Article Text

Abstract
Background and aims: Longstanding ulcerative colitis (UC), especially in the presence of epithelial dysplasia, is associated with an increased risk of developing cancer. As dysplasia is not visible during routine endoscopy, at least 40–50 random biopsies in four quadrants every 10 cm are recommended. Fluorescence endoscopy after sensitisation with 5-aminolaevulinic acid (5-ALA) was assessed for the detection of dysplasia in ulcerative colitis by taking optical guided biopsies. 5-ALA is converted intracellularly into the sensitiser protoporphyrin IX which accumulates selectively in neoplastic tissue allowing the detection of dysplasia by typical red fluorescence after illumination with blue light.
Methods: In 37 patients with UC, 54 examinations were performed with fluorescence endoscopy after oral (20 mg/kg) or local (either with an enema or by spraying the mucosa with a catheter) sensitisation with 5-ALA. A total of 481 biopsies of red fluorescent (n=218) and non-fluorescent (n=263) areas of the colonic mucosa were taken.
Results: Forty two biopsies in 12 patients revealed either low grade (n=40) or high grade (n=2) dysplasia. Sensitivity of fluorescence for dysplastic lesions was excellent and ranged from 87% (95% confidence interval (CI) 0.73–1.00) to 100% (95% CI 1.00–1.00) after local sensitisation, in contrast with only 43% (95% CI 0.17–0.69) after systemic administration. Specificity did not differ for both forms of local sensitisation (enema 51% (95% CI 0.44–0.57) and spray catheter 62% (95% CI 0.51–0.73)); after systemic sensitisation specificity was 73% (95% CI 0.69–0.83). Negative predictive values of non-fluorescent mucosa for exclusion of dysplasia were very high; 89% after systemic sensitisation and 98–100% after local sensitisation. Positive predictive values were 13% and 14% after local sensitisation with enema and spray catheter, and 21% after oral sensitisation with 20 mg/kg ALA. The overall number of biopsies per examination was less than five from fluorescent positive areas.
Conclusion: Fluorescence endoscopy after 5-ALA sensitisation is a possible tool to visualise dysplastic lesions in ulcerative colitis using 5-ALA sensitisation. Local sensitisation is a promising alternative approach compared with systemic administration of 5-ALA. A randomised controlled study is now indicated to compare the efficacy of endoscopic fluorescence detection with the standard technique of four quadrant random biopsies.
- ulcerative colitis
- dysplasia
- fluorescence endoscopy
- 5-aminolaevulinic acid
- 5-ALA, 5-aminolaevulinic acid
- PPIX, protoporphyrin IX
- FE, fluorescence endoscopy
- UC, ulcerative colitis
Statistics from Altmetric.com
- 5-ALA, 5-aminolaevulinic acid
- PPIX, protoporphyrin IX
- FE, fluorescence endoscopy
- UC, ulcerative colitis
The most significant predictor of the risk of malignancy in patients with inflammatory bowel disease is the presence of dysplasia in colonic mucosa.1 Unfortunately, 95% of these lesions appear in flat mucosa with no or non-specific macroscopic characteristics.2 Four quadrant random biopsies every 10 cm is the procedure of choice to detect dysplasia in flat mucosa but this technique is limited by a high sampling error.3
Optical guided biopsies by fluorescence endoscopy (FE) could be a useful technique to avoid sampling errors in the detection of dysplasia and reduce the overall number of biopsies. A sensitiser, which accumulates selectively in malignant and premalignant tissue, fluoresces under blue light excitation and enables targeted biopsies.
5-Aminolaevulinic acid (5-ALA), a prodrug in haeme biosynthesis, which is converted intracellularly into the sensitising agent protoporphyrin IX (PPIX), seems to be an attractive substance for FE. Due to a low ferrochelatase activity in tumour cells, PPIX accumulates selectively in malignant tissue.4 Furthermore, PPIX is associated with limited skin photosensitivity of 1–2 days.5 Promising results for FE of bronchial6 and bladder7 tumours after 5-ALA sensitisation have been reported. For the first time, we have demonstrated previously in an animal colitis model that it may be possible to detect dysplastic lesions even with the “naked eye” in a dose dependent manner after sensitisation with 5-ALA.8
The aim of this study was to assess the feasibility of detecting or excluding dysplasia in patients with chronic ulcerative colitis (UC) by FE using various sensitisation modes.
PATIENTS AND METHODS
Patient population
Thirty seven patients (22 female, 15 male, median age 46 years) with endoscopically and histologically proven UC for more than five years gave their written consent to take part in the study and underwent a total of 54 colonoscopies. The protocol was approved by the ethics committee of the medical faculty of the University of Regensburg.
Pre-examination and study criteria
As mentioned above, patients with longstanding (>5 years) and a minimal diagnosis of left sided UC willing to take part in the study were included. Patients with acute or chronic liver disease or those with known porphyria were excluded. All patients were examined by ultrasonography, and serum liver parameters (transaminases, bilirubin, alkaline phosphatase, pseudocholinesterase) were assessed to exclude liver disease as 5-ALA can induce a transient increase in liver enzymes.
Furthermore, only patients in clinical remission were examined as acute inflammation is known to induce false positive fluorescence.8 The activity of UC is defined analogous to the UC scoring system.9
Sensitisation and fluorescence endoscopy
After conventional colon lavage, patients were sensitised orally with 20 mg/kg body weight 5-ALA (Medac GmbH, Hamburg, Germany) dissolved in orange juice, or locally either by enema (3 g 5-ALA dissolved in 250 ml NaCl 0.9% for one hour) or by spraying the 5-ALA solution onto the colonic mucosa with a spray catheter (5-PWL; Olympus, Hamburg, Germany). After local sensitisation, the patient was advised to turn around in order to ensure that the whole colon was covered by the enema. FE was performed 4–6 hours after systemic and 1–2 hours after local sensitisation.
Endoscopy was performed using fibrescopes (CF-1T20L; Olympus, Hamburg, Germany) connected to a light source delivering white or blue light (D-light; Storz, Tuttlingen, Germany), emitting blue light at a wavelength of 390–405 nm. The endoscope was adapted to a camera (Endovision Telecam SL; Storz) with an imaging processing module delivering real time fluorescence pictures. A yellow band pass filter (Storz) was used to connect the ocular of the endoscope to the camera.
Biopsies were taken first under blue light from fluorescent (n=218) and, after switching to conventional white light, randomly from non-fluorescent (n=263) areas. The pathologist was blinded to the fluorescence status of biopsies. For histological diagnosis, conventional 5 μm cryostat sections were cut at different depths of the biopsy, and stained with haematoxylin and eosin.
Statistical analysis
Descriptive values are expressed as median (range) for age and number of biopsies. Statistical analysis was performed using the χ2 test with Yates’ correction. Probabilities of less than 0.05 were accepted as significant. Asymptotic 95% confidence intervals (95% CI) for sensitivity and specificity were calculated using SAS version 8.1.
RESULTS
A total of 54 examinations in 37 patients with histologically proven colitis of more than five years’ duration were included. Fourteen patients had pancolitis and 23 had left sided colitis. Median age, duration, and extent of disease of the study population are shown in table 1.
Distribution of the study population with respect to age, and extent and duration of ulcerative colitis
Detection of dysplasia with FE
A total of 481 biopsies were examined; the number of biopsies taken from fluorescent positive (n=218) and negative (n=263) areas was almost similar (see table 4).
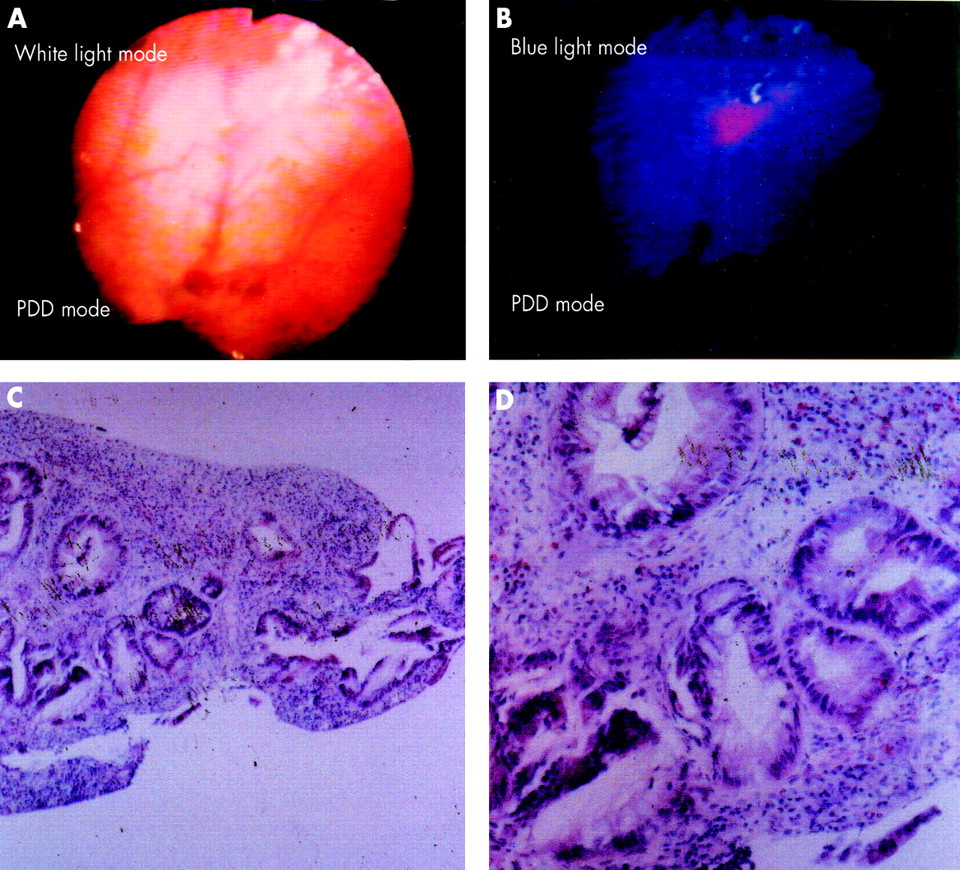
Forty two biopsies in 12 patients showed either low grade (n=40) (fig 1A–D) or high grade (n=2) dysplasia; no carcinoma was found. After local sensitisation, three cases of low grade dysplasia (3/28) were found in biopsies from non-fluorescent areas but the two cases of high grade dysplasia were from areas with red fluorescence (fig 2). The remaining 23 biopsies with low grade dysplasia were also from fluorescent areas. After systemic sensitisation with 20 mg/kg 5-ALA, 14 biopsies contained low grade dysplasia—6 (43%) from fluorescence positive and 8 (57%) from fluorescence negative areas (details of biopsies with histological diagnosis of dysplasia are summarised in tables 2 and 3).
Distribution of dysplasia positive biopsies with respect to their fluorescence
Distribution of dysplasia containing biopsies with respect to fluorescence
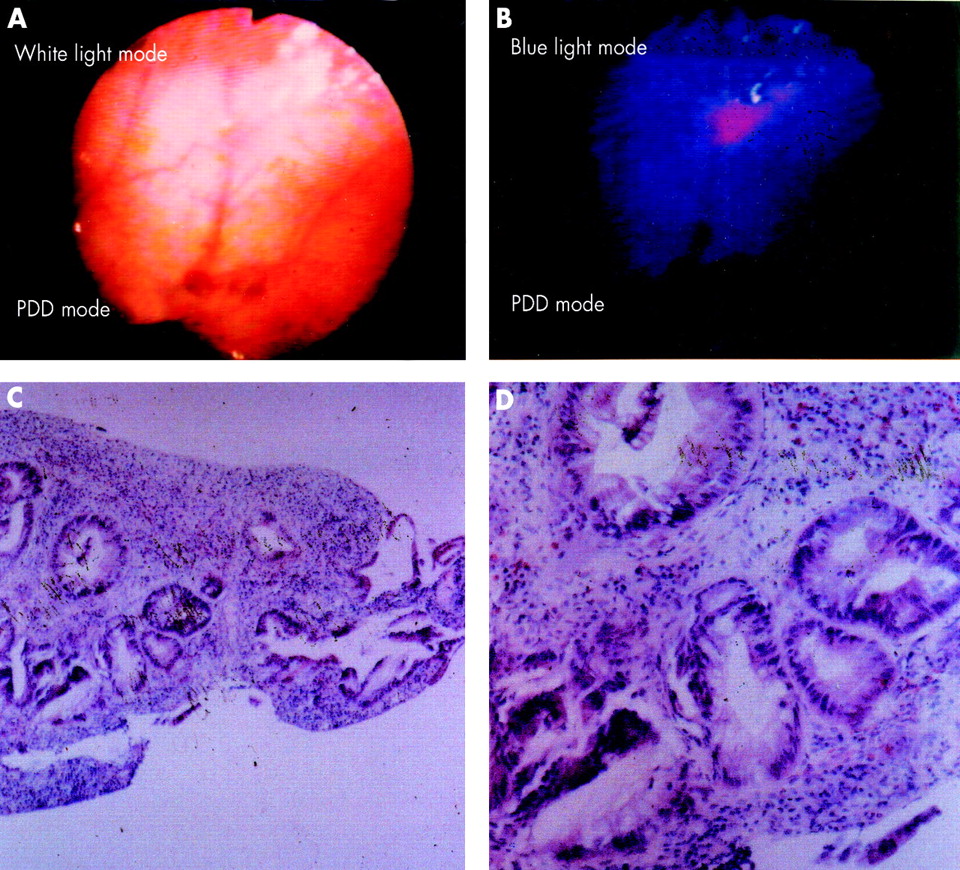
Endoscopic fluorescence images. (A, B) Comparative presentation of regular white light endoscopy (A) and fluorescence endoscopy (B) one hour after local sensitisation with enema. A biopsy from the red fluorescent area presented a flat adenoma with low grade dysplasia, as shown in (C) and (D). (C, D) Haematoxylin and eosin sections of a biopsy of a red fluorescent area showing an overview (C) (magnification 40×) and further enlargement of distorted crypts with irregular and slightly hyperchromatic nuclei (D) (magnification 125×).

{kind=link}
{kind=link}
Endoscopic fluorescence images. (A, B) Comparative presentation of regular endoscopy with white light (A) and fluorescence endoscopy (B) one hour after local sensitisation with enema. A biopsy from the red fluorescent area presented high grade dysplasia.
The mean number of biopsies per examination, including some random biopsies under white light, varied from 8.3 (systemic sensitisation) to 8.4 (local with spray catheter) to 9.3 (local sensitisation with enema). When only fluorescent positive biopsies were considered, 4.8 (enema), 3.5 (spray catheter), and 2.4 (systemic) biopsies per examination were necessary.
False positive fluorescence was mainly induced by inflammation, margin of ulcers, and faeces. As contamination with faeces could be washed off, no biopsies were taken from these areas.
Sensitivity and specificity for detection of dysplasia varied with the different application modes of 5-ALA: sensitivity after 20 mg/kg 5-ALA orally was low (43% (95% CI 0.17–0.69)). However, local sensitisation with enema increased sensitivity to 87% (95% CI 0.73–1.00) (p=0.015) and after local sensitisation with spray catheter to 100% (95% CI 1.00–1.00) (p=0.09). In contrast, specificity after sensitisation with 20 mg/kg orally (73% (95% CI 0.69–0.83)) was higher (p<0.001) compared with the local sensitisation mode with enema (51% (95% CI 0.44–0.57)) whereas specificity after local sensitisation with the spray catheter did not differ significantly (table 5). Distribution of dysplasia positive and negative biopsies with respect to their fluorescence is shown in table 4.
Distribution of biopsies with respect to dysplasia and fluorescence positive and negative status for different application modes
Positive predictive values were 13% and 14% after local sensitisation with enema and spray catheter, and 21% after oral sensitisation with 20 mg/kg ALA (table 5). Negative predictive values of non-fluorescent mucosa for exclusion of dysplasia were very high; 89% after systemic sensitisation and 98–100% after the local sensitisation mode with enema and spray catheter.
Sensitivity, specificity, and positive and negative predictive values of fluorescence for dysplastic lesions after different sensitisation forms using 5-ALA
It is noteworthy that after local sensitisation with enema, fluorescence was visible even in the ileocaecal area, indicating that the enema covered the entire colon.
Side effects
Only one patient complained of nausea and vomiting. This patient was sensitised with 20 mg/kg 5-ALA orally. A transient increase in liver enzymes was found in the same patient. In total, a threefold increase in liver enzymes was found 24 hours after oral sensitisation with 5- ALA (20 mg/kg) in two patients. In both cases enzymes normalised within one week. After local sensitisation there was no increase in liver enzymes. There was no significant decrease in blood pressure in the three groups over 24 hours of monitoring. None of the patients complained of circulatory disorders.
DISCUSSION
Patients with longstanding or extensive UC are at increased risk of developing cancer.1 The most significant predictor of malignancy in patients with inflammatory bowel disease is the presence of dysplasia in colonic biopsies. Dysplastic alterations of the mucosa may occur in flat or raised mucosal lesions. However, 95% of dysplastic foci occur in flat mucosa, most often in macroscopically non-suspicious appearing mucosa.2 To minimise cancer related mortality, patients with longstanding UC are advised to undergo annual or biannual colonoscopic surveillance with random biopsies every 10 cm.3 It has been estimated that at least 33 biopsy specimens have to be taken from the entire colon to achieve a 95% chance of detection of dysplasia when present.10 For illustration, a set of 10 surveillance biopsy samples covers only an estimated 0.05% of the total colonic surface area.11 Therefore, the recommendation of the German Society of Digestive and Metabolic Diseases is to take at least 40–50 biopsies.12
Due to this limitation of conventional endoscopy, new diagnostic tools have been developed with the aim of minimising “sampling errors” in the detection of precancerous lesions. FE based on endogenous or exogenous fluorophores which accumulate selectively in malignant lesions is an interesting approach to obtain optical guided biopsies. In patients with UC, the main aim is to detect or exclude dysplasia in the colon with a high probability and with a minimum of biopsies.
The first promising results for the detection of tumours in the colon of rats with the “naked eye” used a haematoporphyrin derivative (HPD) as a sensitiser.13,14 The use of this complex lipophilic haematoporphyrin derivative is however associated with prolonged skin photosensitivity for approximately 6–8 weeks. In contrast, 5-ALA seems to be more suitable for fluorescence diagnosis as it is associated with only a limited skin photosensitivity of 24 hours and higher tumour selectivity.5 After sensitising with 5-ALA, red fluorescence induced with blue light can easily be detected by the naked eye or with a special camera system.
Previously, we demonstrated that 5-ALA induced photosensitisation enabled the detection of dysplastic lesions in dextran sulphate sodium induced colitis with high sensitivity but low specificity. Sensitivity and specificity were strongly dependent on the drug dose used. False positive fluorescence was mainly induced by inflammation.8
In this study, we assessed the ability of FE to detect dysplasia in patients with UC. We tested local application of 5-ALA either by enema or by spraying the substance with a catheter on the mucosa, based on the assumption that local sensitisation is associated with fewer side effects. FE was performed with both methods 1–2 hours after sensitisation. A third application mode was oral administration of 5-ALA 20 mg/kg body weight.
In our study, we decided to sensitise patients with UC with 20 mg/kg body weight 5-ALA as 100% sensitivity was achieved with this drug dose in patients with Barrett’s oesophagus, with tolerable side effects.15 Regula et al demonstrated that higher concentrations of 5-ALA are needed in the lower compared with the upper gastrointestinal tract to achieve similar selectivity.5 As 8/14 biopsies containing dysplasia did not fluoresce, these data indicate that 20 mg/kg 5-ALA orally may be too low to detect dysplasia in patients with UC. However, increasing the dose would be associated with increased side effects and probably lower specificity.
The higher sensitivity and negative predictive value after local sensitisation indicate that local application is superior to systemic sensitisation in patients with UC. As indicated by positive fluorescence, even in the ileocaecal area after enema, local sensitisation seems appropriate even for patients with pancolitis. In our study, we did not differentiate between low and high grade dysplasia as even the presence of low grade dysplasia requires colectomy.16 The high negative predictive values after local sensitisation with either enema or spray catheter (98% and 100%, respectively) showed that in patients with no selective fluorescence in their colon after local sensitisation with 5-ALA, the presence of dysplasia can almost be excluded.
FE was associated with acceptable side effects. While local sensitisation induced no side effects, systemic application caused mild nausea and vomiting in one patient and a transient increase in liver enzymes in two patients.
Although this is one of the first promising studies reporting that early detection of cancerous and precancerous lesions in patients with UC is possible, in principal, with PDD, we have to stress the limitations of the study. There were only a small number of patients with dysplasia containing biopsies, but to our knowledge this is the highest number of patients with dysplasia used to test a new method of screening for dysplasia. Therefore, the statistical analysis has to be interpreted with caution. Although only patients in clinical remission were included in the study, there were areas with macroscopic and histological signs of inflammation, inducing a high rate of false positive fluorescence. However, methodical errors of the local application mode—for example, unequal absorption of ALA using enema or the spray catheter—have to be considered and cannot be excluded.
It was not the aim of our study to compare fluorescence endoscopy with conventional white light endoscopy but to evaluate the value of fluorescence endoscopy in detecting dysplasia and to optimise the application mode of ALA. We consider the most important result the high negative predictive value, indicating that there is almost no dysplasia in a fluorescence negative colon after local application of ALA.
To date, obtaining four quadrant biopsies every 10 cm is still the gold standard for patients with longstanding and extensive UC. A randomised trial comparing the efficacy in the detection or exclusion of dysplasia in longstanding UC with FE after local sensitisation with 5-ALA and white light endoscopy with random biopsies is now warranted.
Acknowledgments
The study was partly supported by the Wilhelm-Sander-Stiftung, Germany (96.081.2).