Article Text

Abstract
Objective Colonoscopy is the accepted gold standard for detecting colorectal adenomas, but the miss rate, especially for small and flat lesions, remains unacceptably high. The aim of this study was to determine whether enhanced mucosal contrast using pancolonic chromoendoscopy (PCC) allows higher rates of adenoma detection.
Methods In a prospective, randomised two-centre trial, PCC (with 0.4% indigo carmine spraying during continuous extubation) was compared with standard colonoscopy (control group) in consecutive patients attending for routine colonoscopy. The histopathology of the lesions detected was confirmed by evaluating the endoscopic resection or biopsy specimens.
Results A total of 1008 patients were included (496 in the PCC group, 512 in the control group). The patients' demographic characteristics and indications for colonoscopy were similar in the two groups. The proportion of patients with at least one adenoma was significantly higher in the PCC group (46.2%) than in the control group (36.3%; p=0.002). Chromoendoscopy increased the overall detection rate for adenomas (0.95 vs 0.66 per patient), flat adenomas (0.56 vs 0.28 per patient) and serrated lesions (1.19 vs 0.49 per patient) (p<0.001). There was a non-significant trend towards increased detection of advanced adenomas (103 vs 81; p=0.067). Mean extubation times were slightly but significantly longer in the PCC group in comparison with the control group (11.6±3.36 min vs 10.1±2.03 min; p<0.001).
Conclusions Pancolonic chromoendoscopy markedly enhances adenoma detection rates in an average-risk population and is practicable enough for routine application.
- Colonoscopy
- chromoendoscopy
- adenoma
- detection rate
- adenocarcinoma
- colorectal adenomas
- colorectal cancer screening
Statistics from Altmetric.com
- Colonoscopy
- chromoendoscopy
- adenoma
- detection rate
- adenocarcinoma
- colorectal adenomas
- colorectal cancer screening
Significance of this study
What is already known about this subject?
At colonoscopy, important neoplasias may be missed, especially if they are flat or if they are located on the proximal side of haustral folds and flexures.
Chromoendoscopy with indigo carmine spraying is used to improve the yield of colonoscopy for neoplasias. The dye increases mucosal contrast and the tip of the catheter can be actively used to straighten colonic folds for inspection of blind areas.
The role of chromoendoscopy in patients admitted for routine colonoscopy is uncertain.
What are the new findings?
Pancolonic chromoendoscopy with indigocarmine is an easy to apply supplemental tool with only a modest increase in the procedural time.
It increased overall adenoma detection compared with standard colonoscopy. This increase was significant for flat and small lesions but was modest for advanced neoplasias.
How might it impact on clinical practice in the foreseeable future?
The findings of this study support the use of indigo carmine dye spraying during colonoscopy, especially for patients who are at high risk for neoplastic lesions.
Introduction
Colonoscopy is regarded as the gold standard procedure in screening programmes for colorectal neoplasias. Detecting adenomas at colonoscopy is of the utmost importance, since endoscopic resection of these neoplastic lesions has been shown to prevent colorectal cancer effectively.1 Unfortunately, a substantial proportion of adenomas are missed during standard colonoscopy examinations. According to several reports, 10–25% of lesions remain undiagnosed at colonoscopy, even when conducted by experienced practitioners.2–5 Potential explanations for failure at colonoscopy include poor bowel preparation and inadequately short withdrawal times.6 An important technical factor that determines whether lesions are detected is the level of mucosal contrast provided by the imaging method. Low contrast may contribute to the miss rate for small and flat lesions, which only produce subtle changes in the mucosal topography such as loss of the vascular net pattern, focal pallor and marginal irregularity.7
Strategies capable of enhancing mucosal contrast might therefore improve the adenoma detection rate and optimise the potential of colonoscopy to prevent colorectal cancer. In this context, chromoendoscopy with indigo carmine dye spraying has been proposed as a method of enhancing the mucosal topography. Fine surface details become visible as this inexpensive and non-absorbed dye accumulates in the innominate grooves and crypt openings in the colonic mucosa. Most reports have described the use of indigo carmine locally to highlight areas of mucosa that already appear suspicious8–10 or to facilitate in vivo differentiation of polyp types.11 Applying the dye more generally in the form of pancolonic chromoendoscopy (PCC) may be advantageous if it helps detect previously unvisualised pathology. PCC has been reported to improve the detection of flat dysplasias in patients with ulcerative colitis12 and flat adenomas in screening and high-risk populations.3 13 However, there have only been a few prospective randomised studies comparing dye spraying with standard colonoscopy in average- and moderate-risk groups of patients.14–19 These studies have reached varying conclusions. Although some suggest that chromoendoscopy may increase the detection rates of small and flat adenomas in diagnostic colonoscopies,14–17 19 this may not necessarily translate into an improvement in the overall adenoma yield.15 18 In addition, staining of the entire colon during colonoscopy requires extra training and may be labour-intensive and time-consuming, and thus unsuitable for routine use.
The present study investigates the value of PCC in the detection of colonic polyps and compares its performance with that of standard colonoscopy. This represents the largest prospective and randomised trial on the value of PCC with a multicentre approach. In contrast to the multistep segmental spraying techniques described in previous studies,13 16 17 a low-volume spraying technique was used in the present study, with gentle dye spraying during continuous withdrawal of the scope. This simplified technique allows shorter extubation times and ensures complete mucosal staining without excessive dye accumulation.
Patients and methods
Patients
During an 18 month study period, consecutive patients presenting to the two study centres were recruited, as permitted by the availability of the study colonoscopists and the study instruments. Patients were eligible for inclusion in the study if they were aged 45 or over and presented for primary screening or diagnostic colonoscopy for a variety of reasons (table 1). Patients with known inflammatory bowel disease, overt bleeding, polyposis syndromes or previous surgical resection of the colon, and patients receiving anticoagulant medication were excluded. All of the patients provided informed consent before participating in the study. The study protocol was approved by the clinical research ethics committee of the General Ethics Council of the state of Hesse, Germany (no. 84/2007) and conformed with good clinical practice (study number DRKS00000174).
Patients' demographic characteristics and indications for the procedure
Endoscopic procedure
The examinations were carried out by five experienced endoscopists in two medical centres using high-resolution standard endoscopes (Fujinon EG-450, EG-490 and EG-590; Fujinon, Saitama, Japan). The endoscopists were required to have carried out at least 50 examinations with PCC in order to become acquainted with the low-volume indigo carmine spraying procedure. All endoscopists were aware of the hypothesis of the study.
At colonoscopy, the colonoscope was inserted as far as the caecum, and the quality of bowel preparation was rated by the endoscopist in accordance with the validated criteria described by Ell et al.20 Patients with poor (semi-solid stool) or very poor (solid stool) preparation were withdrawn from the study. Introduction as far as the caecum was performed as quickly as possible, with no special care being taken to look for lesions.
After intubation of the caecum, patients with adequate bowel preparation were randomly assigned to either the PCC group or the control group by nurses using standard randomisation lists. The lists contained consecutive patient numbers, with each number linked to allocation to one of the two study arms (PCC or control group). The randomisation lists were not accessible to the endoscopists.
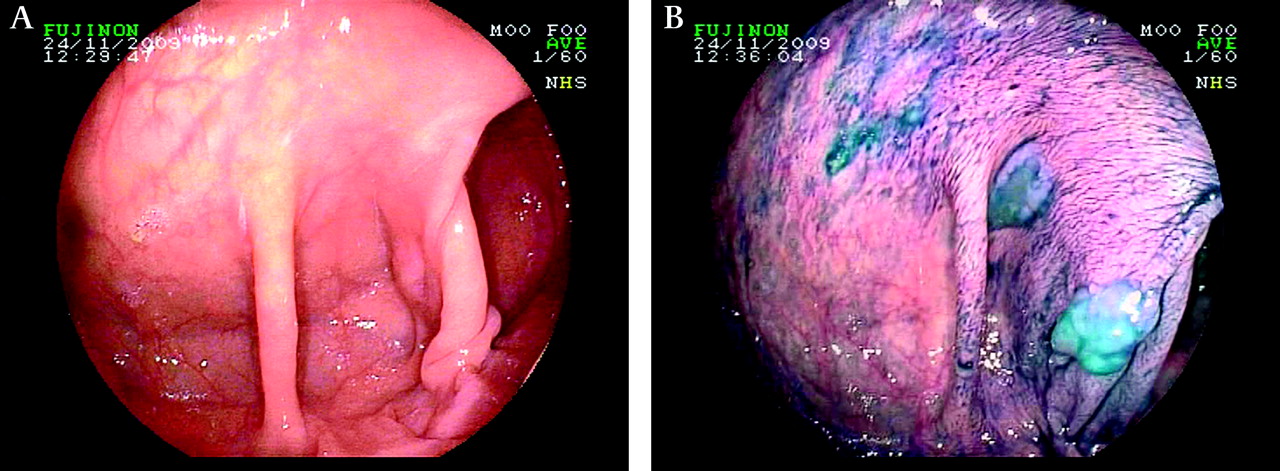
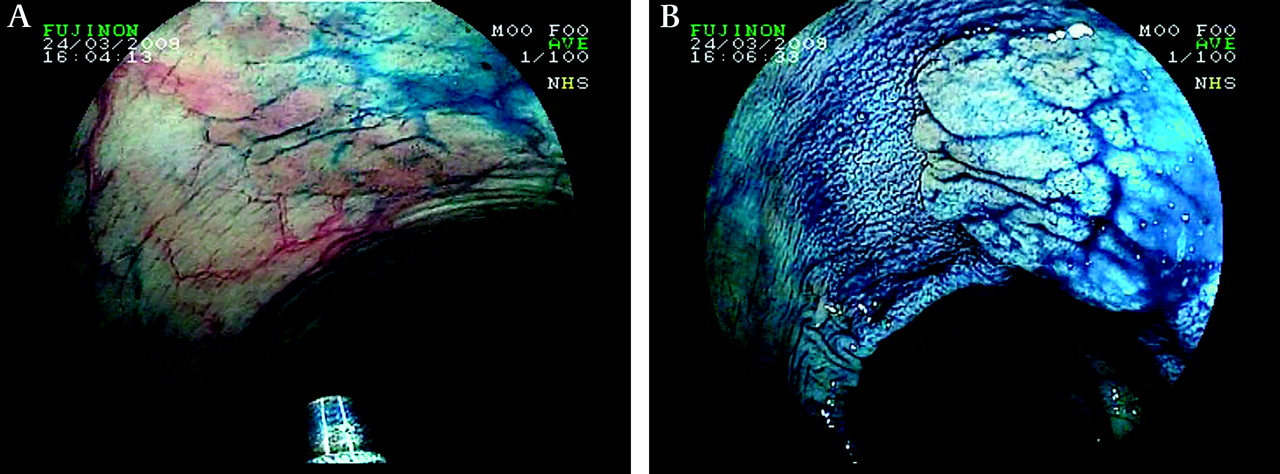
Assessment of the colon to search for lesions was performed systematically only during withdrawal of the instrument, with a minimum diagnostic extubation time that was set at 8 min. Special care was taken to wash and clean the entire colon during instrument introduction and withdrawal, in order to provide optimal conditions. Patients randomly assigned to the control group received conventional colonoscopy during the withdrawal of the instrument. In the PCC group, withdrawal was performed using the indigo carmine low-volume spraying technique. A dye-spraying catheter (PW-5L-1, Olympus) was inserted through the colonoscope's working channel and was extended 5–10 mm from the instrument channel throughout extubation, allowing straightening of mucosal folds for inspection of the proximal side and aspiration of excess fluid. Because the spraying catheter does not completely block the working channel, the suction function for fluids was not hampered to a relevant extent. During continuous extubation, indigo carmine (0.4%) was gently applied by the nurse in order to achieve diffuse coverage of the entire mucosal surface, using only a small volume of dye in order to avoid excess dye accumulation. This continuous one-step low-volume technique is much simpler than the previously described multiple-step staining techniques involving segmental staining followed by re-examination after excess dye has been aspirated. Figure 1 shows the appearance in the ascending colon before and after indigo carmine spraying. Figure 2 illustrates the increase in plasticity and contrast enhancement achieved when imaging a flat adenoma during indigo carmine spraying.

(A) The ascending colon visualised with standard colonoscopy. (B) After indigo carmine dye spraying. Indigo carmine highlights two lesions corresponding to sessile serrated adenomas.

A flat adenoma visualised during withdrawal with indigo carmine spraying. (A) There are some mucosal irregularities, which are highlighted by minimal amounts of indigo carmine. (B) After targeted indigo carmine spraying, the plasticity and demarcation of the lesion are enhanced.
In both groups, the lesion morphology, size (estimated by the endoscopist) and anatomic location were documented during withdrawal. Each lesion was characterised according to the Paris Classification criteria. We have used the term ‘flat’ to encompass non-polypoid neoplasms (type IIa–c). Non-polypoid lesions (type II) project <2.5 mm, whereas polypoid lesions project ≥2.5 mm into the lumen. Lesion size was estimated visually with the use of an open biopsy forceps when needed.
The histopathological findings were confirmed by evaluation of the endoscopic resection or biopsy specimens. Advanced adenomas were defined as adenomas ≥1 cm or adenomas with high-grade intraepithelial neoplasia. Hyperplastic polyps and sessile serrated adenomas were grouped as serrated lesions. An important feature of the study design was that rectal lesions were excluded from assessment, as high numbers of small, serrated rectal lesions are common. Complete sampling of these lesions for histological assessment might not have been feasible and might have obscured the study results.
Statistical analysis
The primary outcome parameter in the study was the total number of patients with at least one adenoma. A sample size calculation was performed, assuming from historical data a prevalence rate of 30% of patients with adenomas in the control group. To demonstrate an increase in this rate to 40% with PCC, 476 subjects were required in each arm of the study (90% power; significance level 0.05). Secondary outcome measures included the total number of adenomas, the accuracy of histological prediction of lesions and withdrawal times for each technique.
Wilcoxon rank sum tests were performed to compare the two groups for differences in the number of adenomas per subject. Fisher exact tests and the Mann–Whitney U test were performed as indicated.
Results
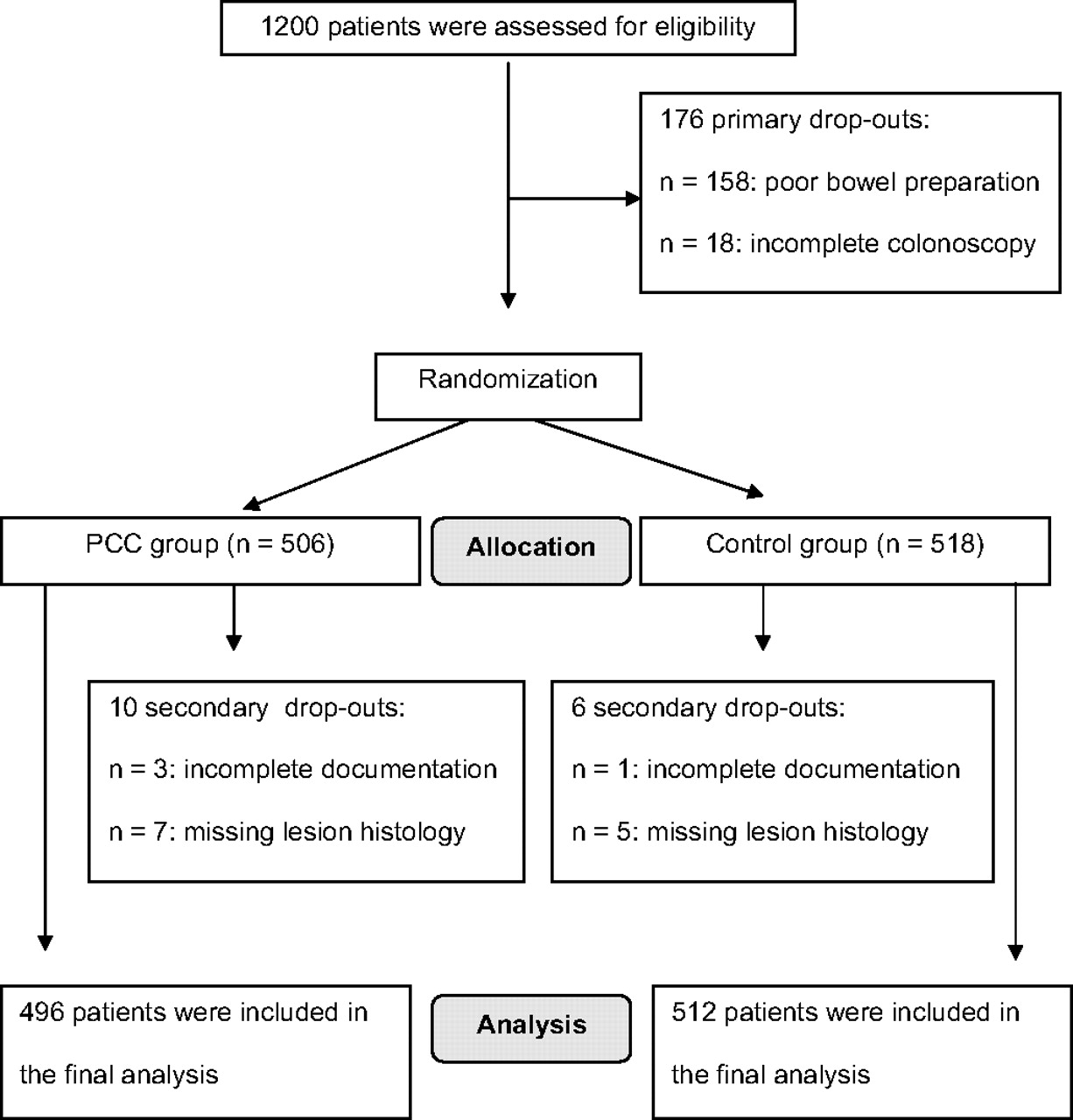
A total of 1200 patients were assessed for eligibility between September 2008 and February 2010. Patients with poor or very poor preparation (n=158) or incomplete colonoscopy (n=18) were excluded, leaving 1024 patients for random assignment to the PCC group or control group (figure 3). Secondary drop-outs occurred in four cases due to incomplete documentation and in nine cases because histological findings for the lesions were missing, leaving a total of 496 patients in the PCC group and 512 patients in the control group for final analysis (figure 3). Altogether, there were 468 female patients (46.4%), and the mean age of the patient population was 63.6 years (range 45–94 years). The patients' demographic characteristics and the indications for colonoscopy are shown in table 1. There were no statistically significant differences between the PCC group and the control group with regard to sex, age or the indications for colonoscopy. In comparison with standard colonoscopy, indigo carmine spraying increased the extubation time in procedures without endoscopic interventions slightly, but statistically significantly (11.6±3.36 min vs 10.1±2.03 min, respectively; p<0.001). The total procedure times (including colonoscopies with endoscopic interventions) were 16.64±8.77 min (range 8–82) in the PCC group and 12.76±5.45 min (range 8–55) in the control group (p<0.001). The mean volume of indigo carmine used in the PCC group was 58.0±16.77 ml per patient.

{kind=link}
{kind=link}
{kind=link}
Flow diagram showing progress through the study, in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement. PCC, pancolonic chromoendoscopy.
In all, the colonoscopy examinations in the 1008 patients detected 1681 lesions, including 808 adenomas and 24 carcinomas. Table 2 shows the prevalence rates of lesions in the PCC group and control group in a per-lesion analysis.
Pathological features of the evaluated lesions
There was a significant increase in the overall detection rate for adenomas in the PCC group (470 adenomas; mean of 0.95 per patient) in comparison with the control group (338 adenomas; mean of 0.66 per patient; p<0.001). The detection rate for the subgroup of flat adenomas in the dye-spraying group was nearly double that in the control group (p<0.001). In the subgroup of advanced adenomas (adenomas ≥1 cm and/or high-grade intraepithelial neoplasia), there was a tendency towards a higher detection rate in the PCC group, but this trend did not reach statistical significance (p=0.067). High-grade intraepithelial neoplasia was histologically confirmed in 23 adenomas (16 in the PCC group and seven in the control group). Two of these adenomas were ≤1 cm. There were no differences with regard to the carcinoma detection rate (12 in each group).
In addition to the improved detection of neoplastic lesions, there was also a significant increase in the detection of serrated lesions in the dye-spraying group (p<0.01). Fifteen of the serrated lesions were histologically confirmed as serrated adenomas (5 in the PCC group and 10 in the control group).
When the polyp findings were analysed according to distribution (right hemicolon, transverse colon, left hemicolon), no differences were observed between the PCC group and the control group with regard to the proportion of adenomas detected (table 3).
Locations of detected adenomas
Table 4 shows the prevalence of patients with lesions. In the PCC group and control group, the prevalence rates for patients with one or more lesions of any histology were 70.4% vs 58.2% (p<0.001); for patients with one or more adenomas, the rates were 46.2% vs 36.3% (p=0.002). This difference continued to be significant in the subgroup of patients with adenomas ≥5 mm in size (p=0.012), but did not reach statistical significance in the subgroup of patients with advanced neoplasias (p=0.076). In addition to differences in the detection rates for neoplastic lesions in the PCC group, there was also a significant increase in the number of patients with one or more serrated lesions (46.2% vs 29.5%; p<0.001).
Identification of patients with adenomas and serrated lesions
Table 5 shows that the extent of the effect of PCC on adenoma detection was operator dependent. Four endoscopists had increased detection rates for patients with at least one adenoma. The increase reached statistical significance in two operators. However, the total number of performed colonoscopies and indications for the procedures differed significantly between endoscopists. Therefore, interindividual comparison of the performance is not possible.
Identification of patients with adenomas by individual endoscopists
Discussion
It is essential to detect adenomas during screening colonoscopy examinations, but a significant proportion of adenomas are missed even with current technology. Although most of the missed adenomas are small and possibly of minor importance, the efficacy of screening colonoscopy is based on the concept of leaving the patient with a clean colon by removing all of the adenomas found. A higher adenoma detection rate is therefore regarded as a sign of better quality colonoscopy.
The present study is the largest randomised, prospective multicentre trial to investigate the clinical feasibility of indigo carmine dye spraying for detecting neoplastic colonic lesions. The calculation of case numbers was set in such a way as to reveal even minor differences between the conventional and PCC techniques at adenoma detection levels already well known from previous studies, both in Wiesbaden11 and nationally in Germany.21 22 A total of 1008 patients with screening and diagnostic colonoscopies were randomly assigned to either the PCC group or the control group. The overall adenoma prevalence was 41.6%, a rate that compares well with the adenoma rates of 37.5% and 35.5% reported in recent large German screening trials.11 22 Application of indigo carmine during colonoscope withdrawal improved both the overall yield of adenomas and the number of patients in whom adenomas were found.
These data are consistent with three recent reports on PCC in high-risk populations,13 16 23 which found that PCC was superior in terms of the overall adenoma detection rate and also for identifying patients with at least one adenoma. The benefit conferred by PCC in average-risk populations is a matter of controversy, however. While one study found increased overall adenoma detection rates,14 other studies have reported that indigo carmine spraying detects significantly more diminutive and flat colorectal adenomas, but without a statistically significant overall increase in total adenoma detection rates or more frequent identification of patients with at least one adenoma.15 17–19 However, in three of these studies,15 17 18 the sample sizes were not calculated in such a way as to be capable of detecting differences <25%, and the patient numbers were limited to <300. A very recent well-conducted US multicentre trial19 compared high-definition PCC versus high-definition standard colonoscopy in 660 average-risk patients and found that the number of patients with at least one adenoma (55.5% vs 48.4%) and the number of adenomas per patient were higher in the PCC group, although these findings failed to reach statistical significance (p=0.07, respectively). Interestingly, a subanalysis revealed significant differences of the additional adenoma yield in the PCC group according to the study site, suggesting that chromoscopy has an inconsistent effect on adenoma yield and may benefit certain endoscopists, but not others. This notion is supported by our study that showed variable gains of adenoma detection by PCC in individual endoscopists.
However, in the US multicentre trial19 overall analysis showed that PCC detected significantly more diminutive and flat lesions per patient, with an additional yield that was comparable with the findings of our study. In accordance with this trial19 and previous other studies,14–18 the present study also shows that small tubular adenomas represent the majority of additional neoplastic lesions identified using dye spraying.
The value of detecting large numbers of small adenomas and removing them during colonoscopy may be questionable. However, these findings have implications for the recommended time intervals between screening colonoscopies in the individual patient. The present study shows that dye spraying improved the detection rate not only for small lesions but also for flat lesions. This is of critical importance, as several studies have indicated that flat adenomas are 10 times more likely than polypoid lesions to contain advanced neoplasia.24 The present study showed a strong trend towards higher detection rates with PCC for advanced neoplasias, although this did not reach statistical significance.
Although universal use of PCC may not be justified, these findings indicate that it may be appropriate for higher risk individuals—for example, those with a genetic predisposition to colorectal cancer or those previously found to have multiple or advanced adenomas, in whom the additional time required for the procedure is offset by increased confidence in achieving complete adenoma clearance. The present study also confirms the findings of previous investigators16–19 that more non-neoplastic polyps are detected with chromoendoscopy. Although this effect has not previously received much attention, several studies have in the meantime shown that serrated lesions may be precursors for colorectal cancer, via the serrated pathway.25 Reliable detection of serrated lesions during colonoscopy is therefore warranted.
Whether the use of an auxiliary technique is adopted in everyday practice depends on the additional clinical benefit it provides, as well as on its feasibility. In previous trials, PCC has mostly been carried out as a multiple-step procedure, including segmental application of dye and removal of excess dye, followed by inspection after repeated segmental insertion. This approach is time-consuming and has therefore not been implemented to any great extent in clinical practice. To overcome this problem, a low-volume one-step spraying technique was used in the present study which allows steady withdrawal of the device with gentle application of indigo carmine to ensure high-quality mucosal staining, while avoiding excess dye and time-consuming multiple-step segmental forward and backward movements of the scope. The present study shows that this technique is feasible, although some technical aptitude is required and specific training may be necessary for less experienced endoscopists. The dye-spraying catheter can be extended from the instrument channel throughout extubation, allowing aspiration of excess fluid around it. In addition, in the same way as the hood is used in hood-assisted colonoscopy, the tip of the catheter can be actively used to straighten colonic folds for inspection of blind areas.
Using the low-volume technique, the average volume of dye applied and the average withdrawal times are considerably lower than the dye volumes and time requirements for PCC reported in previous studies.13 16 18 19 This has important implications, as critics of chromoendoscopy have suggested that the prolonged inspection time required to perform chromoendoscopy, rather than the actual dye-spraying procedure itself, was the reason for the increased adenoma yield. Although the mean procedural time in the PCC group was significantly longer in comparison with standard colonoscopy in the present study, the time difference (11.6 min vs 10.1 min) was quite small and does not readily explain the increased yield of lesions. These results show that time constraints do not justify an avoidance of PCC in routine colonoscopy procedures. However, it is important to note that high-quality bowel preparation is a prerequisite for the use of dye-spraying techniques; 158 patients had to be excluded from the study due to inadequate bowel preparation.
Virtual chromoendoscopy with narrow-band imaging and Fujinon Intelligent Chromoendoscopy (FICE) have been regarded as a less laborious alternative to chromoendoscopy with dyes, and it was hoped that these methods might be able to replace PCC. However, it was found that narrow-band imaging21 26 and FICE11 did not result in improved detection of adenomas in comparison with standard colonoscopy for routine clinical indications.
Our study has certain limitations. First, patients admitted for regular colorectal cancer screening comprised ∼50% of the study population, but we also included patients admitted for surveillance colonoscopy or evaluation of symptoms. Therefore, it might be argued that a significant number of patients were not at average risk but at increased risk of colorectal neoplasias. If the study cohort were to have been exclusively composed of patients undergoing first-time screening colonoscopy, even a multicentre approach would have hardly reached the target sample size.19 Secondly, several endoscopists participated in the study and, despite our efforts to standardise the technique, persisting variations could potentially result in interindividual variations of adenoma detection rates. Futhermore, since it is impossible to blind endoscopists for the technique being used, there is an unavoidable bias. We acknowledge that these problems cannot be resolved for obvious reasons; therefore, we had to compromise and chose a study design that maximises generalisability of the results and optimises the relevance to clinical practice. Thirdly, in our study we did not use high-definition imaging. Some studies suggest that high-definition imaging itself might create a gain in adenoma detection and therefore the results of the present study might not be as applicable to colonoscopies performed with high-definition imaging.
In summary, our results show that PCC is superior to standard endoscopy for detecting lesions in the lower gastrointestinal tract. As this study included large numbers of patients and several endoscopists at two study centres, it can be regarded as providing a true picture of the benefits and disadvantages of this technique. Although there may be a learning curve involved in applying the dye (for both endoscopists and technical assistants), PCC is an easy to use supplementary tool. The findings of this study strengthen the argument for incorporating dye-spraying techniques into colonoscopy, especially for patients who are at high risk for neoplastic lesions.
References
Footnotes
Funding This study was supported by Fujinon, Saitama, Japan. Fujinon played no role in the design of the study, the analysis or the decision to publish.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the clinical research ethics committee of the General Ethics Council of the state of Hesse, Germany (no. 84/2007).
Provenance and peer review Not commissioned; externally peer reviewed.