Article Text

Abstract
Although endoscopic surveillance of patients with Barrett's oesophagus has been widely implemented, its effectiveness is debateable. The recently reported low annual oesophageal adenocarcinoma risk in population studies, the failure to identify most Barrett's patients at risk of disease progression, the poor adherence to surveillance and biopsy protocols, and the significant risk of misclassification of dysplasia all tend to undermine the effectiveness of current management, in particular, endoscopic surveillance programmes, to prevent or improve the outcomes of patients with oesophageal adenocarcinoma. The ongoing increase in incidence of Barrett's oesophagus and consequent growth of the surveillance population, together with the associated discomfort and costs of endoscopic surveillance, demand improved techniques for accurately determining individual risk of oesophageal adenocarcinoma. More accurate techniques are needed to run efficient surveillance programmes in the coming decades. In this review, we will discuss the current knowledge on the epidemiology of Barrett's oesophagus, and the challenging epidemiological dilemmas that need to be addressed when assessing the current screening and surveillance strategies.
- BARRETT'S OESOPHAGUS
- ADENOCARCINOMA
- SURVEILLANCE
- EPIDEMIOLOGY
Statistics from Altmetric.com
Introduction
In 1952, the incidence of oesophageal adenocarcinoma (OAC) was low enough that an OAC in Barrett's oesophagus (BO) merited a case report.1 OAC has now become the fifth leading cause of cancer-related death in men worldwide,2 with its incidence continuing to rise inexorably in the Western world.3 ,4
The dismal prognosis of OAC has focused interest on BO, its precursor lesion and a very common condition in western countries.5 ,6 BO is defined by replacement of oesophageal squamous epithelium by columnar epithelium with intestinal metaplasia as a consequence of gastro-oesophageal reflux disease (GORD).7 The cascade of GORD to BO and ultimately OAC offers attractive targets for screening and surveillance. These interventions aim to decrease mortality and improve survival related to OAC by early detection and treatment of either dysplastic BO tissue or early cancer. Endoscopic surveillance of BO has been recommended in various guidelines by different gastroenterological societies, and as such, has been widely implemented.8–13 However, as current evidence for either improved survival or cost effectiveness is equivocal at best, the efficacy of BO surveillance remains the subject of heated debate.14–16 This uncertainty also limits the basis for population BO screening.
In view of new epidemiological data that have become available since the development of surveillance guidelines, reconsideration of effective preventive strategies for BO patients seems justified. This review will provide an overview of our current knowledge on the epidemiology of BO and the challenging epidemiological dilemmas that need to be addressed when reassessing screening and surveillance strategies.
Epidemiology of BO
The epidemiology of BO is especially complicated because the majority of affected individuals are asymptomatic and remain undiagnosed.17 Those patients who come to medical attention are likely to represent a subpopulation that may very well differ from those who remain undiagnosed. Published epidemiological data can, therefore, only be an approximation of the true prevalence of BO.
Prevalence of BO in the general population
Most prevalence data have been derived from BO diagnoses made during oesophagogastroduodenoscopy (OGD) performed for dyspeptic symptoms, however, BO prevalence has been studied in unselected populations. An overall BO prevalence of 6.8% was found in a cohort of 961 patients undergoing colonoscopy that were offered an additional OGD. Short-segment BO (SSBO) was relatively common in persons aged 40 years or older (5.5%), irrespective of heartburn history.18 A similar colonoscopy-based study, limited to 300 subjects over age 65 years, found long segment BO (LSBO) in 4% and SSBO in 15%. There was no significant relation with reflux symptoms.19
So far, three population-based studies have addressed the prevalence of BO in the general population. Ronkainen et al20 performed upper endoscopy in a random sample of 1000 Swedish adults. BO was found in 1.6%, long segment in 0.5%, and short segment in 1.1%. Other population-based studies in Italy and China reported a BO prevalence of 1.3% and 1.9%, with LSBO in 0.2% and 0.5% of patients, respectively.21 ,22 These estimates indicate that approximately 0.5–1.5% of western populations would need to be offered regular endoscopic surveillance, according to current guidelines, if BO surveillance programmes are to be implemented.
Age, sex and ethnic distribution of BO
A British endoscopy study reported a 7% annual increase in prevalence of BO for both sexes. For men this increase started at age 20 years, however, in women it was delayed until age 40 years, resulting in a 20-year age shift and an overall 2:1 male predominance among BO cases.23 A large Dutch general practice registry confirmed the parallel age-specific increases in BO, with a similar 20-year age shift between men and women.24 The Northern Ireland BO registry which included over 9000 BO patients, also noted significantly fewer women than men diagnosed with BO in the age group of 16–40 years.25 This delayed development of BO is consistent with the 17-year delay in female OAC incidence, leading to an overall 3.5:1 male predominance, presumably as a result of women acquiring BO at an age when they die from other causes before developing OAC.26 ,27 This observation may relate to an endogenous protective effect related to sex-specific hormone production observed in premenopausal women, most likely oestrogen, which is known for its anti-inflammatory effects in certain tissues.11 ,12 The relationship between the prevalence of reflux oesophagitis and obesity in women suggests that this hormonal protection for women may disappear with their tendency to gain weight during perimenopause.28 The interaction between oestrogen and obesity in this respect needs further study.
Apart from these gender-related differences in BO epidemiology, there are also marked ethnic differences. A report from the USA based on Surveillance, Epidemiology and End Results (SEER) data noted far higher OAC rates in Caucasian white males than in black American males, with female rates far lower for both ethnic groups.3 ,29 In the UK, a higher BO prevalence in white Caucasians compared with Asians was reported.30 Data on the prevalence in Hispanics are contradictory, with some studies showing a similar prevalence to that in Caucasians,31 and other studies showing a lower prevalence.32 ,33
Increasing incidence of BO in the general population
The dramatic increase in the incidence of OAC over the past decades is thought to have been preceded by a similar steep increase in incidence of BO. Methodological problems have, however, confused the measurement of actual BO incidences.34–36 Some of the reported increases in newly made diagnoses are a result of more widespread use of endoscopy, increased awareness of BO among endoscopists, and higher oesophageal biopsy rates. However, a 93% increase in BO incidence between 1993 and 2005 was published from the Northern Ireland BO registry, where the potential confounding by number of endoscopies was avoided by counting the number of BO cases per 100 endoscopies.37 A similar Dutch study also reported an increase in BO incidence irrespective of numbers of performed OGDs. Importantly, the increased incidence was most pronounced among men under 60 years of age, suggesting a birth cohort effect, which might be related to increasing affluence after World War II.38 Similar cohort phenomena in OAC incidence have been demonstrated in the USA and Australia.39 ,40 Additionally, recent Dutch data reported a continuing rise in OAC and a decline in gastric cardia adenocarcinoma incidence.41
Explanations for the increasing BO incidence
One popular explanation for the increasing incidence of BO in western countries is the decreasing prevalence of gastric colonisation with Helicobacter pylori.42 A population-based study provided evidence that absence of H pylori colonisation was associated with BO.43 The suggested mechanisms for the inverse association include decreased acid production through gastric atrophy by H pylori infection44 ,45 and enhancement of gastric emptying, especially in younger persons.46 A parallel between the aforementioned birth cohort effect in BO incidence, and that of the prevalence of H pylori was also reported.47 ,48 The considerably lower OAC rates in countries with a high prevalence of H pylori also provide support for this hypothesis.49–51 However, H pylori infestation can also augment acid production. The OAC incidence of Swedish inpatients treated for duodenal ulcer during the 1960s considerably exceeded that of their contemporary gastric ulcer patients and the general Swedish population.52 Furthermore, the H pylori hypothesis fails to explain the male predominance and ethnic differences in BO and OAC incidence.
Therefore, an alternative hypothesis to explain the increasing prevalence of BO and OAC that is based on the prevalence of obesity has been proposed and is gaining popularity. This hypothesis proposes that the mounting prevalence of obesity, in particular visceral obesity, is responsible for the rising incidences of BO and OAC. Ryan et al53 found abundant evidence for obesity as the driving force behind the rising OAC rates. Obesity has been associated with a significant 1.5-fold to 2-fold increase in the risk of GORD symptoms and erosive oesophagitis, and a 2-fold to 2.5-fold increase in the risk of OAC.54 Possible mechanisms mediating this association include increased intragastric pressure and gastro-oesophageal pressure gradient,55 more frequent transient relaxations of the lower oesophageal sphincter,56 and increased oesophageal acid exposure.57
Two large case-control studies from the USA have reported that in particular, abdominal circumference (ie, waist-hip ratio), but not body mass index (BMI), was an independent risk factor of BO.58 ,59 A study among veterans based on CT scans showed that visceral adipose tissue but not BMI was independently associated with BO.60 The suggested mechanism could relate to the induction of a systemic pro-tumorigenic inflammatory state as a result of adipocytokines and pro-coagulant factors released by adipocytes in abdominal visceral adipose tissue. A high prevalence of metabolic syndrome in BO, especially in LSBO, with increased cytokine and fasting insulin levels, as compared to SSBO patients has been found.61 Additionally, visceral adipose tissue has also been strongly associated with increased serum levels of interleukin 6 (IL-6), tumour necrosis factor α (TNF-α), and C-reactive protein,62 as well as with leptin, which may stimulate cell proliferation and inhibit apoptosis in Barrett's-derived OAC cells.63
Visceral obesity may well help to further explain several epidemiological features of BO such as the sex and ethnic differences. A much stronger association between increasing BMI and GORD symptoms has been observed among whites than among black subjects and Asians,64 while white males have more visceral adipose tissue than black males.65 Another US study revealed that, at the same age and level of adiposity, black men and women had less visceral adipose tissue than white men and women, these differences were greater in men than in women.66 Visceral adipose tissue was also higher in white than in black postmenopausal women, although the latter had higher levels of subcutaneous fat.67 After menopause, visceral adipose tissue has been shown to increase in European–American, but not in African–American women.68 However, larger amounts of visceral adipose tissue were observed in Asian Americans than in white subjects.69 Genome-wide studies have identified a number of genetic loci involved in abdominal fat distribution, BMI and obesity.70 ,71 Further studies between the association of BO and these genetic loci to confirm these observations are now indicated.
Based on these correlations, it is plausible to assume that the steadily increasing prevalence of obesity,72 ,73 in particular, visceral obesity in many populations, will drive an increase in incidence of BO and OAC.
Cancer risk in patients with BO
Accurate estimates of the annual incidence of OAC and high-grade dysplasia (HGD) among patients with BO have been difficult to obtain, since studies have shown considerable variation in incidence rates. Published data predominantly have come from small cohort studies with relatively short follow-up, and mostly from referral centres, which likely have ascertainment biases that will show a higher cancer incidence than may be observed in larger population-based studies. Consequently, in light of these issues, it is not surprising that evidence of publication bias in surveillance studies favouring publication of small studies with high cancer incidence rates has been reported.74
Meta-analyses on cancer risk
Currently, seven systematic reviews have been published on the cancer risk in patients with BO.74–80 The pooled estimates for the annual OAC incidence among BO patients in these reviews varied between 0.3% and 0.6%, and between 0.9% and 1.0% for the combined incidence of HGD and OAC (table 1).
Overview of results from meta-analyses on oesophageal adenocarcinoma (OAC) risk in patients with Barrett's oesophagus (BO)
It should be noted that two reports failed to exclude early incident cancers (detection within 1 year after baseline diagnosis of BO),74 ,75 and three included cancers occurring in patients with HGD at baseline,74–76 thereby inflating risk of OAC.
In order to obtain more accurate estimates of the risk of OAC in BO patients, analysis of the data derived from high-quality studies (large study size, robust definition of BO) has been performed and has tended to show a lower cancer risk. This analysis revealed that the annual OAC incidence rates in BO cohorts with less than 2000 patient years widely ranged between 0 and 3.55%, and fell to 0.07–0.82% in cohorts with more than 2000 patient years of follow-up.78 The reliability of OAC incidence rates thus appears to depend on the size of the cohort and duration of follow-up. Besides the obvious higher chance of random deviation from the norm in small studies, there are a number of potential confounders that can strongly influence outcomes such as variations between cohorts in the male to female ratios, and age at BO ascertainment. A less obvious confounder is the proportion of the cohort lost to follow-up, with the resultant loss of follow-up years and OAC ascertainment, resulting in unreliable high OAC incidence rates.81
Population-based cohort studies
Recently, three population-based BO follow-up studies were published in which national cancer registries provided complete ascertainment of OAC incidence.6 ,82 ,83 Inclusion in the BO cohorts was based on national histopathology registries, while inclusion in the third study was based on an endoscopy registry83 (table 2). The design of these studies strongly reduced selection bias, which has been a particular limitation of previous cohort studies. The first and largest study consisted of 42 207 patients entered in a Dutch nationwide histopathology registry between 1991 and 2006 with a first diagnosis of BO with intestinal metaplasia and including either no concurrent dysplasia or, at most, low-grade dysplasia (LGD).6 Subsequent histological events were monitored until November 2007, or a diagnosis of OAC or HGD was made. The number of patient years for the remainder of the cohort was estimated from survival data from the general Dutch population. For BO patients undergoing endoscopic follow-up after baseline diagnosis, the annual OAC risk was 0.4%; however, when cancer risk was analysed for all BO patients, regardless of whether any follow-up was performed, the annual OAC risk dropped to 0.14%, with 0.19% in men and 0.08% in women.
Overview of results from nation-wide population-based incidence studies of oesophageal adenocarcinoma (OAC) in unselected patients with Barrett's oesophagus (BO)
The second study comprised 11 028 BO patients with intestinal metaplasia, with or without LGD, enrolled in the Danish Pathology Registry from 1992 through 2009.82 The civil registration number assigned to all Danes enabled data linkage of all medical registries and dates of emigration or death. After again eliminating all OAC cases occurring in the first year after index BO diagnosis, the authors found an annual OAC risk of 0.12% for the entire cohort, 0.15% for men and 0.05% for women.
The last study was the third update of the Northern Ireland BO registry cohort, comprising every adult diagnosed with BO in Northern Ireland between 1993 and 2005.83 The cohort includes 8522 BO patients, with or without intestinal metaplasia, followed until the end of 2008. The ascertainment of OAC was achieved by matching BO registry data with that of the Northern Ireland Cancer Registry. Besides including BO without intestinal metaplasia at index biopsy, the cohort differed from the two previous studies in that for some patients endoscopic data were available. An annual cancer risk of 0.13% for the entire cohort was found; 0.17% for men and 0.08% for women.
Some limitations of these studies warrant consideration. First, all three studies included the incidence of HGD as an outcome. As these were observational cohorts, and HGD is often asymptomatic, its ascertainment was far inferior to that of OAC and, consequently, its incidence was considerably underestimated. Second, sampling error and misclassification of dysplasia status may have affected the published results. Third, some patients with intestinal metaplasia of the cardia could have been misclassified as having BO, as endoscopic data were not provided. Nevertheless, the study size, population-basis, low ‘loss to follow-up’ rates, and high OAC ascertainment, though linkage of histology and cancer registries are major advantages of these studies. Additionally, the finding of remarkably similar absolute annual risks of 0.12–0.14% provides support that these studies are reporting accurate incidence data. Consequently, these studies have changed the views on BO-associated cancer risk and have set new standards for assessing OAC risk in BO.
Risk of mortality in patients with BO
Whether patients with BO have an increased mortality risk from causes either related or unrelated to OAC compared with the general population remains controversial.34 ,84–90 In studies reporting an excess mortality, this was primarily due to extra-oesophageal diseases such as pneumonia and, in particular, cardiovascular disease. It may well be that patients with pre-existing illness are more likely to have endoscopy and to have BO found than other members of the population.34 Additionally, increased mortality due to cardiovascular disease in BO may result from a shared association with obesity.
Screening for BO
The high prevalence of BO and its expected mounting incidence in the general population which heralds a further increase in OAC incidence, can be seen as arguments for targeted population screening for BO. Based on the epidemiological data described above, this approach would seem to be a plausible and necessary step to ultimately decrease OAC-related mortality. In order to achieve this goal, subjects at risk of BO would need to be identified, and either treated or monitored under surveillance, or both. However, for these approaches to have optimal efficacy, methods for the accurate assessment of an individual's cancer risk are needed.
Predictors of BO
BO is associated with increasing age, male gender, Caucasian race and visceral obesity,78 ,91 ,92 but symptomatic GORD remains its best known risk factor. While the severity of reflux symptoms fails to distinguish between reflux oesophagitis and BO,93 a long duration of reflux symptoms seems a better indicator of the presence of BO.94 ,95 In a community-based study, as compared with patients with GORD symptoms for less than 1 year, the relative risk of BO was respectively 3.0 and 6.4 for patients with reflux symptoms for 1–5 years and >10 years.96 Cigarette smoking is also a modest risk factor for BO.97 A recent analysis from five case-control studies reported adjusted ORs in the range of 1.5–2; the association strengthened with increased exposure to smoking until approximately 20 pack-years.98 Currently there is no evidence that alcohol intake increases the risk of BO.99 ,100 Two other studies have even suggested an inverse association between BO and wine consumption.101 ,102 Families with BO and OAC in multiple relatives over successive generations have been reported, suggesting a heritable component to BO and OAC.103–105 One study showed that familial BO was present in 30 (7.3%) of 411 probands with either LSBO, OAC or adenocarcinoma of the gastro-oesophageal junction, comprising 17 of 276 (6.2%) with BO, 11 of 116 (9.5%) with OAC, and 2 of 21 (9.5%) with adenocarcinoma of the gastro-oesophageal junction.106 Another study reported a 24% BO prevalence among first-degree members of BO index cases.107 A segregation analysis involving data on 881 singly ascertained pedigrees provided epidemiologic evidence in support of one or more rare autosomally inherited dominant susceptibility allele(s) in BO families, and, hence, motivated linkage analyses.108 Germline mutations in the MSR1, ASCC1, and CTHRC1 genes have been associated with the presence of BO and OAC,109 and a recent genome-wide association study (GWAS) study with 5986 BO cases and 12 825 controls in the replication stage found that genetic variants at two loci were associated with BO risk; one located at chromosome 6p21 within the major histocompatibility complex, and one on chromosome 16q24 for which the closest protein-coding gene was FOXF1, which is a transcription factor involved in oesophageal development and structure.110
Current guidelines for screening for BO
Currently, the American Gastroenterological Association (AGA) position statement on the management of BO recommends enrolling patients with multiple risk factors associated with OAC in screening programmes, although this was classified as a weak recommendation with moderate-quality evidence.9 The committee recommended against screening all patients with GORD. This statement corresponds to the American Society for Gastrointestinal Endoscopy (ASGE) guidelines,11 and to the updated guideline from the British Society of Gastroenterology (BSG) yet to be published.13 The French Society of Digestive Endoscopy (SFED) recommends against screening and does not make exceptions for any subgroups of patients.10 In the absence of randomised controlled trials of endoscopic screening, some cost effectiveness modelling studies have indicated that screening programmes may be cost effective,58 ,59 whereas other modelling studies have not.60
Dilemmas in screening for BO
One major dilemma that diminishes the usefulness of screening is that a significant proportion of BO patients lack reflux symptoms (box 1). In population-based studies of the prevalence of BO, over 45% of identified BO patients did not report symptoms of GORD.20 ,21 Additionally, even in patients with OAC, approximately 40% have no GORD history prior to diagnosis.111 Therefore, symptomatic GORD as a selection criterion for endoscopic screening is likely to exclude half the BO population. In fact, even if one accepts GORD as an entry criterion, a second dilemma is that the at-risk population is very large, as GORD symptoms are ubiquitous in the general population, with a prevalence of 15–20% in the Western world, and an incidence of approximately 5/1000 person-years.112 Implementation of a screening programme for BO based on GORD symptoms would, consequently, create a huge burden on the healthcare system, which is difficult to justify at this time given the paucity of data demonstrating a benefit of BO screening programmes on health outcomes. Another question that would need to be addressed in a BO screening programme is that of the age at which screening should be initiated. The yield of BO will be higher in older populations, however, in view of the long incubation period between the onset of BO and OAC, the majority of the elderly BO subjects are unlikely to develop OAC. Therefore, screening at age 40 would probably identify a higher proportion of BO patients who will ultimately develop OAC. However, these subjects would then be committed to decades of endoscopic surveillance with limited benefit per screening session given the low annual cancer risk.
Dilemmas with screening for Barrett's oesophagus (BO).
-
Significant proportion of BO patients and those with oesophageal adenocarcinoma lack reflux symptoms.
-
At-risk population for BO is too broadly characterised.
-
Endoscopy is invasive and expensive as a screening tool.
There are also substantial problems with the execution of various facets of endoscopic screening and surveillance programmes, such as false BO diagnosis through biopsies of the gastric cardia, resulting in unnecessary patient anxiety, unnecessary follow-up examinations, and, in the USA, increased expense and difficulty in obtaining life and other insurance.113 Additionally, OGD is relatively expensive,114 and carries a, albeit small, risk of complications, which becomes important when applied to large populations in a screening setting.115 ,116 Furthermore, the procedure is obviously burdensome to many patients,117 especially since patients diagnosed with BO may overestimate their cancer risk, contributing to a decreased quality of life.118 These limitations all favour restricting the use of endoscopic procedures for BO screening in large, population-based screening programmes (box 1).
Dilemmas with surveillance of Barrett's oesophagus (BO).
-
Overall risk of oesophageal adenocarcinoma in BO is low.
-
Only few patients will eventually die from oesophageal cancer.
-
Most cancers are detected outside surveillance programmes.
-
Biopsy sampling error due to patchy distribution of dysplasia.
-
Suboptimal adherence to rigorous biopsy protocol in daily practice.
-
Interobserver variability in diagnosing the presence and degree of dysplasia.
-
Natural history of dysplasia is unclear.
-
Surveillance is burdensome for patients.
-
Current practice is not cost effective.
Potential new minimally invasive screening modalities
Less invasive technology may solve the latter problem. In a study offering unsedated transnasal endoscopy and video capsule endoscopy as alternatives to sedated endoscopy, participation rates were 50%, 59% and 38%, respectively, which suggests that less invasive methods are preferable to patients.119 Ultrathin video endoscopes can easily be passed transorally or transnasally, providing an efficient, cost-effective alternative to standard sedated endoscopy.120 However, so far it has not been shown to result in a large increase in the number of primary care referrals for BO screening with unsedated ultrathin OGD.121 This could be the result of many factors, for example, the unwillingness of some patients to undergo unsedated procedures, and the lack of service provision for nasal endoscopy at many hospitals.
Oesophageal capsule endoscopy (OCE) offers a method of visualising the oesophagus without the discomfort and risks of OGD. Initial pilot studies have demonstrated a high diagnostic yield of BO, a high patient preference, and no safety problems.122 ,123 However, a meta-analysis of nine studies on the diagnostic accuracy of OCE for BO have reported a relatively low sensitivity (77%) and specificity (86%) for detecting BO.124 These suboptimal test performances, together with the current high cost of capsules and the inability to biopsy any detected BO are obvious disadvantages to OCE and preclude OCE as a screening test for BO in GORD patients.
Currently, the most promising alternative to endoscopic screening is the Cytosponge test, which is based on an ingestible oesophageal sampling device that allows cytology samples to be retrieved from the oesophagus. These samples can then be used in immunohistochemical assays of trefoil factor 3. It has an acceptable sensitivity and specificity for BO (73% and 94%, respectively), is easily applicable in primary care, and well tolerated by most patients.125 ,126 Furthermore, the binary scoring for trefoil factor 3 makes the test amenable to automation. A cost-effective model showed that screening based on the Cytosponge assay in 50-year-old men with symptoms of GORD followed by treatment of patients with dysplasia or intramucosal cancer is cost effective and would reduce mortality from OAC compared with no screening.127 Further validation of the Cytosponge test in different communities is required to assess its potential role in future BO screening. The most ideal screening test, however, would be based on the use of serum biomarkers, which are under development, and which may be available in the future.
Surveillance of patients with BO
Once BO is diagnosed, patients are offered endoscopic surveillance in order to detect high-risk BO (eg, BO with HGD) or early stage cancers suitable for curative treatment. Several factors need to be considered in individual patients before starting endoscopic surveillance, such as age, comorbidity, the patient's understanding of limitations of endoscopic surveillance, and the willingness of the patient to adhere to be compliant with the endoscopy-based surveillance programme.
Current guidelines for endoscopic surveillance
The majority of societal guidelines base the interval of surveillance endoscopy solely on the histological evaluation of biopsy samples, but usually not take other factors into account, such as, for example, age, gender and BO segment length (table 3). For BO patients without dysplasia, current guidelines by the American College of Gastroenterology (ACG) recommend surveillance endoscopy at 3-year intervals. For patients with LGD, annual surveillance endoscopy is recommended, and for those with HGD who receive no invasive therapy, intensive endoscopic surveillance exams every 3 months is recommended.8 The ASGE and the AGA medical position statements on the management of BO recommend intervals between 3 and 5 years for non-dysplastic BO (NDBO).9 ,11 The SFED does correlate the surveillance interval for patients with no dysplasia (ND) to the length of the BO segment; in those with SSBO surveillance endoscopy should be performed every 5 years, in those with a segment length of 3–6 cm, every 3 years, and in those with segments longer than 6 cm, every 2 years.10 Contrasting with the recommendations in the BSG guideline from 2006, the recently revised guideline also takes the length of the Barrett's segment into account, with recommended surveillance intervals every 2–3 years for non-dysplastic LSBO, and 3–5 years for those with SSBO.13
Guidelines for endoscopic surveillance of Barrett's oesophagus (BO) by gastroenterological societies
Dilemmas in endoscopic surveillance of Barrett's oesophagus
Although surveillance endoscopy is intuitively rational and endorsed by international gastroenterological societies, the data supporting many aspects of the recommended strategies are based on equivocal data. Consequently, most recommendations are classified as weak. More importantly, there are no prospective randomised controlled trials unequivocally demonstrating a beneficial effect of endoscopic surveillance on OAC mortality. Retrospective studies have shown that patients with OAC were more likely to have their cancer detected at an earlier stage when they had previously been in a surveillance programme compared to those patients not under surveillance.128 Furthermore, early recognition of HGD or cancer has been associated with an improved survival from OAC.129 However, results of non-randomised comparisons between surveillance and non-surveillance-detected cancers are hindered by a variety of factors including lead time and length bias, which falsely associate surveillance programmes with improved outcomes.130
One further problem with surveillance is that, although the vast majority of OAC cases arise in the setting of BO, only a small proportion of BO patients will eventually develop OAC,6 ,131 and even less will eventually die from OAC. In a Dutch cohort study, only 5.6% of total mortality among BO patients was related to OAC.84 Another observational study following a cohort of 409 BO patients for 10 years showed that only four (1.0%) of them died as a result of OAC.81 Moreover, an estimated 95% of patients with a new diagnosis of OAC do not have a previous diagnosis of BO,17 suggesting that for the general population, BO surveillance programmes will only have a modest effect on OAC mortality.
Several authors have used mathematical models to explore the cost effectiveness of BO surveillance.132–134 US researchers concluded that, for a cancer risk of 0.5% per annum, surveillance every 4 years was indicated, but if the annual risk was 0.4%, surveillance every 5 years was the only viable cost-effective strategy.134 Others reported that screening 50-year-old men with GORD to detect adenocarcinoma was probably cost effective when subsequent surveillance was limited to BO patients with dysplasia ($10440 per quality adjusted life year (QALY)). Screening was, however, far too expensive when surveillance was also performed in NDBO patients, even at 5-yearly intervals (additional $596000 per QALY).133 A British cost-efficacy study reported that at an annual cancer risk of 0.5%, BO surveillance conferred less benefit and more costs than no surveillance at all, irrespective of the surveillance interval used.132 The outcomes of all these modelling studies were strongly influenced by predefined parameters, the most critical of which was the annual incidence of OAC among BO cases, with most assuming 0.4–0.5%, which is the incidence still employed in current surveillance guidelines.8 Consequently, the observed 0.12–0.14% incidence from the population studies will only further provide support against the cost effectiveness of surveillance.
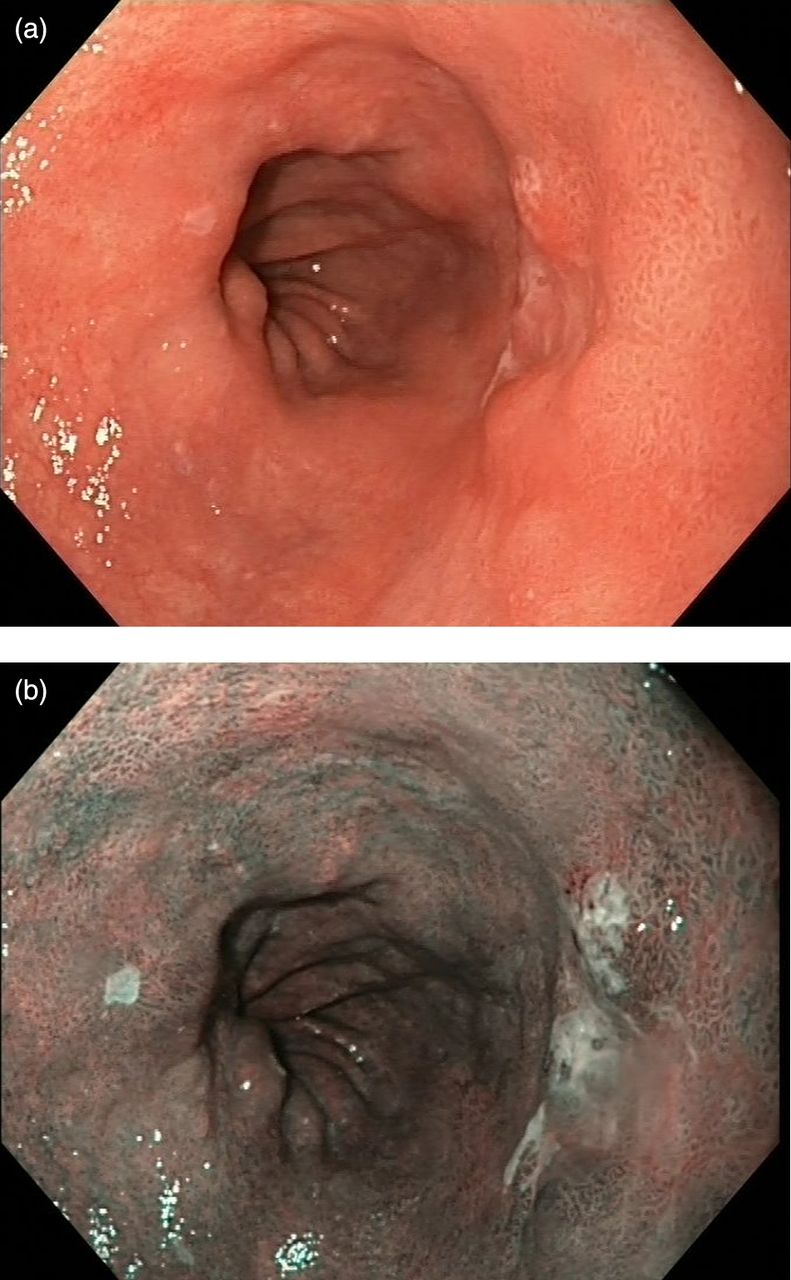
The execution of surveillance is also beset by technical problems. As dysplasia in Barrett's mucosa is often patchy, its diagnosis is subject to sampling error when biopsy-based sampling methods are used for its detection.135 In a retrospective study on 68 patients who underwent an oesophagectomy for HGD, 12 were diagnosed with adenocarcinoma in the resection specimen, of which eight were invasive cancers.136 Additionally, in a Danish study of newly diagnosed BO patients, more than two-thirds of all OACs were diagnosed during the first year of follow-up, indicating sampling error at the index biopsy.82 Extensive biopsy sampling, known as the Seattle biopsy protocol, has been recommended for decreasing sampling error, but is unable to eliminate the problem entirely, because even if it is properly performed, only 4–6% of the BO area can be sampled.137 Although the protocol has been associated with increased detection of dysplasia and invasive cancer,138 in daily practice, adherence to such a rigorous endoscopic surveillance protocol seems to be poor, and compliance is inversely associated with the length of the BO segment. In a Dutch retrospective study of endoscopy and pathology reports, adherence to the Seattle protocol was as low as 30%, in particular, among BO patients with segments of 10–15 cm in length.139 A similar US study reported an overall adherence of only 51%, with evidence that failure to protocol adherence was associated with decreased rates of dysplasia detection.140 These findings suggest that for those BO patients at highest risk of development of OAC, adherence appears to be the poorest. Advanced endoscopic techniques, such as chromoendoscopy, narrow-band imaging (NBI) and autofluorescence endoscopy, which are intended to enhance the detection of dysplastic areas for biopsy sampling, are promising,141 although they have not consistently been shown to increase neoplasia detection as compared with high-resolution white-light endoscopy (figure 1). A recent randomised controlled trial showed that use of NBI-targeted biopsies and the current standard of random four-quadrant biopsies diagnosed similar proportions of patients with BO, although NBI could achieve this with significantly fewer biopsies, suggesting improved efficiency and consequent cost reduction.142 However, as the study was limited to three tertiary BO referral centres, these results cannot be directly extended to non-tertiary centres. Given the poor adherence to the surveillance biopsy protocol, especially in those patients who are presumed to benefit the most of endoscopic surveillance, it should be considered to refer patients with longer segments of BO to tertiary centres for surveillance by an endoscopist experienced in specialised imaging modalities. A limitation, however, could be that given the ongoing increase in incidence of BO in the general population, this policy may create a huge burden on the healthcare system of tertiary hospitals. Therefore a cut-off length should be defined for identification of candidates for centralised surveillance. Additionally, it remains to be shown that such referral has no negative impact on patient adherence.

{kind=link}
Barrett's oesophagus containing early neoplasia; (A) lesion with white-light endoscopy, and (B) lesion with narrow-band imaging.
The substantial disagreement among pathologists in assessing the presence and grade of dysplasia has also raised concerns about the use of surveillance programmes that depend on accurate determinations of dysplasia in BO. The interobserver agreement in differentiating HGD from intramucosal cancer is only fair,143 while the interobserver agreement for the distinction between ND and LGD is poor.144 ,145 A retrospective study of the natural history of LGD in a community-based cohort of BO patients demonstrated that following review by two expert pathologists, 85% of patients with an initial diagnosis of LGD could be downstaged to ND or indefinite for dysplasia, while those with a consensus diagnosis of LGD had significantly higher rates of malignant progression than patients downstaged to ND.146 These findings indicate that a new diagnosis of LGD in particular should always undergo expert pathology review. Furthermore, the diagnosis of dysplasia varies between consecutive surveillance biopsies, which may be a result of sampling error, but may also indicate the inconsistent nature of this risk marker. It remains unclear whether dysplasia can regress over time. Misclassification of the presence and grade of dysplasia may lead to unnecessary follow-up endoscopies in case of overdiagnosis, or to possibly insufficient follow-up exams with inappropriate surveillance intervals in the case of underdiagnosis (box 2).
Risk stratification in patients with BO
The prolonged interval between BO onset and OAC incidence implies that the rational management of individual patients will require the ability to establish in any given BO patient an accurate assessment of risk for developing OAC and the approximate time to progression. To attain this goal, a prediction model, preferably based on demographic, environmental, endoscopic, histological and molecular markers is needed. A systematic review by Prasad et al147 described the current state of knowledge on predictors of progression in BO in detail. In the following paragraph, the current state of predictive factors for OAC is summarised.
Demographic and environmental risk factors
Male gender remains the most robust demographic factor predictive of OAC development. Population-based studies, as well as systematic reviews, have shown a much higher OAC incidence in men with BO than in women with BO.6 ,77 ,82 This finding is consistent with the strong male predominance in patients with OAC.29 ,148 The role of age on the progression in BO is, however, less clear. Several studies have shown that increasing age is an independent predictor of OAC development,149 with the highest incidence of OAC among BO patients older than 70 years of age,82 although other large cohorts could not confirm this.150 ,151 A retrospective study from the Cleveland Clinic BO registry did not show different rates of progression between BO patients younger and those older than 50 years.152 However, in a prospective observational cohort study from our centre, patients with a diagnosis of BO as long as 10 or more years prior to inclusion had a threefold increased risk to develop HGD or OAC, as compared with patients with a shorter known duration of BO diagnosis.153 Assuming the existence of an incubation period of three or four decades between BO onset and OAC development,154 and that the prevalence of BO increases with age, the smaller number of patients acquiring BO around their fourth decade are far more likely to survive long enough to develop OAC as compared with the great majority acquiring BO in their fifth and sixth decades. Consequently, the generally unknown age of BO onset would be far more relevant to prognosis than age itself, if this could be determined.
Malignant progression in BO has also been associated with an increased BMI at young age,155 and an increased waist to hip ratio, the latter being associated with an increased proliferation rate in BO as indicated by an increased percentage of S-phase cells.156 Additionally, increased waist to hip ratio, a surrogate marker of visceral adipose tissue distribution, but not BMI, was shown to be related to the risk of aneuploidy, 17p loss of heterozygosity (LOH) and 9p LOH,157 confirming visceral adipose tissue as a potential predictor of neoplastic progression. Smoking has, in some studies, been suggested as an additional risk factor for progression to OAC,155 ,158 ,159 while other investigators did not confirm this.151 ,153 ,160
Endoscopic risk factors
Multiple studies have found that length of the BO segment is a risk factor for development of OAC.158 ,160–167 A Dutch prospective cohort study of 713 BO patients found that each centimetre increase in BO length was associated with an 11% increase in the risk of developing HGD or OAC.151 Wani et al168 reported a significant higher risk of OAC in BO segments longer than 6 cm (0.09%/year) as compared to those shorter than 6 cm (0.65%/year; p=0.001). In a retrospective cohort study of 155 patients with SSBO and 93 with LSBO, a BO segment length >3 cm was found to be associated with dysplasia (OR 1.2; 95% CI 1.07 to 1.34).169 The presence of baseline dysplasia can be an important confounder of these associations between BO length and OAC incidence. In a large prospective cohort study, after adjustment for histology at study entry, segment length was not a significant predictor of progression.166 However, a recent meta-analysis on cancer risk in NDBO patients, reported an overall OAC risk of 0.33% (95% CI 0.28% to 0.38%), but only 0.19% for SSBO patients without dysplasia.80 It further remains to be clarified whether there is a specific length at which the risk of neoplastic progression increases significantly.
Visible nodularity has been associated with an increased risk of OAC, although the association seems to indicate the prevalence of concurrent HGD or OAC rather than a risk of future progression. An analysis of oesophagectomy specimens performed for HGD detected by endoscopic biopsies, demonstrated OAC in 7 of 9 (78%) patients with a visible lesion, whereas OAC was found in 7 of 22 (32%, p=0.02) patients without endoscopically visible lesion.170 In other studies, after endoscopic mucosal resection of lesions with HGD on endoscopic biopsy, a final diagnosis of cancer was made in more than a third of patients.171 ,172
The presence and size of a hiatal hernia have been associated with increased OAC risk,160 ,161 although these are probably merely surrogate markers for the severity of GORD. Oesophagitis has been reported to predict a 3.5 times higher risk of developing HGD/OAC in BO patient compared with those without.151 The underlying inflammation in oesophagitis is believed to increase the risk of mutations leading to HGD and OAC.173
Dysplasia and role of biomarkers
Currently, the grade of dysplasia is the most widely used and accepted marker for risk stratification in BO, but its value may be impaired by interobserver disagreement and sampling error. A correlation between the extent of dysplasia and the risk of progression to OAC has been sought. In patients with HGD, this was found to predict risk of progression to OAC (14% incidence of OAC within 3 years in patients with focal HGD vs 56% in diffuse HGD).174 Additionally, an association has also been reported between the extent of LGD (measured by the total number and fraction of dysplastic crypts) and the risk of progression to OAC.175
There have been a range of attempts to identify further biomarkers supporting or even replacing dysplasia as a risk stratifier. These have been extensively reviewed in two excellent recent reviews, including markers of genomic instability, tumour suppressor loci abnormalities, epigenetic changes, proliferation markers, cell cycle predictors and immunohistochemical markers.176 ,177 Of all potential biomarkers, immunohistochemistry for nuclear p53 currently holds out the best prospects for risk stratification in clinical practice, as it can be fairly easily applied, has demonstrated ability to improve the reproducibility of a diagnosis of dysplasia, and can also be a predictor of neoplastic progression.178 ,179 In a histopathological study on the impact of adding p53 immunohistochemistry to histology for classification of dysplasia, weighted kappa scores between pairs of pathologists showed substantial agreement, and improved after p53 immunohistochemistry.180 We previously observed an increased risk of development of HGD/OAC in the presence of aberrant p53 expression (HR 6.5, 95% CI 2.5 to 17.1)181 and recently in a prospective study confirmed that aberrant expression of p53 protein was a more powerful predictor of neoplastic progression than histological diagnosis of LGD. The positive predictive value for neoplastic progression increased from 15% with histological diagnosis of LGD to 33% with LGD and concurrent aberrant p53 expression.182 As a result of these and similar studies, the updated BSG guideline for the management of BO recommends to consider p53 immunohistochemistry as an adjunct to routine clinical diagnosis.13 Yet, the AGA medical position statement on the management of BO recommends against the use of any molecular markers to confirm a diagnosis of dysplasia or as a method of risk stratification.9
Management of patients with NDBO revisited
Endoscopic surveillance of BO patients without dysplasia remains the subject of debate, even more so since the publication of population-based studies that demonstrate a low OAC risk in BO patients. These new estimates have important implications for the clinical management of BO patients. First, the downgraded risk estimates of cancer in NDBO provide little support for the effectiveness of current surveillance at 3–5-year intervals. A meta-analysis of cost-effectiveness studies on endoscopic surveillance of NDBO, which was based on older and probably overestimated cancer risk estimates, already concluded that current surveillance strategies are unlikely to be cost effective.183 Although the value of dysplasia as a marker for risk stratification is hampered by interobserver disagreement and sampling error, all recent population-based cohort studies show that LGD at index biopsy was associated with a considerably heightened OAC risk, this, in spite of the fact that most cases will not have been diagnosed by specialist pathologists. This raises the question whether long-term surveillance can be omitted in some BO patients when absence of dysplasia has been confirmed repeatedly. Given the fact that a large proportion of OAC seems to occur within a year from BO diagnosis, it remains of paramount importance to perform an adequate endoscopic inspection at initial diagnosis, combined with obtaining a sufficient number of biopsy specimens to confidently assess for dysplasia. A subsequent follow-up endoscopy within 1 year after initial diagnosis, especially in LSBO, should be performed, in order to be more confident of a true absence of neoplastic or dysplastic histology. Although current epidemiological risk factors for cancer progression do not discriminate perfectly between low-risk and high-risk patients, they still strongly suggest that, in particular, white female SSBO patients without dysplasia at index diagnosis are the least likely to benefit from surveillance. In male SSBO patients without dysplasia a stopping rule for surveillance could be implemented after two endoscopies without dysplasia in non-targeted biopsy sampling. In female LSBO patients, it may be reasonable to extend further surveillance intervals from the currently proposed 3–5 years when absence of dysplasia has been confirmed, in particular, when no additional risk factors, such as smoking and obesity, are present. In case of a very long segment of BO, given the poor adherence to surveillance biopsy protocols in daily clinical practice, referral to a tertiary centre experienced in specialised imaging modalities may be considered.
A second important implication is that the new cancer risk estimates advocate against the increasing use of ablation therapy in NDBO patients. Endoscopic therapy for BO has been one of the most important developments for clinical practice, and is now the standard of care for patients with HGD or early mucosal cancer, preferred to surgery.184 For NDBO, however, given the low rate of cancer progression, the benefit of such intervention, even if leading to complete ablation, is unclear. A cost-usage analysis by Inadomi et al185 suggested that ablation therapy of NDBO could be the preferred management strategy if the procedure eliminates the need for long-term endoscopic surveillance. However, a cost-effectiveness study on the use of radio-frequency ablation (RFA) for BO by the same study group,186 based on more recent cancer risk estimates in BO, found that initial RFA was not cost effective for patients with NDBO within the range of plausible rates of progression of BO to OAC, while it might be cost effective for confirmed and stable LGD. For patients with HGD, initial RFA was more effective and less costly than endoscopic surveillance. Additionally, there remain many unanswered questions regarding the durability of the ablation procedure and the need for endoscopic surveillance after ablation. Sharma et al reported on three cases of subsquamous neoplasia including two developing OAC after RFA, highlighting the need for continued meticulous surveillance with biopsies of neosquamous epithelium, even after apparent successful eradication of intestinal metaplasia.187 If endoscopic ablation in low-risk BO is applied in practice, it should therefore only be performed within a trial.
Summary and future directions
BO is a common disorder in western countries, and appears to have a persistent increasing incidence in the general population, with obesity being the suspected most important driving factor for the increasing incidence. The increasing incidence heralds a further increase in OAC incidence in the coming decades, and emphasises the need for effective preventive strategies. At present, however, screening cannot be recommended, as the population at risk is too broadly defined, and current screening techniques are burdensome and costly. More research is anticipated on the development of less invasive and more cost-effective modalities for detection of BO, as well as on the development of non-endoscopic markers that can predict presence of BO.
With recent studies showing much lower cancer risk in BO than previously anticipated, and the growing emphasis on healthcare cost containment, the rationale for endoscopic surveillance is likely to come under greater scrutiny. The risk of OAC among patients with BO is so minor that in the absence of dysplasia, routine surveillance of such patients is of dubious value. BO patients with short segments of BO without dysplasia are the least likely to benefit, and surveillance could be omitted, especially when other clinical risk factors are absent. In LSBO patients in whom absence of dysplasia can be confirmed repeatedly, it may be reasonable to extend further surveillance intervals from the currently proposed 3–5 years or even longer. Moreover, the increasing use of endoscopic ablation therapy in NDBO patients is at present not justifiable outside clinical studies. Future studies should focus on the development of a risk score that incorporates demographic, endoscopic, histologic and molecular risk factors, and on improvement of optical recognition of dysplasia. Prospective multicenter study with inclusion of a significant number of uncomplicated BO patients and randomisation to clinical factors and biomarkers are needed.
Acknowledgments
Endoscopic images were kindly provided by Dr AD Koch, Erasmus MC University Medical Center, Rotterdam, The Netherlands.
References
Footnotes
-
Contributors PJFdJ, MvB, WMG, EJK wrote the manuscript. PJFdJ, MvB performed the literature search. PJFdJ, EJK had the idea for the article. PJFdJ is the guarantor.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.