAIDs, in theory derives solely from such drug use, making it possible that low risk patients could become no risk patients. Trial data support this notion. In VIGOR, rates of ulceration in patients without specified risk were reduced by 88% from 1.9 (on naproxen) to 0.2 per 100 patient years on rofecoxib. In CLASS, comparable figures (six month data) were 1.35 per 100 patient years (non-selective NSAIDs) and 0.35 per 100 patient years (celecoxib).
“Epidemiological studies suggest that reducing NSAID doses reduces risk”
Epidemiological studies suggest that reducing NSAID doses reduces risk,41,88 possibly to background levels with ibuprofen ⩽1200 mg/day.69 It therefore follows that direct comparison of low dose ibuprofen and a COX-2 inhibitor for safety and efficacy in this group of patients would be worthwhile if the size were not to daunting.
MANAGEMENT OF PATIENTS WITH ANCILLARY RISK FACTORS
For many high risk patients an all embracing preventive strategy is logically more appropriate by reason of the influence of non-NSAID related risk factors.
Past ulcer history
Most (but not all) studies suggest that a prior history of peptic ulcer increases the risk of ulcer complications whether patients do or do not use NSAIDS. Moreover, risk remains high, at least for endoscopic ulcers, even when patients stop taking NSAIDs.89 As this persisting risk appears to affect both H pylori negative and positive patients, and to be site preferential,90,91 it is likely to reflect some local vulnerability of the mucosa at the site of prior ulceration.
Magnification of a high background risk in patients with a past ulcer history who use NSAIDs results in particularly high rates of ulcer complications.92–94 Consequently, risk reductions in such patients switched from a non-selective NSAID to a COX-2 inhibitor, such as rofecoxib (by 8.8 events per 100 patient years in VIGOR) are much greater than in those without prior ulceration (by 2 events per 100 patient years),54 with similar results for celecoxib in CLASS.95 The substantial risk reduction associated with a switch to a COX-2 inhibitor in the ulcer prone, with a low NNT, makes their use practical and economically attractive.
“The substantial risk reduction associated with a switch to a COX-2 inhibitor in the ulcer prone, with a low NNT, makes their use practical and economically attractive”
However, many would regard as unacceptable the high residual risk after switching to a COX-2 inhibitor (which in VIGOR was 10 events per 100 patient years).96 This residual risk seems likely, but not certain, to reflect true residual risk rather than any remaining gastrotoxicity of COX-2 inhibitors. Co-prescription of a PPI would seem an appropriate strategy in patients with a past ulcer history as PPIs can influence not only NSAID associated risk but also that attributable to the residual influence of previous ulceration. In endoscopy studies, omeprazole reduced ulcer recurrence by 78% in those without84 and 64% in those with ulcers97 initially, compared with 54% for perforation, ulcer, and bleeds with rofecoxib 50 mg versus ibuprofen 2400 mg (all patients). Results with lansoprazole and pantoprazole have been similar to those seen with omeprazole,78–80 and omeprazole itself has been shown to reduce ulcer rebleeding fourfold.81 Again, direct comparison of the occurrence rates of symptomatic/complicated ulcer in patients treated with low dose non-selective NSAIDs under PPI protection with those receiving COX-2 inhibitors (alone and combined with a PPI) would be of considerable clinical interest and is a strategy some might prefer on current limited evidence.
Older patients
Risks of ulcer and ulcer complications increase with age in individuals who do not use NSAIDs. These raised risks may reflect the cohort pattern of ulcer morbidity and mortality observed since the second half of the 19th century,97 and now in its decline, and itself may be partly explained by an increased prevalence of H pylori currently seen in older people. Other factors, including an accumulated history of subclinical ulcers and reduced mucosal integrity due to vascular disease, may also be important. NSAIDs consistently magnify background risk by some fourfold, regardless of age, so that the proportion of disease attributable to NSAIDs remains constant. It was therefore predictable that substitution of a COX-2 selective inhibitor for standard NSAID would result in marked reductions in the numbers affected, but also leave substantial residual risk. Given the uncertainty about the mechanism(s) that leads to increased risk in the elderly, arguments can be made for using COX-2 inhibitors, or for using non-selective NSAIDs with PPIs. Sound comparative evidence of overall gastrointestinal and non-gastrointestinal safety in this group is needed.
Patients requiring high doses of NSAIDs
Increasing NSAID dosage within the accepted ranges approximately triples the risk of ulcer complications (table 2).41,88 By contrast, full dose coxibs possess equivalent anti- inflammatory and analgesic power, and available evidence suggests that they should not increase gastrointestinal risk although risks associated with fluid retention may rise.11
Patients requiring corticosteroids
Correct management is difficult to identify unequivocally as evidence conflicts about the effect of corticosteroids on the risk of ulcer disease.87,99–102 If, as some studies suggest, the effect of corticosteroids is to act only as an NSAID specific risk magnifier,100,102 particular benefit would be anticipated with COX-2 inhibitors, and there was some evidence for this in the VIGOR study.96,103 Other studies however suggest that corticosteroids also increase risk in non-NSAID users,87,99 making vigorous prophylactic strategies possibly more appropriate for those on high dose corticosteroids with multiple current diseases.
H pylori positive patients
The interaction between H pylori and NSAIDs is controversial, with some reports suggesting that infection raises the chances of NSAID associated ulcer,104 others the reverse.105,106 Regardless of such controversy, when patients use COX-2 inhibitors, H pylori would be expected to remain a source of continuing ulcer risk, requiring eradication in appropriate patients. Although there are no trials, this approach is supported by data from the VIGOR study where the residual risk of ulcers in patients taking rofecoxib was approximately doubled in H pylori infected compared with non-infected individuals.96,103
Patients with cardiovascular disease
These patients currently pose the greatest intellectual and therapeutic challenge in this area. Claimed associations of ulcer bleeding with cardiovascular disease, or its treatment, are common. In assessing such claims, allowance has to be made for concurrent aspirin and anticoagulant use and for concurrent disease. A weakly significant association of ulcer bleeding with prior cardiovascular disease was found in the MUCOSA study.77 In a case control study an odds ratio of 5.9 (2.3–13.1) for the influence of cardiovascular disease appeared independent of aspirin and anticoagulant use.87 Thus arthritic patients with heart disease may have multiple risks—of ulcer complications both from cardiovascular disease and from aspirin use, along with an enhanced rate of hypertension from use of NSAIDs or COX-2 inhibitors (although a suggested association with calcium channel blockade107 has not been confirmed,87 and nitrates claimed to protect or to have little effect).108
“Claimed associations of ulcer bleeding with cardiovascular disease, or its treatment, are common”
Management of such patients should start from assessment of the net value of aspirin. This is clear cut for secondary prophylaxis and for some high risk groups29,30 but more widespread use may cause more harm than good.29 Secondly, for those who need aspirin, doses above 100 mg daily are not evidence based and result in increased risk of ulcer bleeding29 (a meta-analysis suggesting no dose dependence109 seems flawed because it compared high dose studies in the 1970s with low dose studies in the 1990s when inclusion criteria differed and reporting of complications was likely to have been more rigorous). If a patient needs aspirin, recent data on the interaction with ibuprofen40 suggests it is unsafe to assume that aspirin would protect against coronary thrombosis in the presence of this drug. Such a patient needing anti-inflammatory medication might benefit from a selective COX-2 inhibitor, not for its gastroprotective effects but for its permissive cardiovascular benefits in allowing aspirin to continue to be effective. Because this is as yet speculative, direct data on clinical end points are needed.
As aspirin itself increases the risk of ulcer bleeding, whether or not patients use COX-2 inhibitors, those that are at high risk from such aspirin use (for example, following an ulcer bleed) would logically be managed under the protection of a PPI. Abandoning aspirin following an ulcer bleed in a patient with significant coronary instability would run the risk of precipitating vascular events during hypotension following haemorrhage, or as a consequence of the bleeding induced hypercoagulable state. The chances of cardiovascular death are overall many times greater than those of ulcer death. Equally, switching to a non- aspirin antiplatelet agent seems both optimistic in discounting a role for haemostasis in ulcer bleeding and contentious, given that associations with gastrointestinal bleeding have been reported.110,111
On the other hand, until recently, there was little direct evidence for a protective effect of PPIs on the risk of ulcer bleeding in patients taking cardioprotective doses of aspirin. Abundant endoscopic data showed that PPIs protected against aspirin induced injury up to one month, but longer term patient studies with doses of aspirin ⩽325 mg were lacking. Recently published data have clarified the matter by showing a substantial reduction in ulcer rebleeding in users of aspirin 100 mg treated with lansoprazole 30 mg compared with placebo, following H pylori eradication in all.82
Patients with coagulation defects or on anticoagulants
Use of anticoagulants results in an increase in ulcer bleeding in the absence of NSAID use, a similar proportionate magnification with NSAIDs, and a consequential high absolute excess risk in these circumstances.87,112 Consequently, prescribers tend to avoid NSAIDs in patients taking anticoagulants or with coagulation deficiencies, despite a need for pain relief in, for example, patients with haemophiliac arthropathy. Although there are no data, lack of any antiplatelet effect is sufficient justification to use COX-2 inhibitors in these patients although monitoring prothrombin time is desirable.113
CONCLUSIONS
It is likely that an overall reduction in NSAID toxicity will only be achieved by applying different strategies to different patients. There are sufficient data to make a best guess at what these should be. However, as we have indicated throughout this article, there is an outstanding research agenda involving direct comparison of strategies by subgroup. These could be amalgamated into a comparison of subgroup optimised management with cruder strategies that would need research council support, given that such an approach is unlikely to be forthcoming from the pharmaceutical industry.
Acknowledgments
We thank Miss Laura Garratt for her assistance with the production of this manuscript.