Article Text

Abstract
Objective To examine differences in the relative survival and excess death rates of patients with colorectal cancer in Norway, Sweden and England.
Methods All individuals diagnosed with colorectal cancer (ICD10 (International Classification of Diseases, 10th revision) C18–C20) between 1996 and 2004 in England, Norway and Sweden were included in this population-based study of patients with colorectal cancer. The main outcome measures were 5-year cumulative relative period of survival and excess death rates stratified by age and period of follow-up.
Results The survival of English patients with colorectal cancer was significantly lower than was observed in both Norway and Sweden. Five-year age-standardised colon cancer relative survival was 51.1% (95% CI 50.1% to 52.0%) in England compared with 57.9% (95% CI 55.2% to 60.5%) in Norway and 59.9% (95% CI 57.7% to 62.0%) in Sweden. Five-year rectal cancer survival was 52.3% (95% CI 51.1% to 53.5%) in England compared with 60.7% (95% CI 57.0% to 64.2%) and 59.8% (95% CI 56.9% to 62.6%) in Norway and Sweden, respectively. The lower survival for colon cancer in England was primarily due to a high number of excess deaths among older patients in the first 3 months after diagnosis. In patients with rectal cancer, excess deaths remained elevated until 2 years of follow-up. If the lower excess death rate in Norway applied in the English population, then 890 (13.6%) and 654 (16.8%) of the excess deaths in the colon and rectal cancer populations, respectively, could have been prevented at 5 years follow-up. Most of these avoidable deaths occurred shortly after diagnosis.
Conclusions There was significant variation in survival between the countries, with the English population experiencing a poorer outcome, primarily due to a relatively higher number of excess deaths in older patients in the short term after diagnosis. It seems likely, therefore, that in England a greater proportion of the population present with more rapidly fatal disease (especially in the older age groups) than in Norway or Sweden.
- Colorectal neoplasms
- survival
- colorectal cancer
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
The survival of patients with colorectal cancer varies substantially across Europe, and the UK's survival rates compare unfavourably with those of many other countries with comparable health systems and populations.
The majority of the studies investigating survival differences have examined variation at 5 years, but survival differences at earlier time points in the course of disease may be more revealing.
What are the new findings?
The survival of English patients with colorectal cancer was significantly lower than was observed in both Norway and Sweden.
The majority of the survival difference for English patients with colon cancer was due to a high number of excess deaths among older patients in the first 3 months after diagnosis.
There was a similar trend for English patients with rectal cancer, but excess deaths remained elevated until 2 years of follow-up.
If the lower excess death rate of Norway had applied in the English population, then 13.6% and 16.8% of the excess deaths in the colon and rectal populations, respectively, could have been avoided within 5 years of follow-up.
How might it impact on clinical practice in the foreseeable future?
Public health interventions are required to address the poorer short-term survival of English patients with colorectal cancer.
Introduction
The 5-year survival of patients with colorectal cancer has been shown to vary substantially across Europe.1 These differences have caused considerable concern in the UK, where survival rates compare unfavourably with those of many other countries with comparable health systems and populations.2
Before steps can be taken to eliminate the UK survival deficit, it is important to understand how it has arisen.3 There is evidence to suggest that differences in the extent of disease at diagnosis, treatment and co-morbidities may contribute to some of the variation observed,4–6 but further detailed studies are required to understand why the UK has a lower survival proportion relative to many of her economic neighbours.
The majority of international studies of cancer survival have examined differences at 5 years. If variations in the extent of disease at diagnosis or initial treatment account for the observed variations in survival, however, then differences at earlier time points in the course of the disease may be more revealing. For example, recent studies have demonstrated that the greatest differences in survival between the Nordic countries and the UK occurred in the first 6 months after diagnosis.7 8 These differences were also strongly age dependent, with excess mortality and the differences between countries increasing substantially with age. This suggests that fundamental differences do exist between the countries' colorectal cancer populations at diagnosis. Such analyses help, therefore, to identify patient subsets with particularly good or adverse survival outcomes and can be used to help devise strategies that could improve the delivery of healthcare and consequently improve patient survival.
Determination of the origins of survival differences requires a comparison of outcomes across countries with similar populations, healthcare systems and cancer registration processes. Like the UK, both Norway and Sweden have population-based cancer registration systems with complete geographical coverage and a robust means of ascertaining deaths. Age-standardised incidence rates of the disease are similar at ∼62.8, 47.8 and 54.9 cases per 100 000 person-years in males in Norway, Sweden and the UK, respectively.9 The equivalent figures for women are 52.5, 38.4 and 35.4 per 100 000 person-years.9 In addition, the three populations have similar age distributions and life expectancies and have publicly funded healthcare systems with a well-organised cancer care and treatment infrastructure available and accessible across the population.10 As a consequence, a further quantification of the differences in colorectal cancer survival across the three countries could be highly informative.
A number of previous studies have presented differences between countries as either cumulative relative survival (usually at 5 years) or relative risk (RR) of increased mortality.7 This can be misleading when the underlying risk is low as even a moderately large RR may have little impact on the number of deaths. This is particularly important in colorectal cancer as it is known that eventually the mortality rate of those diagnosed with the disease returns to the same level as that expected in the general population.11 For this reason we have concentrated on the estimation of absolute risks using the excess mortality associated with a diagnosis of cancer.
The aim of this study is to examine differences in the survival and excess death rates of patients diagnosed between 1996 and 2004 in Norway, Sweden and England by both age and duration of follow-up, and to further elucidate the English survival deficit.
Methods
All cases of colon cancer (ICD10 (International Classification of Diseases, 10th revision) C18) and rectal cancer (ICD10 C19 and C20) diagnosed in the period 1996–2004 were extracted from population-based cancer registries in England, Norway and Sweden. Cases that were diagnosed by death certificate only (DCO), had missing survival time data, negative survival time or a survival time of 0 days were excluded (table 1). This left a study population of 241 041, 29 513 and 46 025 individuals in England, Norway and Sweden, respectively.
Study population
Survival analyses were undertaken using methods described in previous studies comparing cancer survival between these three countries.12 13 Relative survival (using the period approach to obtain the most up to date estimates of survival focusing on the more recent follow-up period of 2001–200414) was calculated as the ratio of observed survival of the study population to its expected survival (determined from annual sex- and age-specific life tables for each of the three countries).15 16 Patients were informative for follow-up if they provided person-years in the period 2001–2004. This equated to 181 359, 23 407 and 36 953 individuals in England, Norway and Sweden, respectively.
Age standardisation of the relative survival rates used the weights of the International Cancer Survival Standard (ICSS) cancer patient population.17 To study differences between countries, the number of excess deaths per 100 person-years was calculated.
The number of excess deaths in each follow-up interval (0–3 months, 3 months–1 year, 1–2 years and 2–5 years) in each age group (0–49, 50–59, 60–69, 70–79 and ≥80 years) was estimated for each country—that is, the additional number of deaths per year over that expected in the general population. In addition, the number of avoidable deaths per year was calculated, which is the number of fewer deaths that would have occurred in England if the English patients with colorectal cancer had the same survival experience as their Norwegian counterparts using the methods previously described by Møller et al.13 Relative survival was performed using the ‘strs’ function in Stata,18 and other analyses with the R-statistical software package.19
Results
Table 2 shows the cumulative 5-year relative survival estimates by age for colon and rectal cancer in the three countries. Overall, relative survival decreased with age and was lowest in those aged ≥80 at diagnosis, with the exception of Swedish patients with colorectal cancer for whom the relative survival was similar, and at a high level, in all age groups. The survival of English patients with colon and rectal cancer was lowest across all age groups.
Age distribution and the 5 year cumulative relative survival for patients with colon and rectal cancer, with 95% CIs in parentheses, in England, Norway and Sweden
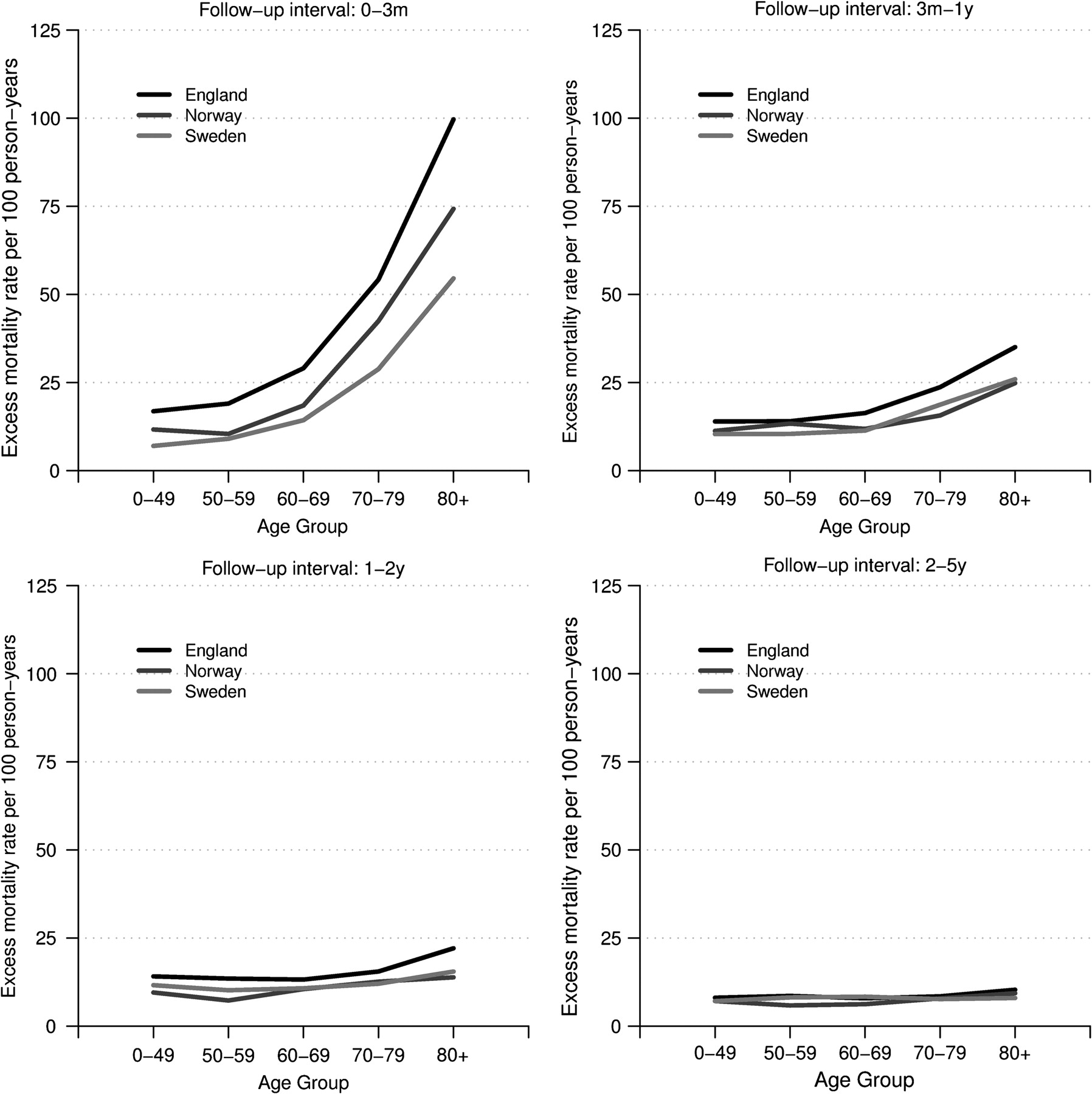
In all three countries, the excess mortality among patients with colorectal cancer was highest in the first 3 months after diagnosis and was most evident in the oldest age groups (figure 1). The level of excess mortality varied, however, between the countries. Excess mortality was greatest in England and was at its maximum in the first 3 months after diagnosis and in the oldest patients. For example, for individuals aged ≥80 years at diagnosis, the excess mortality was 150 deaths per 100 person-years in England compared with 60 deaths per 100 person-years in Sweden. There was also variation in the excess mortality rate between the three countries in the 3 months–1 year follow-up period, with rates being higher in England. In subsequent follow-up periods, intercountry differences were negligible.

Excess death rates among patients with colon cancer in England, Norway and Sweden (2001–2004) by age at diagnosis and period of follow-up.
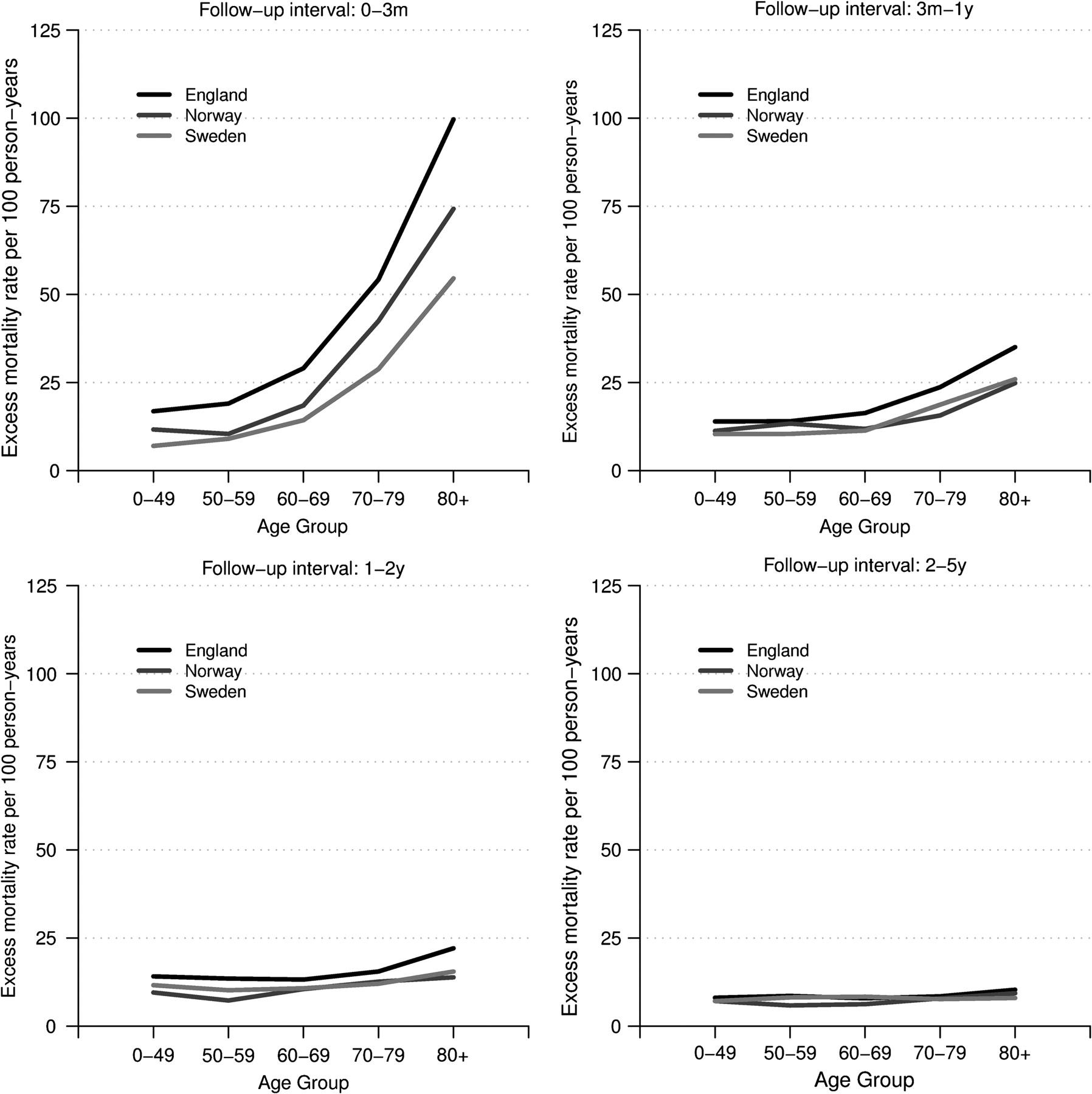
Although excess mortality was slightly lower, its distribution was similar for patients with rectal cancer (figure 2). Again, in all three countries the excess mortality was greatest in the first 3 months after diagnosis, in the oldest patients and in the English population. In contrast to the colon cancer population, however, the excess mortality rate remained higher in the English population for up to 2 years of follow-up.
{kind=link}
{kind=link}
Excess death rates among patients with rectal cancer in England, Norway and Sweden (2001–2004) by age at diagnosis and period of follow-up.
The annual numbers of excess deaths per year within the patients with colon and rectal cancer of each country across each of the follow-up periods are shown in tables 3 and 4. Within the English study population there were 6534 and 3895 excess deaths per year at 5 years postdiagnosis in patients with colon and rectal cancer, respectively. However, if the death rates of patients with colorectal cancer in Norway could have been attained in the English population, then 890 (13.6%) of these excess deaths in the colon cancer population could have been avoided and 654 (16.8%) avoided in the rectal cancer population. For colon cancer, almost all of these avoidable deaths occurred within the first 3 months after diagnosis. In contrast, the excess mortality of rectal cancer persisted up to 2 years after diagnosis.
Annual excess deaths per year in patients with colorectal cancer versus expectation based on national life tables
Annual avoidable deaths per year in English patients with colorectal cancer versus expectation based on patients with colorectal cancer in Norway
In the follow-up period of 1–2 years and 3–5 years negative avoidable deaths were calculated (table 4). These have been observed as the avoidable deaths calculation is based on deaths from all causes and as, eventually, everyone will die then any positive early avoidable deaths will eventually be counteracted by negative avoidable deaths at later time points. In this case these deaths occur within 5 years of follow-up.
Discussion
In all three countries patients with colorectal cancer were subject to higher rates of mortality than the general population. This excess mortality was most evident within the first 3 months after diagnosis and for the oldest patients. There was also variation between the countries, with the English population experiencing lower survival proportions. Among patients with colon cancer this was primarily due to a high number of excess deaths within the first 3 months after diagnosis. For the rectal cancer population excess deaths were greatest in the first 3 months after diagnosis but remained elevated until 2 years of follow-up elapsed.
Other studies have also demonstrated survival differences between English and Nordic patients with colorectal cancer that were age dependent and greatest immediately after diagnosis.7 8 There is a growing body of evidence that English survival outcomes are truly inferior to those of its economic neighbours, and such findings have resulted in significant efforts being made to reduce the differences.2 3 To address the problem fully, however, the underlying causes must be understood, and there are a number of potential explanations for these observations that are discussed below.
First, the survival variations may have arisen inadvertently through fundamental intercountry differences in the collection of cancer registry data. A number of problems may exist. For example, in contrast to cancer registries in England and Norway, Swedish registries do not make use of death certificates in the primary case ascertainment of tumours,20 21 and this introduces a bias towards higher cancer survival estimates in Sweden. DCO registrations were, however, excluded from the analyses to minimise the impact of this. Furthermore, a common explanation for a case being registered via death certificate is that no active treatment was given to the individual and, as a result, no pathology or treatment reports were sent to the registry that would have enabled earlier identification. Given that such individuals have a poor prognosis, the exclusion of these cases will have served to diminish the survival differences observed. In addition, cancer registries which use death certificates as a registration source attempt to trace the medical records of such individuals prior to their death to determine if they had had a diagnosis of cancer made prior to their death. Such cases are often called death certificate-initiated registrations and are often of a poorer prognosis than the general cancer population. As such, their inclusion in the Norwegian and English data sets but absence from the Swedish data set could, potentially, have influenced the observed results. The proportion of cases registered in this way is, however, very low and so is unlikely to account entirely for the survival differences observed.
The reliability of UK cancer survival statistics and cancer registration has recently been called into question.22 Incomplete registration of cancers (especially of the good prognosis cases) and incorrect allocation of dates of diagnosis (relating to disease recurrence rather than original presentation) have been suggested to account for the low UK survival rates observed. If this is true, then the survival differences observed in this study may not be real but due simply to differences in data collection practices. Two recent studies provide evidence to counter these arguments. First, work using an identical methodology to that employed in this study, but comparing survival across socio-economic groups in England rather than between countries, found a similar effect (Møller H, personal communication 2010). There was a survival difference between individuals residing in the lowest and highest socio-economically deprived areas, but the differences were greatest in the oldest people and in the first months after diagnosis. The methods employed by each of the English registries are reasonably consistent across the country and so differences in registration practice cannot account for the survival differences observed. In addition, another study (Møller H, personal communication 2010) investigated the impact of potentially incorrect dates of diagnosis in registries by linking registry data to Hospital Episode Statistics and, if a patient had been in hospital prior to the date of diagnosis in the registry, using this to calculate survival times. This demonstrated minimal impact on cancer survival and would again suggest that the English estimates are robust.
Another problem related to data collection is that, in the data from Norway an excess of cases had the date of diagnosis coded as the first day of the month, indicating that some cancers whose day of diagnosis was unknown had been assigned to this date. Sensitivity analyses were undertaken, therefore, where all Norwegian cases with a date of diagnosis on the first day of the month were recoded to the middle of the month (data not shown). This had no discernible impact on the results.
It is also possible that the observed variation in survival could be explained by the existence of fundamental differences in the disease and patient characteristics of the populations. There is reasonable evidence to demonstrate that differences exist in the stage distribution of tumours between countries, and so it is possible that this may account for some of the observed variation in survival.4 5 13 23 The current lack of population-based staging information between these countries has, however, hindered a more complete investigation of the effect of stage on survival. It remains a credible argument, however, that a higher proportion of the English colorectal cancer population present with advanced disease than their Norwegian or Swedish counterparts, resulting in English excess death rates being significantly higher in the first 3 months after diagnosis.
Likewise the presence of co-morbid disease may have a detrimental effect on outcomes, as this can both preclude radical treatment and increase its risk. If the English population possessed more co-morbid disease at diagnosis, then this could, again, account for their initially poorer prognosis. Unfortunately no direct evidence is available to enable comparison of levels of co-morbid disease across the countries, making it difficult to quantify the existence or influence of any such differences. General population life expectancy is, however, comparable across the three countries, which may suggest that levels of co-morbidity were similar.24
If differences in the stage of disease and co-morbidity at presentation did exist, then this may translate to intercountry differences in surgical practice and outcomes. For example, overall resection rates may be lower and emergency presentation and postoperative mortality rates higher in countries with higher staged or less healthy patients at diagnosis. Evidence suggests that surgical intervention rates may be higher in Norway and Sweden than in England, which would support the argument that a higher proportion of the English patients presented with advanced disease.25–27 In contrast, however, the incidence of emergency surgery is similar (at ∼20–25%) in all three countries, and this suggests that similar levels of disease presenting with acute abdominal symptoms exist across the populations.12 27–30 Further evidence is required before it can be determined conclusively whether differences in the extent of disease and co-morbidity at diagnosis between the countries can fully account for the survival differences observed.
A final possible explanation for the survival differences observed pertains to the fact that there may be variation in the quality of supportive medical care that older patients receive in each country which directly influences outcome. For example, the relatively higher number of deaths in the initial months after diagnosis in England may be indicative of suboptimal perioperative care.31 Surgery is the primary treatment modality for colorectal cancer and there is good evidence to suggest that postoperative mortality rates vary among providers.25 30 31 It is possible, therefore, that higher rates of postoperative deaths in England compared with Norway or Sweden could contribute to the poorer survival in the first 3 months after diagnosis. It is, however, very difficult to explore this further as robust comparable surgical information does not yet exist to enable intercountry comparisons. If Scandinavian health systems are, however, more successful at ensuring their patients survive the postoperative period then it is important to learn from them and to improve the English system accordingly.
The intercountry differences in rectal cancer survival could, potentially, also be partially explained by variations in surgical and oncological practice. Incomplete surgical excision of rectal tumours is associated with local recurrence of the disease which, generally, proves fatal. Total mesorectal excision (TME) has been shown to increase the likelihood of a complete excision, reduce local recurrence and, consequently, improve survival.32 33 This technique was generally adopted by all surgeons in Sweden and Norway in advance of the UK,26 34 and its use could have translated to an improvement in survival in Scandinavia over the time period of this study. Of those patients who develop local recurrence, 75% do so within the first 2 years after diagnosis and, as a consequence, higher rates of local recurrence in England compared with Scandinavia could, potentially, contribute to the higher excess mortality observed over this follow-up period.
Other management factors may also be influential. Over the course of the study period several randomised trials were published whose results have directly influenced the management of this disease, and there may have been intercountry differences in the adoption of these treatments. For example, over the study period, evidence came from a Swedish study that preoperative radiotherapy was advantageous in the management of rectal cancer,35 and it is possible that more patients in Sweden received this treatment than in Norway or England.25 26 It is possible that other treatments (such as chemotherapy or operative method) or organisational factors (such as delays in access to treatment or specialisation of surgeons) may also have been different across the three countries. As yet, however, there are no population-based data sets available in each of the participating countries that would enable a full quantification of the influence of such factors on survival. Future development and comparison of such data sets could, however, enable a greater understanding of the causes of the survival differences and help in the formulation of strategies to address them.
Over the period studied there were no population-based co-ordinated screening programmes in any of the countries considered. As such, differences in screening practice will not account for the survival differences observed. In 2006 a national population-based screening programme began roll-out in England and the scheme attained national coverage earlier in 2010. Early analyses suggest that this screening programme is detecting tumours at a much earlier stage of disease than occurs in the symptomatic population.36 As a result this is likely to lead to a significant improvement in colorectal cancer survival in England. Screening programmes are also planned or under discussion in Sweden and Norway. Detecting disease at an early stage is the best way to maximise survival rates, and so the implementation of these plans is likely to have a major impact on future survival rates.
Whatever the cause of these survival differences between the Scandinavian and English populations, they represent important mortality differences that are potentially avoidable. This study suggests that if the excess death rate of Norway were to apply in the English colorectal cancer population then 1544 deaths per annum would have been avoided. It is probable that all the inter-related factors of co-morbidity, extent of disease at diagnosis and quality of care contribute to the observed survival deficit, but more evidence is required before the influence of each of these potential factors can be fully quantified. Whatever the cause, it is apparent that a larger proportion of the population in England present with rapidly fatal disease, especially in the older age groups. This phenomenon has now been observed both internationally across a number of other cancer sites,12 13 and also between socio-economic groups in England.23 Further robust and comparable data regarding co-morbidity and stage at presentation are now required to ensure appropriate public health interventions that address the poorer short-term survival (such as screening or increasing awareness of symptoms in primary care) of patients with colorectal cancer in England. It is hoped that a better understanding of these factors may be gained as a result of ongoing projects such as the International Cancer Benchmarking Partnership.37
References
Footnotes
This paper is a contribution from the National Cancer Intelligence Network (http://www.ukacr.org/; http://www.ncin.org.uk/) and is based on the information collected and quality assured by the regional cancer registries in England, the Cancer Registry of Norway and the Swedish Cancer Registry.
Funding Cancer Research UK Bobby Moore Fund.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.