Article Text

Abstract
Background and aims: Glucagon-like peptide 2 (GLP-2) may improve intestinal absorption in short bowel syndrome (SBS) patients with an end jejunostomy. Teduglutide (ALX-0600), a dipeptidyl peptidase IV resistant GLP-2 analogue, prolongs the intestinotrophic properties of GLP-2 in animal models. The safety and effect of teduglutide were investigated in SBS patients with and without a colon in continuity.
Methods: Teduglutide was given subcutaneously for 21 days once or twice daily to 16 SBS patients in the per protocol investigational group, 10 with end jejunostomy (doses of 0.03 (n = 2), 0.10 (n = 5), or 0.15 (n = 3) mg/kg/day), one with <50% colon in continuity (dose 0.03 mg/kg/day), and five with ≥50% colon in continuity (dose 0.10 mg/kg/day). Nutrient balance studies, D-xylose tests, and intestinal mucosa biopsies were performed at baseline, on the last three days of treatment, and after three weeks of follow up. Pre-study fasting native GLP-2 levels were determined for the five patients with ≥50% colon in continuity.
Results: Pooled across groups and compared with baseline, teduglutide increased absolute (+743 (477) g/day; p<0.001) and relative (+22 (16)%; p<0.001) wet weight absorption, urine weight (+555 (485) g/day; p<0.001), and urine sodium excretion (+53 (40) mmol/day; p<0.001). Teduglutide decreased faecal wet weight (−711 (734) g/day; p = 0.001) and faecal energy excretion (−808 (1453) kJ/day (−193 (347) kcal/day); p = 0.040). In SBS patients with end jejunostomy, teduglutide significantly increased villus height (+38 (45)%; p = 0.030), crypt depth (+22 (18)%; p = 0.010), and mitotic index (+115 (108)%; p = 0.010). Crypt depth and mitotic index did not change in colonic biopsies from SBS patients with colon in continuity. The most common side effects were enlargement of the stoma nipple and mild lower leg oedema. The improvements in intestinal absorption and decreases in faecal excretion noted after treatment had reversed after the drug free follow up period. A controlled study with a more robust design is ongoing in order to determine the optimal dosage of teduglutide for SBS patients to achieve the maximal effect and utility of this drug in clinical practice.
Conclusion: Teduglutide, at three dose levels for 21 days, was safe and well tolerated, intestinotrophic, and significantly increased intestinal wet weight absorption in SBS patients with an end jejunostomy or a colon in continuity.
- GLP-2, glucagon-like peptide 2
- SBS, short bowel syndrome
- PN, parenteral nutrition
- DPP-IV, dipeptidyl peptidase IV
- AEs, adverse events
- glucagon-like peptide 2
- intestinal adaptation
- intestinal failure
- parenteral nutritional
- short bowel syndrome
- teduglutide
Statistics from Altmetric.com
- GLP-2, glucagon-like peptide 2
- SBS, short bowel syndrome
- PN, parenteral nutrition
- DPP-IV, dipeptidyl peptidase IV
- AEs, adverse events
- glucagon-like peptide 2
- intestinal adaptation
- intestinal failure
- parenteral nutritional
- short bowel syndrome
- teduglutide
The estimated annual prevalence of short bowel syndrome (SBS) patients with non-malignant disease requiring home parenteral nutrition is at least 40 per million of the US population.1,2 In Europe, the point prevalence has been reported to be between 0.6 and 12.7 in various countries.3
SBS usually results from surgical resection of the small bowel for conditions such as Crohn’s disease, mesenteric infarction, congenital anomalies, and multiple strictures due to adhesions or radiation. SBS patients suffer from malabsorption that may lead to malnutrition, dehydration, and weight loss. Some patients can maintain their protein and energy balance through hyperphagia; more rarely they can sustain fluid and electrolyte compensation to become independent of parenteral fluid.
Although long term parenteral nutrition (PN) is life saving in patients with intestinal failure, it is expensive, impairs quality of life,4 and is associated with serious complications such as catheter sepsis, venous occlusions, and liver failure.5 Treatments that amplify absolute intestinal absorption, and eliminate or minimise the need for PN, have great potential significance to SBS patients.
The endogenous meal stimulated hormone, glucagon-like peptide 2 (GLP-2), raises considerable interest for SBS patients. GLP-2 acts to slow gastric emptying,6 reduce gastric secretions,7 increase intestinal blood flow,8 and stimulate growth of the small and large intestine.9 In animal studies, GLP-2 administration induces mucosal epithelial proliferation in the stomach, and small and large bowel by stimulation of crypt cell proliferation9 and inhibition of enterocyte apoptosis.10
SBS patients with end jejunostomy and no colon have limited meal stimulated GLP-2 secretion11 due to removal of GLP-2 secreting L cells which are located primarily in the terminal ileum and colon. GLP-2 deficiency could aggravate gastric hypersecretion, rapid intestinal transit, and lack of intestinal adaptation observed in these SBS patients.
Jeppesen et al have described benefit in an open label study using pharmacological doses of native GLP-2 in SBS jejunostomy patients.12 There was significant improvement in intestinal wet weight absorption and a more modest improvement in energy absorption that led to an increase in body weight, lean body mass, and a rise in urinary creatinine excretion.
In contrast, SBS patients with a colon in continuity have elevated basal and meal stimulated endogenous GLP-2. The potential benefit of pharmacological doses of GLP-2 in these patients has not been studied.
The half-life of native GLP-2 is approximately seven minutes due to enzymatic degradation by dipeptidyl peptidase IV (DPP-IV). A DPP-IV resistant recombinant human GLP-2 analogue, teduglutide, was developed by replacing alanine with glycine in position 2 of the peptide. This is the first study of the safety and effect of three dose levels of teduglutide given for 21 days to SBS patients with either end jejunostomy or colon in continuity.
MATERIAL AND METHODS
Patients
Study subjects were recruited from centres in the US and Denmark that care for patients receiving PN. All patients had undergone extensive resection of the small bowel without any surgical resection of the stomach, duodenum, or pancreas.
Study inclusion criteria were: over 18 years of age; diagnosis of SBS that could be secondary to Crohn’s disease, volvulus, injury, or vascular ischaemia; remnant small bowel of <150 cm; no clinical suspicion of active inflammatory bowel disease or fistulas; no history of radiation enteritis or sprue; no alcohol or drug abuse; no significant renal, hepatic, or cardiac diseases; no glutamine for at least four weeks prior to screening; no growth factors; and no participation in any clinical trial within three months of screening (except for the use of teduglutide in patients in the rechallenge group). SBS patients with ⩾50% colon in continuity had a demonstrated faecal weight exceeding 1 kg/day and faecal energy loss exceeding 2 MJ/day (478 kcal/day).
Women of childbearing age had to have a negative blood β-human chorionic gonadotropin test before inclusion in the study and use effective contraceptives during the study. Usual medications such as proton pump inhibitors, codeine, loperamide, and oral and parenteral supplements were kept constant. Local ethics committees or institutional review boards approved the protocol. Procedures were in accordance with the ethical standards of the Helsinki Declaration of 1964, as modified by the 48th World Medical Association in 1996. Each eligible patient gave written informed consent prior to the study.
Study protocol
This was an open label pilot study to determine the safety and effect of teduglutide in patients with SBS. The patient’s history was reviewed and a physical examination performed to determine eligibility before inclusion in the study. Estimated residual small bowel and colon lengths were determined by reviewing operative reports and available radiographic studies. Eligible patients were admitted as inpatients to hospital wards or General Clinic Research Centres (GCRC) on three separate occasions, 18 days apart, for the last four days and three nights of the baseline period and at the end of the treatment and follow up periods. Treatment consisted of recombinant teduglutide (supplied by NPS Allelix, Mississauga, Ontario, Canada) formulated as a lyophilised powder with L-histidine, mannitol, and monobasic and dibasic sodium phosphate (lot 8502901). Water was added to reconstitute the drug for administration by subcutaneous injections in the abdomen or thigh. Twelve SBS patients with jejunostomy received 0.03 mg/kg/day (n = 3), 0.10 mg/kg/day (n = 5), or 0.15 mg/kg/day (n = 4) once daily. Doses were chosen to examine dose response in SBS patients over a range of doses expected to provide clinical benefit. Single doses up to 10 mg (equivalent to approximately 0.10 mg/kg) were shown to be safe and well tolerated when administered to normal volunteers (previous study, data not presented). Based on the pharmacological, toxicological, and pharmacokinetic profile available when the protocol was prepared, doses of teduglutide 25% log above (0.15 mg/kg) and 50% log below (0.03 mg/kg) the 0.10 mg/kg dose were included in this pilot study. Five patients from the two highest dosing groups were rechallenged with a divided dose (0.05 mg/kg or 0.075 mg/kg every 12 hours) at least three months after their initial participation to investigate antibody formation and to evaluate twice daily dosing. Five SBS patients with ⩾50% colon in continuity received teduglutide 0.10 mg/kg/day once daily. This dose was given because it was expected to provide clinical benefit based on animal data and was tested in patients with end jejunostomy.
During each inpatient period, patients underwent 72 hour nutrient balance and D-xylose absorption studies, and a proximal or distal bowel endoscopy to ascertain the condition of the intestinal mucosa and obtain biopsy samples (not repeated in rechallenge patients). In jejunostomy patients, biopsies were obtained through the jejunostomy stoma or by upper gastrointestinal endoscopy. In patients with colon in continuity, colorectal biopsies were obtained. Teduglutide treatment began on day 1 (immediately after the baseline period) and continued once daily (or twice daily in rechallenge patients) for 21 days. On the first and last day of dosing, all patients had blood collections for plasma levels and pharmacokinetic parameters (submitted for publication, results to be presented separately13), and to test for any antibodies to teduglutide or Escherichia coli protein. Whereas pretreatment antibodies to teduglutide were not expected and served as a control, teduglutide was recombinantly produced in E coli and pre-existing antibodies to E coli were possible. Patients were monitored for safety (adverse events, physical examinations, vital signs, ECGs, laboratory results, and injection site examinations) during the inpatient periods and during outpatient visits on days 7 and 14.
The 72 hour nutrient balance studies were completed with each patient eating their usual diet, calculated from a seven day food diary completed by the patient during the screening period. It was intended that dietary intake should be fixed during balance studies and the study did not seek to evaluate the effects of teduglutide on spontaneous dietary intake. During the 72 hour balance periods, all oral intake (duplicate meals and beverages and declined food), faecal/stomal output, and urine were collected and weighed. All stool samples were refrigerated during the collection period. Stools and diets were separately homogenised and analysed by MDS Clinical Trial Laboratories for energy content (bomb calorimetry),14 nitrogen (macro-Kjeldahl’s method),15 fat (gravimetric technique),16 and sodium and potassium (atomic absorption).17
D-xylose was used to test intestinal carbohydrate absorption.18 After an overnight fast, patients drank a test solution of 25 g D-xylose in 200 ml of distilled water over a 2–3 minute period. A blood sample was taken at two hours and urine collected for five hours following ingestion.
Morphological analysis
Endoscopic examinations were performed in each subject at completion of baseline, treatment, and follow up phases. Tissue samples for measurement of villus height and crypt depth were prepared and analysed in a blinded fashion by the same pathologist. Villus height and crypt depth were measured using light microscopy (eyepiece micrometer) as the mean of 10 well oriented villi and crypts. The number of mitotic figures per 100 crypt epithelial cells was calculated.
Body weight
Body weight was measured on a levelled platform scale every morning before breakfast after patients emptied their bladder and stoma bag. Mean body weight was calculated for four consecutive days.
Statistics
A test for normality was performed justifying parametric statistical testing in this study. Using the SAS (version 8.2; SAS Institute, Cary, North Carolina, USA) statistical program, a Student’s paired t test was employed that compared treatment with baseline values, and follow up with baseline values. Absolute intestinal absorption was calculated as equivalent to the difference between ingestion and excretion, and relative absorption as (diet−faecal)/diet×100%. No comparisons were made between patients on different doses or with different anatomy due to the limited number of patients in the study. Data are expressed as mean (SD). A value of p<0.05 was considered significant.
RESULTS
Patients
Eighteen SBS patients (11 females, seven males) were enrolled in this open label, multicentre, dose ranging pilot study. Four US sites recruited six (two, two, one, one) patients and one Danish site recruited 12 patients. Of the 18 patients, 17 patients received teduglutide; one female patient was discontinued prior to treatment due to intercurrent disease. Baseline characteristics of these 17 patients are given in table 1. Patient 09 experienced a long septic episode and was excluded from the effect analysis due to this destabilisation. A total of 16 SBS patients comprised the overall per protocol investigational group (group 1). These 16 patients were subdivided into an end jejunostomy group of 10 (group 2) and a ⩾50% colon in continuity group of five (group 3). There were originally 11 jejunostomy patients but patient 03 was found on biopsy to have a remnant segment of colon, later estimated to be 30%. This individual was kept in group 1 but was not included in any subgroup analysis. As judged from analysis of duplicate meals adjusted for declined food, some patients had better dietary consistency than others. It was intended that dietary intake was fixed during the balance studies and the study did not seek to evaluate the effects of teduglutide on spontaneous dietary intake. Patients who had an oral food intake where the dietary wet weight and energy content at treatment did not differ by more than 10% from baseline values were termed “high dietary compliance”. Ten patients had a high dietary compliance (<10% variability from baseline value), five with end jejunostomy and five with ⩾50% colon in continuity (group 4). Five end jejunostomy patients who received teduglutide 0.10 or 0.15 mg/kg/day as a single dose were later rechallenged with a divided dose (0.05 or 0.075 mg/kg twice daily). Their first single dose treatment (group 5) was compared with the second divided dose treatment (group 6).
Patient characteristics
Of the 17 patients treated, three with colon in continuity did not require either PN or parenteral fluids, two end jejunostomy patients required fluids only, and 12 patients required both PN and fluids (table 1).
In the 16 SBS patients where the treatment effect was analysed (group 1), mean age was 49.5 (13.0) years (range 27–74), mean weight was 58.4 (12.4) kg (range 38.9–79.2), mean height was 168 (7) cm (range 158–180), and mean body mass index was 20.7 (3.9) kg/m2 (range 15.0–26.9). Twelve of the 16 SBS patients used antidiarrhoeal medications, and 14 patients used antisecretory medications, including one (patient No 12) that took octreotide.
Compliance
Jejunostomy patient No 03, who was found to have a segment of colon in continuity, and patient 15C, known to have colon in continuity, did not complete the follow up period. Drug compliance (counting the number of returned vials) was complete in all patients participating during the nutrient balance periods. During the 21 day treatment period, drug compliance was complete, except in one patient with colon in continuity who administered the full dose for 15 days, half doses for two days, and no dose for four days. Of the five rechallenged patients, two administered for 21 days twice daily, two administered for 20.5 days twice daily, and one administered for 19.5 days twice daily.
Safety results
All patients were monitored for safety. There were no deaths and no withdrawals due to adverse events (AEs). Four of the treated patients reported five serious AEs which included dehydration, sepsis, and catheter related infection. None of the serious AEs were judged to be related to the study drug. Dehydration is common in conditions with fever and changes in oral intake. Two patients (patient 09 (table 1) 0.15 mg/kg once daily and patient 6R (table 1) 0.05 mg/kg twice daily) became dehydrated. The first patient had sepsis and dehydration that began two days after completing the dosing portion of the study. The second patient had dehydration that began during the screening period (two days prior to the dosing portion of the study) and resolved six days later. The incidence of AEs was similar between groups. The most common AEs were oedema of the lower limbs (7/16 patients, 44%), and localised swelling of the jejunostomy nipple (7/10 patients, 70%). All five rechallenged patients (group 6) showed this AE at least once in both 21 day treatment cycles. Other AEs included headache (4/16 patients, 25%) and abdominal pain (3/16 patients, 19%), two had Crohn’s disease and colon in continuity. Examination of the jejunal or colon biopsy samples did not reveal any cases of reactivation of Crohn’s disease. Three patients had minor injection site reactions (single events of bruising, induration, rash; four events of erythema). No clinically significant abnormal laboratory values were identified in relation to teduglutide treatment. No safety concerns were raised from vital signs or ECGs. No antibodies to teduglutide were detected. One patient had a relative E coli protein antibody titre of 1:1624, and six patients had relative titres between 1:107 and 1:228 after treatment.
Endogenous GLP-2 levels
For patients with ≥50% colon in continuity, fasting concentrations of endogenous GLP-2 were measured prior to administration of teduglutide. For four of the five subjects, their concentrations were closer to the fed state for healthy fasting volunteers (fasted 15 (2) pmol/l; fed 61 (9) pmol/l).19 Levels for the five subjects were 16, 27, 37, 41, and 73 pmol/l. Neither baseline nor endogenous meal stimulated GLP-2 secretions were evaluated in SBS patients with end jejunostomy in this study.
Effects of teduglutide
Wet weight
Figure 1 illustrates faecal wet weight, intestinal wet weight absorption, and urine weight in individual patients in group 1 at baseline, during treatment, and at follow up. A 21 day treatment with teduglutide significantly decreased faecal wet weight compared with baseline values in the entire group of SBS patients (group 1, 711 (734) g/day; p = 0.001) and in each subgroup (groups 2–6; table 2). The decrease was similar in those with end jejunostomy (group 2, 682 (911) g/day; p = 0.040) and those with colon in continuity (group 3, 822 (341) g/day; p = 0.006). Absolute wet weight absorption was obtained by subtracting faecal wet weight from diet wet weight. Teduglutide increased absolute wet weight absorption in 15 of 16 SBS patients compared with baseline. These increases were significant for all groups and closely reflected the decreases in faecal output. Absolute wet weight absorption increased as a per cent of intake in 14 of 16 SBS patients. The increase in relative absorption was 22 (16)% (p<0.001) in group 1 (SBS patients; once daily dosing). The magnitude was similar for SBS patients with end jejunostomy (group 2, 20 (18)%, p = 0.007) and those with ⩾50% colon in continuity (group 3, 26 (16)%; p = 0.023). As expected from the increases in intestinal wet weight absorption, teduglutide increased urine weight in 14 of 16 SBS patients (group 1, 555 (485) g/day; p<0.001) (table 3). Similar increases were seen in those with end jejunostomy (group 2, 680 (535) g/day; p = 0.003) and those with ⩾50% colon in continuity (group 3, 461 (200) g/day; p = 0.007).
Wet weight, sodium, and potassium: faecal excretion, and absolute and relative absorption
Urine wet weight, sodium and potassium
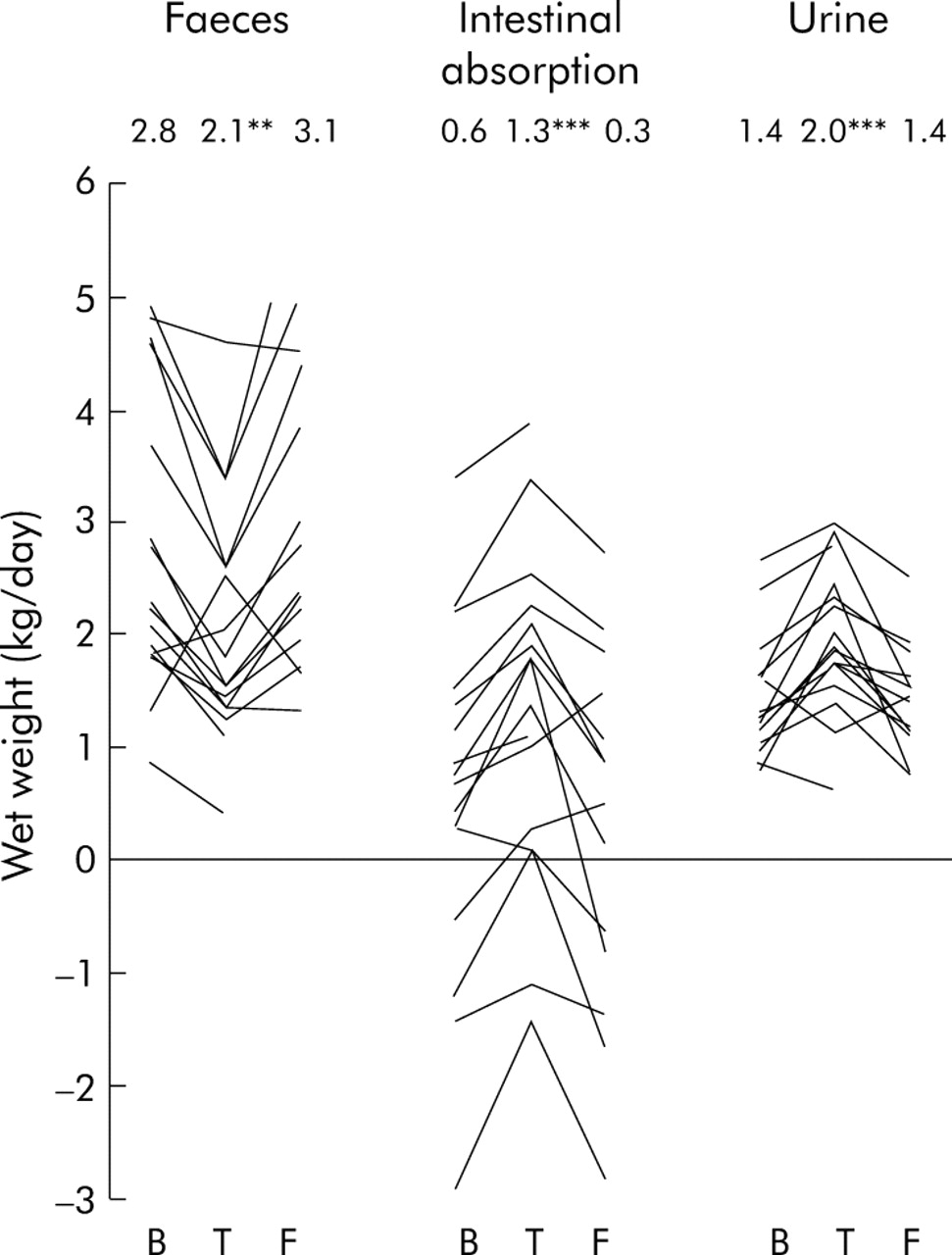
Faecal wet weight, intestinal wet weight absorption, and urine weight in individual patients in group 1 at baseline (B, days –3 to 0), during treatment (T, days 18–21), and at follow up (F, days 39–42).
Sodium and potassium
Faecal sodium decreased and sodium absorption increased, but only relative absorption (table 2), and increased urine excretion (table 3) reached statistical significance. Faecal potassium decreased significantly (table 2) but this was not reflected in significant changes in intestinal absorption or urinary excretion.
Energy
Figure 2 illustrates faecal energy excretion and intestinal energy absorption in individual patients in group 1 at baseline, during treatment, and at follow up. Compared with baseline, the 16 SBS patients had significant decreases in energy excretion on teduglutide (group 1, 808 (1453) kJ/day (193 (347) kcal/day); p = 0.042) (table 4). This reduction was also significant in those with colon in continuity (group 3, 1343 (916) kJ/day; p = 0.031) and those with high dietary compliance (group 4, 1060 (1083) kJ/day; p = 0.013). Significant effects were also seen with improved energy absorption (group 3, 1027 (798) kJ/day, p = 0.045; group 4, 963 (1290) kJ/day, p = 0.043) and relative energy absorption (group 3, 10 (7)%, p = 0.030; group 4, 8 (11)%, p = 0.040).
Energy, fat, and nitrogen: faecal excretion, and absolute and relative absorption

{kind=link}
{kind=link}
Faecal energy excretion and intestinal absorption in individual patients in group 1 at baseline (B, days −3 to 0), during treatment (T, days 18–21), and at follow up (F, days 39–42).
Fat and nitrogen
Faecal fat and nitrogen losses tended to decrease and intestinal absorption tended to increase but were not statistically significant.
D-xylose
Plasma absorption measured at two hours increased with teduglutide in 14 of 16 SBS patients but the overall change was not significant (53 (48)%; p = 0.060). Five hour urinary D-xylose excretion did not change.
Body weight
Eleven of 16 SBS patients increased their weight while on teduglutide but the mean increase (0.9 (2.1) kg) was not statistically significant (p = 0.120) (table 5). The weight increase was significant (2.2 (1.1) kg; p = 0.010) in rechallenged patients who also had the best absolute and relative energy absorption.
Body weight
Biopsies
Significant histological changes in relation to teduglutide treatment were seen in the jejunum in seven of eight group 2 patients who were biopsied. There was an increase in villus height (38 (45)%; p = 0.030), crypt depth (22 (18)%; p = 0.010), and mitotic index (115 (108)%; p = 0.010). Small bowel biopsies were not obtained from patients with colon in continuity (group 3). Biopsies for measurements of colonic crypt depth were obtained in all five patients in group 3. Crypt depth increased in four of five sets of colonic biopsies following teduglutide treatment but the mean increase of 13 (22)% did not reach statistical significance (p = 0.330) and the increase in mitotic index was not significant (76 (112)%; p = 0.170). Most changes in intestinal absorption and histology related to teduglutide treatment had reversed at follow up.
DISCUSSION
The main findings in this study were significant effects of teduglutide on reducing intestinal wet weight excretion and improving wet weight absorption in SBS patients. These effects were even seen in SBS patients with colon in continuity, most of whom had increased endogenous GLP-2 concentrations. The 16 SBS patients in group 1 had significantly increased absolute (743 (477) g/day; p<0.001) and relative (22 (16)%, p<0.001) wet weight absorption, increased urine production (555 (485) g/day; p<0.001), and decreased faecal wet weight excretion (711 (734 g/day; p = 0.002). Effects of equal magnitude were seen in both SBS patients with end jejunostomy and those with ⩾50% colon in continuity. These effects were seen in steady state SBS patients who were optimally treated with conventional antisecretory and antidiarrhoeal medication.
The effects of teduglutide on wet weight absorption were almost twofold those in the pilot study of native GLP-2 for 35 days (420 (480) g/day; p = 0.040), conducted in patients with similar baseline wet weight absorption.12 This greater effect could be related to differences in dose and half life of GLP-2 and teduglutide, respectively. In the pilot study with native GLP-2, 400 μg was given twice daily (corresponding to 0.013 (0.002) mg/kg/day; range 0.011–0.017). The teduglutide doses in the current study were 3–10 times higher, ranging from 0.03 to 0.15 mg/kg/day. Replacement of alanine by glycine in position 2 of GLP-2 blocks degradation by DPP-IV, extending the half life from approximately seven minutes (GLP-2) to 0.9–2.3 hours (teduglutide).13 With only two, five, and three end jejunostomy patients receiving 0.03, 0.10, and 0.15 mg/kg/day of teduglutide, respectively, this study was not able to detect differences between dosing groups. The study was closed before all planned patients had been enrolled due to slow enrolment. Food control for wet weight intake was poor in one patient who received 0.03 mg/kg/day teduglutide, leaving only one patient for evaluation (table 1). Effects on wet weight absorption were of similar magnitude in the 0.10 and 0.15 mg/kg/day teduglutide dosing groups (958 (450) g/day and 987 (479) g/day, respectively), suggesting a plateau was reached at 0.10 mg/kg/day teduglutide or lower. Whether a longer duration of teduglutide treatment would lead to a greater effect remains to be established. Divided doses did not seem to have a substantially greater effect but the limited number of patients in this study does not permit firm conclusions.
Although effects on intestinal sodium excretion and absorption did not reach statistical significance, similar to the study with native GLP-2, there was a significant increase in urinary sodium excretion of 53 (40) mmol/day (p<0.001) following teduglutide treatment and this is best explained by decreases in faecal sodium excretion and increases in intestinal sodium absorption, since the supply of parenteral sodium was kept constant.
In this study, the effects of teduglutide on energy and macronutrient absorption were minor compared with effects on wet weight absorption. Although a decrease in faecal energy excretion (808 (1453) kJ/day (193 (347) kcal/day); p = 0.04) was demonstrated in group 1 SBS patients, this did not translate into significant increases in absolute or relative energy absorption. The inability to show a significant effect may be due to variability in dietary energy intake during the study periods. Group 4 patients with high dietary compliance and low variability of dietary intake during study periods did have a small but significant decrease in faecal energy excretion (1060 (1083) kJ/day (253 (259 kcal/day); p = 0.01) (table 4). This translated into a significant increase in absolute (963 (1290) kJ/day (230 (308 kcal/day); p = 0.04) and relative (10 (7)%; p = 0.03) intestinal energy absorption. It was not possible to demonstrate an effect on intestinal fat or nitrogen absorption.
The effect of teduglutide on absolute energy absorption was twofold higher than with native GLP-2 (441 (634) kJ/day (105 (151 kcal/day)); p = 0.09) at the given doses and treatment periods.12 Thus in contrast with H2 receptor antagonists, proton pump inhibitors, and octreotide, native GLP-2 and teduglutide seem to affect both intestinal wet weight and energy absorption, with an additional positive effect on wet weight absorption in patients already treated with these agents.20
Several physiological mechanisms may account for the positive effects seen on intestinal absorption with teduglutide treatment. SBS patients with end jejunostomy, who have limited or no endogenous meal stimulated GLP-2 secretion,11 often suffer from gastric hypersecretion and rapid gastric emptying, at least initially after enterectomy. GLP-2 has been shown to diminish gastric acid secretion in sham fed healthy humans7 and prolong gastric emptying in SBS patients.12 Therefore, it is likely that a pharmacological replacement may restore the physiological feedback, previously described as the ileal brake mechanism. This is the first human study demonstrating the intestinotrophic properties of a GLP-2 analogue, which need to be verified in a controlled study. No other pharmacological agents have been able to promote a significant adaptation of this magnitude, possibly as a result of increasing the absorptive surface area of the intestine. In SBS patients with end jejunostomy, teduglutide significantly increased small bowel villus heights (38 (45)%; p = 0.030), crypt depth (22 (18)%; p = 0.010), and mitotic index (115 (108); p = 0.010).
The mechanisms regarding the effect of teduglutide in SBS patients with colon in continuity are more speculative. These patients have continuously high endogenous GLP-2 secretion,21 with normal gastric secretion and emptying. However, supraphysiological doses of teduglutide may produce local high concentrations that suppress gastric secretion and induce small bowel growth. Small bowel biopsies were not obtained in these patients. In SBS patients with and without colon in continuity, upregulation of transport proteins is possible, as described in animal studies.22–24
Regardless of the exact physiological mechanism, increases in intestinal absorption in relation to treatments that improve intestinal adaptation would preferably be converted into positive effects regarding body weight or composition, hydration, physical activity, and ultimately quality of life. The latter two points were not examined in either study quoted here. Body weight did not significantly increase following teduglutide treatment (0.9 (2.1) kg; p = 0.120).
The type and severity of adverse events will be an important issue when considering long term treatment in SBS patients. In this population, serious AEs were related to the underlying condition and AEs (enlargement of stoma nipple and mild lower leg oedema) were related to the pharmacodynamic effects of teduglutide. The increase in intestinal wet weight absorption may contribute to peripheral oedema, which can be treated by reducing parenteral volume.
The pharmacodynamics of teduglutide appear to be gut specific and AEs are limited. Therefore, teduglutide may have a role in the long term treatment of SBS patients. The 0.75 l of improved wet weight absorption has significant clinical implications for this SBS patient population (for example, less PN or fewer infusion days/weeks). Spending less time on parenteral infusions may be valuable for the quality of life in these patients. Non-PN dependent SBS patients may also be candidates for this treatment. Many of these patients suffer from repeated episodes of dehydration, renal insufficiency, and kidney stones. Increasing wet weight absorption in these patients may diminish those complications of SBS.
Future controlled studies with a more robust design are needed to determine the optimal dosage and administration of teduglutide to SBS patients to achieve the maximal effect. Subsequent studies will determine whether optimal dosage and administration of teduglutide will result in long term improvements in fluid balance, nutritional status, and independence from parenteral support in some SBS patients, thereby improving their overall quality of life. As a result of the positive findings of this study, a multicentre, multinational, controlled evaluation is now in progress.
Acknowledgments
We thank G Carron, B Bath, L Demchyshyn, C Blosch, J Lopansri, T Considine, and S Peers. The General Clinical Research Centres at Emory University School of Medicine (NIH RR 00039) and Northwester University (NIH 00048) were utilised for subjects studied at these sites.
REFERENCES
Supplementary materials
Competing interests: EL Sanguinetti and J Gregory are employees of NPS Pharmaceuticals Inc. PB Jeppesen, A Buchman, L Howard, T R Ziegler, K A Tappenden, J Holst, and P B Mortensen have served as consultants and received research support from NPS Pharmaceuticals Inc. J S Scolapio has no competing interests.