Article Text

Abstract
Background: Northern France was characterised by a high incidence of Crohn’s disease (CD) and a low incidence of ulcerative colitis (UC) according to the first inquiry undertaken in the late 1980s.
Aims: To assess the trends in the incidence of inflammatory bowel disease (IBD) over a 12 year period (1988–1999) in the same area of Northern France.
Patients: Patients living in Northern France (Nord, Pas-de-Calais, Somme, and Seine Maritime—total of 5 790 526 inhabitants) between 1988 and 1999 were included in the study. Case ascertainment was established according to methodology previously described.
Methods: Trends in incidence were studied using a Poisson regression model in four three year periods (1988–90, 1991–93, 1994–96, and 1997–99) adjusted for age at diagnosis and sex. Incidence rates were standardised for age with the European standard population.
Results: During 1988–99, 7066 cases of IBD were recorded (56.8% CD, 37.7% UC, and 5.5% indeterminate colitis). Mean annual incidence rate of CD increased from 5.2/100 000 inhabitants in 1988–90 to 6.4 in 1997–99 (adjusted p for trend <0.001). In contrast, the incidence of UC decreased from 4.2 to 3.5 (adjusted p for trend <0.001). The ileocolonic subtype of CD increased by 25% even though median age at diagnosis and frequency of digestive investigations were not different.
Conclusions: Contrary to what has been reported in other countries in Northern Europe, the incidence of CD increased by 23% in 12 years in Northern France while that of UC decreased by 17% during the same period. This indicates that some factors which influence IBD frequency (in both directions) are still at work in this area of Europe, and that further studies aimed at identifying these should be performed. The rising incidence of CD could enhance the burden of this disease on the public health system in France.
- ulcerative colitis
- Crohn’s disease
- inflammatory bowel disease
- epidemiology
- IBD, inflammatory bowel disease
- CD, Crohn’s disease
- UC, ulcerative colitis
- UP, ulcerative proctitis
- IC, indeterminate colitis
Statistics from Altmetric.com
- IBD, inflammatory bowel disease
- CD, Crohn’s disease
- UC, ulcerative colitis
- UP, ulcerative proctitis
- IC, indeterminate colitis
Inflammatory bowel diseases (IBD) including Crohn’s disease (CD) and ulcerative colitis (UC) are chronic diseases of environmental, genetic, and/or immunological causes.1 Geographic or temporal variations in the incidence of IBD can help to identify causal factors. Since the 1950s, data from North America and Europe have reported a trend for an increasing incidence of CD and stabilisation (at a higher level) of the incidence of UC.2 In Europe, the EC-IBD population based study reported a higher incidence of UC (11.8/105 compared with 8.7/105) and CD (7.0/105 and 3.9/105, respectively) in Northern compared with Southern Europe.3 Northern France (close to Northern Europe) was characterised by a high incidence of CD (4.9/105) and a low incidence of UC (3.2/105).4 Data on the evolution of the incidence rates of CD in Europe are scarce and report variable trends: some show an increase in Southern Europe5,6 while others show stabilisation or even a decrease in Northern Europe.7,8 To determine how Northern France compares with these results, we report the results of a 12 year registry.
SUBJECTS AND METHODS
Population
Northern France had 5 790 526 inhabitants in the 1999 National Population census. The study area was divided into four sectors: (a) Nord, with 2 554 449 inhabitants and a population density of 445/km2; (b) Pas-de-Calais, with 1 441 422 inhabitants and a population density of 216/km2; (c) Somme, with 555 479 inhabitants and a population density of 90/km2; and (d) Seine-Maritime, with 1 239 176 inhabitants and a population density of 197/km2. There are both rural and urban populations in these areas (ratio urban/rural = 8.9 in Nord, 4.5 in Pas-de-Calais, 1.4 in Somme, and 3.0 in Seine-Maritime). This region is a well defined geographical entity bordering Belgium and the North sea (fig 1). The population was stable—that is, the percentages of the population moving per year for each area were 0.8 for Nord and Pas-de-Calais, 1.1 for Somme, and 0.9 for Seine-Maritime (French National Statistical Institute).

Geographical area of case registration. N, Nord; PDC, Pas-de-Calais; So, Somme; SM, Seine-Maritime.
Case identification and diagnostic criteria
The methodology of the EPIMAD has been described in detail previously.4 Data concerning all patients diagnosed between 1 January 1988 and 31 December 1999 were collected by interviewing the gastroenterologists of the area (n = 238) practising in the private or public sector. Before the study began, all gastroenterologists were informed about the methods and aims of this work, both by letter and by meetings. Only patients who had been resident in the defined study area at the time of diagnosis of their disease were included.
Each gastroenterologist reported on any patient consulting for the first time with clinical symptoms compatible with IBD and was contacted by phone at least three times a year by an interviewer practitioner. This interviewer went to the gastroenterologist’s consulting room and collected the data from the charts in a standardised questionnaire for each new case. The main data collected were: age, sex, year of diagnosis, interval between onset of symptoms and diagnosis, and clinical, radiological, endoscopic, and histological findings at the time of diagnosis.
A final diagnosis of CD, UC, or ulcerative proctitis (UP) was made by two expert gastroenterologists and recorded as definite, probable, or possible following criteria previously published.4 Patients with a case history of chronic colitis compatible with both a diagnosis of CD or UC were defined as indeterminate colitis (IC).
Patients with a case history of colitis of less than six weeks were classified as acute colitis. A systematic follow up at 18 months of patients with acute colitis was undertaken after the first visit in order to reconsider the actual final diagnosis.
Quality assurance procedures
The steering committee of the study included five academic gastroenterologists, two academic epidemiologists, one academic paediatric gastroenterologist, one private gastroenterologist, and five interviewer practitioners. This committee established written instructions for the interviewer practitioners for completing the questionnaire correctly. It also set up a framework to help the expert gastroenterologists in their final diagnosis. The committee met every three months. The aim of these meetings were, by means of test cases, to verify that the protocol was accurately followed by all interviewer practitioners and to minimise interexpert variations.
To validate the completeness of case collection by gastroenterologists, we undertook a one year validation study in the Somme region in 1989. All general practitioners (n = 498) and radiologists, histopathologists, surgical, and paediatric specialists (n = 36) received a questionnaire for notifying incident cases of IBD. If they did not reply, they were contacted by telephone. All specialists and 450 of 498 general practitioners (91%) replied. In total, 85 cases were notified by these practitioners. In contrast, the recording system by the gastroenterologists notified only 82 cases. The three “missing” cases were declared by two pathologists and one general practitioner (one possible UC, one possible CD, and one probable UP). These patients had actually consulted a gastroenterologist who had forgotten to declare their cases to the interviewer practitioner. Thus the completeness of our case collection was 96.5%.
Analysis
Incidence rates were calculated for the combined group of definite and probable cases (CD, UC, and IC) diagnosed between 1988 and 1999. Possible cases of IBD and acute colitis were not included in the calculation of incidence rates. Cases of UC and UP were pooled together. For each region, population data by age and sex were obtained for each year from linear interpolation of the 1982, 1990, and 1999 National Population Census. Mean annual incidence rates were calculated based on the number of patients diagnosed and the number of inhabitants for both sexes. Age standardisation was performed using the European standard population weights 15, 14, 14, 14, 14, 13, 9, 5, and 2 for each 10 year age group.9 Confidence intervals for the age adjusted rates were calculated according to the method proposed by Breslow and Day.9 Trends in incidence from 1988 to 1999 were studied in four three year periods (1988–90, 1991–93, 1994–96, and 1997–99). Trends in incidence by age at diagnosis (0–19; 20–39; 40–59; 60 years or older age groups), sex, and time period (three year intervals) were evaluated using a Poisson regression model adjusted for geographic area (Nord, Pas-de-Calais, Somme, and Seine-Maritime).
Location of disease was reported only for patients who underwent a complete bowel investigation (small and large bowel visualised for CD and large bowel visualised up to the caecum for UC). For CD, three locations were considered: ileocolonic, pure colonic, and pure small bowel. For UC, three locations were considered: UP, defined as involvement to the rectosigmoid junction; pancolitis, defined as involvement up to the caecum; and left sided colitis, including involvement above the rectosigmoid junction with no involvement of the caecum.
For descriptions of age at diagnosis (years) and time intervals between symptoms and diagnosis (months), median and interquartile ranges (25th and 75th percentiles) are given. Comparisons were performed using the Wilcoxon rank sum test or the Kruskall-Wallis test.
Data analysis was performed with SAS software.10
RESULTS
Patients
During 1988–99, a total of 7066 IBD cases were recorded. There were 4013 patients diagnosed as having CD (56.8%), 2665 with UC (37.7%) including 904 UP (34% of UC), and 388 with IC (5.5%). Median age at diagnosis was 27 years (range 21–38) for CD and 35 years (range 26–47) for UC (p<0.001). Median interval from onset of symptoms to diagnosis was three months (range 1–12) for CD and two months (range 1–6) for UC (p<0.001). A familial history of IBD was present in 7.3% of patients (9.7% of CD and 4.2% of UC patients).
Crohn’s disease
Incidence
Mean annual crude incidence rates of CD and UC were 6.0 and 4.0/105 inhabitants, respectively. Standardised incidence rates were 5.8/105 (95% confidence interval (CI) 5.6–6.0) and 4.0/105 (95% CI 3.8–4.1), respectively. The standardised mean annual incidence rate of IC was 0.58 (95% CI 0.52–0.64), which did not change during the study period.
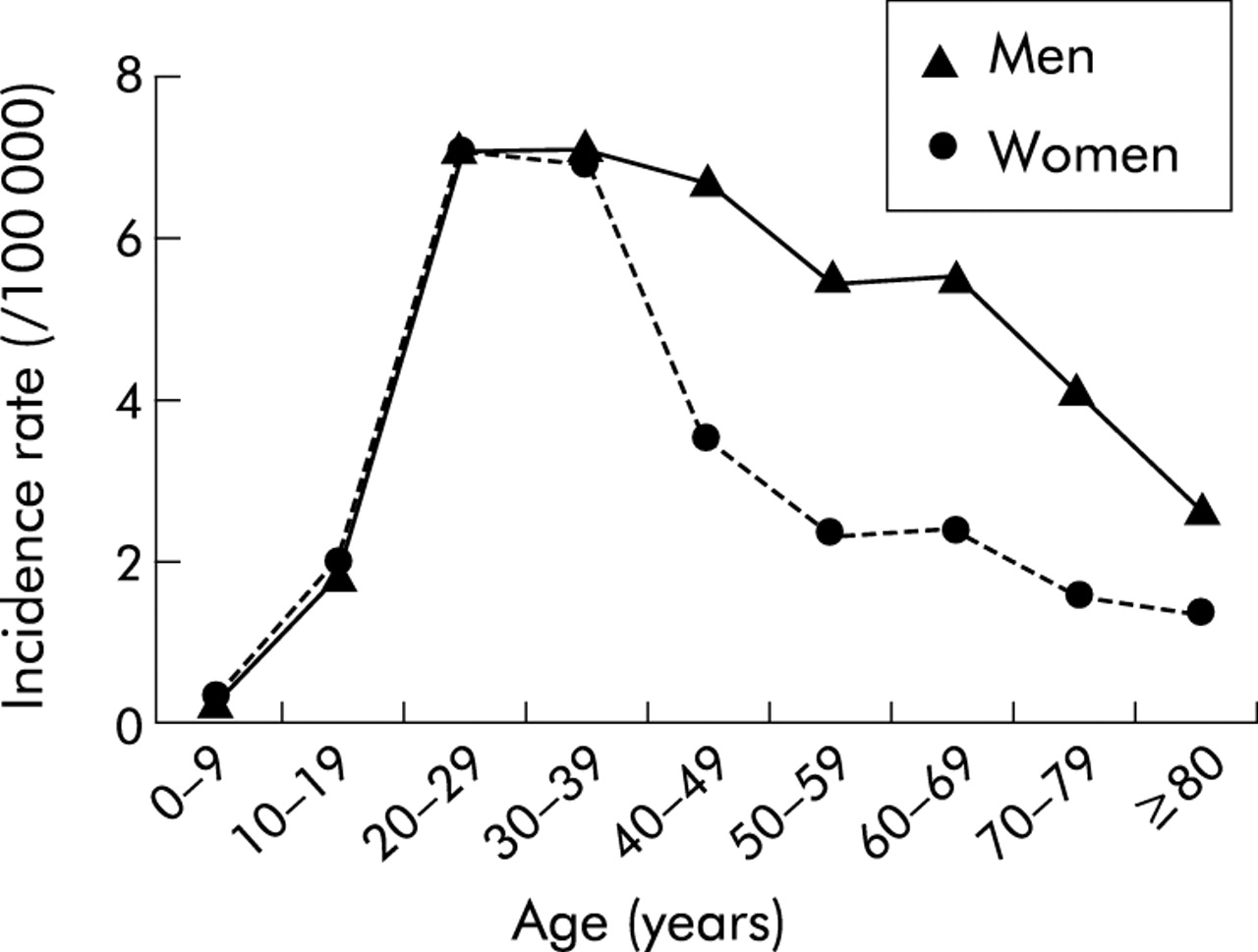
The incidence of CD was more elevated in women than in men: 6.4 versus 5.3/105 (p<0.001). The highest incidence rate was found in the age group 20–29 years for men and women (fig 2). The mean annual standardised incidence rate (/105) increased from 5.2 in 1988–90 to 6.4 in 1997 (fig 3). The rise in incidence was particularly high in the 20–29 year age group and was similar for men and women and in the four regions (table 1). The female/male ratio was 1.2 and did not change over the time period.
Trends in incidence and manifestations of Crohn’s disease (Northern France 1988–99)

Incidence rate of Crohn’s disease by sex and age (Northern France 1988–99).

Trends in standardised incidence (95% confidence interval) of Crohn’s disease (CD) and ulcerative colitis (UC) (Northern France 1988–99).
Disease manifestations (table 1)
At diagnosis, colonoscopy was initially performed in 92% of CD patients, a small bowel follow through x ray in 81%, while a complete (both large and small bowel) investigation was performed in 76.7% of patients; this proportion did not change over the 12 years. An ileocolonic location was observed in 60.7% of patients, pure colonic in 18.7%, and pure small bowel in 20.6%. Perineal involvement was present in 18.3% of patients, and upper digestive lesions compatible with CD location in 36.0% (either at x ray or endoscopy). During the study, the frequency of ileocolonic involvement increased whereas that of colonic involvement decreased. Median age of patients with an ileocolonic location was 24 (19–33) years at diagnosis, for pure small bowel median age was 27 (21–37) years, and for pure large bowel it was 30 (22–42) years (p<0.001).
Ulcerative colitis
Incidence
UC was more common in men (4.6 v 3.4/105; p<0.001). The highest incidence rate was found in the age group 20–29 years, 30–39 years for women, and plateaued from 20–29 to 50–59 years, decreasing more gradually for men (fig 4). The mean annual standardised incidence rate (/105) of UC decreased from 4.2 in 1988–90 to 3.5 in 1997–99 (fig 3). The reduction was observed mainly in the 40 year and older age groups. The decrease was similar in men and women; the female/male ratio remained stable at 0.7 during the whole period (table 2).
Trends in incidence and manifestations of ulcerative colitis (Northern France 1988–99)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence rate of ulcerative colitis by sex and age (Northern France 1988–99).
Disease manifestations (table 2)
The interval between onset of symptoms and diagnosis shortened: from 79.3% of patients diagnosed within nine months of symptom onset in 1988–90 to 85.2% in 1997–99 (p = 0.05). A colonoscopy was performed in 99.1% of patients, and was total (up to the caecum) in 70.7%, not differing among the four age groups. The proportion of patients who underwent a colonoscopy did not change during the 12 years but the proportion of total colonoscopy sharply increased from 66.5% in 1988–90 to 78.9% in 1997–99 (p<0.001). Among patients having had a total colonoscopy, 30% had proctitis, 17.5% pancolitis, and 52.5% left sided colitis, and this was similar in men and women. At diagnosis, pancolitis was more frequent in the age group 0–19 years, affecting 28% of patients compared with 18%, 13%, and 18% in the 20–39, 40–59, and 60 year or older age groups. In contrast, left sided colitis was more frequent in older patients: 63% in the 60 year or older age group compared with 53%, 51%, and 50% in the 0–19, 20–39, and 40–59 year age groups. Although the frequency of pancolitis tended to rise, no significant modification of location at diagnosis was detected.
CD/UC ratio
A rise in the CD/UC ratio was observed (fig 3) for both sexes, each age group, and each region. This ratio, initially less than 1 only in men and in Seine-Maritime, reached 1 or more for all groups in the last period 1997–99 (from 0.9 in 1988–90 to 1.4 in 1997–99 for men; from 0.8 to 1.2 for Seine-Maritime). The gap became even higher in groups where CD was already more frequent than UC (women, regions other than Seine-Maritime).
DISCUSSION
Incidence
Increasing trend for CD
An important finding of this study was that between 1988 and 1999, the incidence rate of CD in Northern France increased by 23% while the incidence rate of UC decreased by 17%. The incidence rate of CD in our study has reached levels comparable with those of Northern countries (table 3), being close to rates for Wales,11 Norway,12 and Minnesota13. Numerous studies have reported an increasing trend over the past 50 years.5,6,11,14–17 The increasing trend was often related to increasing age at diagnosis (global increase5,15,16 or a higher proportion of older patients7,17). This was not the case in our study in which we found a higher proportion of cases in younger patients (20–39 years), as found by Bjornsson and Johannsson.14 After a period of increasing incidence, stabilisation was described in the early 1980s.7,8,13 In our study, the rising incidence has not reached a plateau, suggesting that unknown triggering environmental factors are still at work in Northern France.
Worldwide incidence rates of Crohn’s disease (CD) and ulcerative colitis (UC)
Decreasing trend for UC
We confirm a low incidence of UC in our area, contrasting with higher rates in other countries of Northern Europe (table 3). An increasing trend in the incidence of UC was observed until the 1980s, followed by stabilisation in Europe.5,19–21 Two studies reported a decreasing trend in the incidence of UC, in Minnesota from 15 to 8/105 (1973–93)22 and in Copenhagen from 15.4 to 12.3 and from 14.1 to 12.6 in women and men, respectively (1981–92),23 while two others reported an increasing trend.14,24 Ascertainment bias of UC cases in our study could not explain this decrease as: (a) follow up of acute colitis and possible cases of UC, which could eventually be reclassified as UC, did not change during the study period and; (b) the proportion of proctitis location (30%), considered a marker of case ascertainment, remained stable.
Tobacco consumption and appendectomy are well known factors decreasing the occurrence of UC while tobacco consumption increases the occurrence of CD. However, the decreasing trend for UC, preponderant in older subjects and in men, was not in accordance with the evolution of smokers in France25: more women and less men have been smoking since the early 1990s. Furthermore, tobacco consumption decreased in younger people (18–25 years), from 54% in 1992 to 47% in 1999 (p<0.01) whereas the incidence of CD increased. The variations observed in the cohort between men and women could be linked to a difference in smoking cessation between men and women. In most areas, men tend to stop smoking more frequently than women.26 Future research should focus on these factors to determine their role in the occurrence of IBD.
Our study confirmed the higher incidence of CD than UC in both sexes and in each region of Northern France. Initially reported in France and Belgium4,27–29 in the early 1990s, a higher incidence of CD was also observed in Stockholm,30 Manitoba,31 Rochester,32 Cardiff,11 and Tubingen33 The inverse ratio could be explained by the stability in incidence of UC whereas CD had increased in most developed countries. Our incidence registration, which started later than in other countries, may have started after the crossing point between the incidence of CD and UC. This is more obvious when examining the evolution of the CD/UC ratio from 1988 to 1999 in the Seine Maritime region: UC, which was more frequent than CD, became similar or less frequent than CD.
Disease manifestations
The sex and age distributions of UC and CD were in accordance with previous publications.3,4
CD manifestations
Some studies reported a higher and increasing trend of pure colonic location at diagnosis7,11,14,34: from 47% to 51% of patients with a pure colonic location at diagnosis in Iceland (1970–79 to 1990–94)14 and from 15% to 32% in Sweden (1955–64 to 1980–89).7 In contrast, we observed a predominant and increasing trend of the ileocolonic location and a decreasing trend of pure colonic location. This evolution could not be explained by modification of small bowel investigations which remained stable. There are two possible explanations. Firstly, we studied location only in patients who had undergone a complete bowel investigation (both large and small bowel visualised) which was not always reported in other studies. Secondly, median age was increased in most studies describing a higher pure colonic location15,16 whereas in our study only the proportion of younger patients aged 20–39 years had increased, as occurred in Minnesota.13 Pure colonic location at diagnosis is less frequent in younger compared with older CD patients, and thus these modifications could be due in part to modification of the age distribution at diagnosis.
UC manifestations
In most reports proctitis location represents one third of UC patients and pancolitis is the less frequent location at diagnosis.14,21,29,35 Recent studies reported an increase in distal colitis locations, especially proctitis,20,36 whereas pancolitis remained stable.20 Tysk and Janerot assigned these modifications to better awareness of gastroenterologists to symptomatic patients. In our study we did not find an increase in distal locations (neither left sided colitis nor proctitis). The slight non-significant increasing trend of pancolitis location may be related to the increase in complete colonoscopy investigations (from 66.5% to 78.9% of patients).
In conclusion, we showed that in an area characterised by a high incidence of CD and a low incidence of UC, the trend remains towards a continuing increase in the incidence for CD and decrease for UC. This suggests that factors which influence the frequency of IBD (in an opposite direction for CD and UC) remain active, at least in this part of Europe, and offer an exciting opportunity to study them with a reasonable chance of success.
Acknowledgments
The authors thank the interviewer practitioners who collected the data: B Lemaire, N Guillon, M Inglard, I Rousseau, N Wauquier, P Fosse, M Lecomte, D Panis, L Yzet, C Dias, and S Richon. We also thank Dr Cyrus Tamboli for a thorough reviewing of this manuscript. EPIMAD is organised under an agreement between the Institut National de la Santé et de la Recherche Médicale (INSERM), the Direction Générale de la Santé (DGS), and the Institut National de Veille Sanitaire (InVS), and is also supported by the François Aupetit Association, the Ferring Laboratories, IRMAD (ASTRA Company), the Observatoire Régional de la Santé du Nord-Pas-de-Calais, the Caisse Régionale d’Assurance Maladie de Nord Picardie, and the CHRU de Lille.
We thank all the gastroenterologists and specialists who participated in this study: André JM, Antonietti M, Armand A, Aroichane I, Aubet JP, Auxenfants E, Barbry B, Bardoux N, Baron P, Baudet A, Bazin B, Bebahani A, Becqwort JP, Benet V, Benguigui C, Ben Soussan E, Bental A, Berkelmans I, Bernet J, Bernou-Dron C, Bertot P, Biron N, Bleuet M, Blondel F, Bohon F, Boniface E, Bonnière P, Bonvarlet E, Bonvarlet P, Boruchowicz A, Bostvironnois R, Bouche B, Boudaillez C, Bourgeaux C, Bourguet A, Bourienne A, Bray G, Brazier F, Breban P, Brung-Lefebvre V, Burgiere P, Butel J, Canva JY, Canva-Delcambre V, Capron JP, Cardot F, Carpentier P, Cartier E, Cassar JF, Castex JF, Catteau L, Caujolle B, Cayron G, Chantre M, Charles J, Charneau T, Claerbout JF, Clergue PY, Cohen G, Collet R, Crinquette JF, Dadamessi I, Dapvril V, Davion T, Debas J, Dehont F, Delatre C, Delcenserie R, Delette O, Delgrange T, Delhoustal L, Delmotte JS, Deregnaucourt G, Descombes P, Desechalliers JP, Desmet P, Desseaux G, Desurmont P, Devienne A, Devred M, Devroux A, Dewailly A, Dubois R, Ducatillon P, Duclay J, Ducrocq B, Ducrot F, Ducrotte P, Dufilho J, Duhamel C, Dujardin D, Dupont F, Duranton Y, Elie-Legrend MC, Evrard JP, Filoche B, Finet L, Foissey D, Foutrein-Comes MC, Foutrein P, Frere T, Gallet P, Gamblin C, Geslin G, Gheyssens Y, Gilbert T, Godard P, Godchaux JM, Godchaux R, Goria O, Gottrand F, Gower P, Grandmaison B, Guedon C, Guillard JF, Guillem L, Guillemot F, Hanon D, Heckestweiller P, Hedde JP, Hellal H, Heyman B, Heraud M, Herve S, Hochain P, Houcke P, Ivanovic A, Janicki E, Jeu J, Jonas C, Kerleveo A, Kiriakos A, Kiriakos J, Klein O, Kornhauser R, Koutsomanis D, Laberenne JE, Laffineur G, Lannoy P, Lapchin J, Laprand M, Laude D, Lecieux P, Leclerc N, Le Couteulx C, Ledent J, Lefebvre J, Le Grix A, Lelong P, Lenaerts C, Leplat A, Leroi H, Leroy MY, Lesage JP, Lesage X, Lesage J, Lescanne-Darchis I, Lescut J, Lescut D, Leurent B, Lhermie M, Lion A, Lisambert B, Loire F, Luciani M, Lucidarme D, Lugand J, Macaigne O, Maetz D, Maillard D, Mancheron H, Marti R, Martin F, Martin G, Marzloff E, Mathieu-Chandelier C, Mauillon J, Maunoury V, Maupas JL, Mesnard B, Metayer P, Meurisse B, Meurisse F, Mirmaran X, Modaine T, Morel L, Moulin E, Mouterde O, Mudry J, N’GuyenTack R, Notteghem B, Ostyn A, Ouvry D, Panien-Claudot N, Paoletti C, Papazian A, Parent B, Paris JC, Patrier P, Paupart L, Pauwels B, Pauwels M, Petit R, Piat M, Piotte S, Plane C, Plouvier B, Pollet E, Pommelet P, Pouchain G, Prades P, Prevost A, Prevost JC, Queuniet AM, Quinton JF, Rabache A, Rabelle P, Razemon V, Reix N, Richez C, Robinson P, Rodriguez J, Roger J, Roux JM, Rudelli A, Savoye G, Schlosseberg P, Segrestin M, Seryer A, Sevenet F, Silvie J, Simon V, Spyckerelle C, Talbodec N, Thelu JL, Thorel JM, Toisin J, Tonnel J, Touchais JY, Tranvouez JL, Triplet C, Turck D, Vaillant E, Valmage C, Vanco D, Vanderbecq E, Vandermolen P, Vandevenne P, Vandewalle C, Vanhoove JP, Verbiese G, Vermelle P, Verne C, Vincendet M, Viot J, Voiment YM, Waeghemaecker L, Wallez JY, Wantiez M, Weber J, Willocquet JL, Wolschies E, Zellweger A, Ziade C.