Article Text

Abstract
Objective Recently, the authors demonstrated altered gene expression in the jejunal mucosa of diarrhoea-predominant irritable bowel syndrome patients (IBS-D); specifically, the authors showed that genes related to mast cells and the intercellular apical junction complex (AJC) were expressed differently than in healthy subjects. The aim of the authors here was to determine whether these alterations are associated with structural abnormalities in AJC and their relationship with mast cell activation and IBS-D clinical manifestations.
Design A clinical assessment and a jejunal biopsy were obtained in IBS-D patients (n=45) and healthy subjects (n=30). Mucosal mast cell number and activation were determined by quantifying CD117+ cells/hpf and tryptase expression, respectively. Expression and distribution of AJC specific proteins were evaluated by western blot and confocal microscopy. AJC ultrastructure was assessed by transmission electron microscopy.
Results Compared with healthy subjects, IBS-D patients exhibited: (a) increased mast cell counts and activation; (b) increased protein expression of claudin-2, reduced occludin phosphorylation and enhanced redistribution from the membrane to the cytoplasm; and (c) increased myosin kinase expression, reduced myosin phosphatase and, consequently, enhanced phosphorylation of myosin. These molecular alterations were associated with ultrastructural abnormalities at the AJC, specifically, perijunctional cytoskeleton condensation and enlarged apical intercellular distance. Moreover, AJC structural alterations positively correlated both with mast cell activation and clinical symptoms.
Conclusion The jejunal mucosa of IBS-D patients displays disrupted apical junctional complex integrity associated with mast cell activation and clinical manifestations. These results provide evidence for the organic nature of IBS-D, a heretofore model disease of functional gastrointestinal disorders.
- IBS-D
- intestinal permeability
- tight junction signalling
- mucosal mast cells
- brain–gut interaction
- intestinal mast cells
- gene expression
- gut inflammation
- intestinal barrier function
- stress
- small bowel disease
- serotonin
- neurogastroenterology
- neural–immune interactions
- motility disorders
- anorectal function
- visceral sensitivity
- gastrointestinal motility
- gas physiology
- functional bowel disorder
- antibacterial mucosal immunity
- enteric bacterial microflora
- gut immunology
Statistics from Altmetric.com
- IBS-D
- intestinal permeability
- tight junction signalling
- mucosal mast cells
- brain–gut interaction
- intestinal mast cells
- gene expression
- gut inflammation
- intestinal barrier function
- stress
- small bowel disease
- serotonin
- neurogastroenterology
- neural–immune interactions
- motility disorders
- anorectal function
- visceral sensitivity
- gastrointestinal motility
- gas physiology
- functional bowel disorder
- antibacterial mucosal immunity
- enteric bacterial microflora
- gut immunology
Significance of this study
What is already known about this subject?
-
Low-grade inflammation and altered intestinal permeability are frequently observed in diarrhoea-predominant irritable bowel syndrome (IBS-D) patients.
-
Differential gene expression patterns of jejunal biopsies from IBS-D patients have been linked to pathways involved in mast cell activation, intestinal permeability and tight junction signalling.
-
Barrier dysfunction in IBS has been linked to the downregulation and redistribution of several tight junction-related proteins.
What are the new findings?
-
The jejunal mucosa of diarrhoea-predominant irritable bowel syndrome (IBS-D) patients shows alterations in expression and phosphorylation status of tight junction transmembrane proteins.
-
The jejunal mucosa of IBS-D patients shows ultrastructural abnormalities at the apical junctional complex; specifically, perijunctional cytoskeleton condensation and enlarged apical intercellular distance.
-
These molecular and ultrastructural alterations positively correlated both with mast cell activation and clinical symptoms.
How might it impact on clinical practice in the foreseeable future?
-
Treatment strategies addressed to restore epithelial barrier functional homeostasis may benefit clinical response in these patients.
Introduction
The loss of molecular and functional integrity of the intestinal epithelial barrier allows increased antigenic penetration leading to activation of mucosal immune responses1 ,2 and contributing, thereby, to several gastrointestinal disorders such as the irritable bowel syndrome (IBS).3 Indeed, growing evidence suggests that diarrhoea-predominant IBS (IBS-D) may arise as the result of a combined process of low-grade mucosal inflammation, immune activation and barrier dysfunction.4–9 In these patients, the inflammatory infiltrate is dominated by increased populations of activated mast cells4 ,9–11 which release a wide range of neurotransmitters and other inflammatory mediators. Among all these mediators, tryptase seems particularly relevant as it can activate protease-activated receptor 2 on epithelial cells, resulting in modulation of tight junction (TJ) proteins and increases in permeability through paracellular pathways.12
Studies investigating the molecular basis of these abnormalities have largely focused on the colon,13–15 partly due to the easy access to distal areas of the gut. However, some data indicate that mucosal inflammation in IBS-D patients is not limited to the lower gut,4 ,16 and that increased intestinal permeability occurs along the whole intestine.6 Furthermore, several lines of evidence point to the small bowel as the site of origin of IBS symptoms.17–20 The general hypothesis of our research programme is that IBS-D is a disorder which primarily affects the small bowel and, hence, our studies focused on the jejunum.
In previous studies, we demonstrated increased number and activation of mast cells in a cohort of IBS-D patients (n=25) as compared with healthy subjects (n=23).11 We further observed significant differences in global gene expression in both groups, and TJ signalling pathways came out as the most significant canonical pathways associated with altered gene expression in the jejunal mucosa of IBS-D patients.11 Having shown this abnormal expression of genes related to TJs, we now hypothesised that these alterations are associated with structural abnormalities of the apical junction complex (AJC) at the intestinal mucosal barrier. The relevance of this hypothesis is that it questions the paradigmatic functional nature of this disorder. In the first place, we wished to confirm in a significantly larger cohort of patients and controls the mast cell abnormalities and their correlation with symptoms previously observed. The original aims of the present study were to determine in this cohort: (1) the molecular mechanisms of AJC disassembly; (2) the impact of these molecular alterations on AJC ultrastructure; and (3) whether AJC disassembly is related to mast cell activation and IBS-D clinical manifestations.
Methods
Participants
Naive patients (n=45) referred for the evaluation of IBS symptom who presented daily watery diarrhoea or mushy stools and meeting Rome II IBS-D criteria21 were prospectively recruited from the gastroenterology outpatient clinic. Healthy subjects (n=30) without gastrointestinal symptoms were recruited only by public advertising. Prior to entering the study, candidates were asked to fill out clinical questionnaires (to characterise the symptoms in patients and verify the lack of symptoms healthy subjects), and all underwent a battery of skin prick tests for 22 common food allergens (Leti SA, Barcelona, Spain) to exclude allergy. In all patients a broad biochemical and serological profile, including antitransglutaminase antibodies and thyroid hormones were determined. Previous history of acute gastroenteritis in relation to the initiation of IBS symptoms was specifically excluded. Moreover, reasonable exclusion of gastrointestinal comorbidities, such as microscopic colitis and celiac disease, was achieved by means of upper and lower fiberoptic and small bowel capsule endoscopy, abdominal sonography and barium studies, when considered pertinent. Other exclusion criteria for all participants were: regular use of medication or herbal preparation in the previous 3 months, active smoking, major psychiatric and organic diseases. The study protocol was approved by the Ethics Committee of the Hospital Vall d'Hebron. Written informed consent was obtained from each participant.
General procedures
Clinical evaluation
Using daily questionnaires over a 10-day period, the following parameters were recorded in all participants: (a) severity of abdominal pain by a 100-point visual analogue scale; (b) frequency of abdominal pain (number of days with pain); (c) stool frequency (day with maximum number of bowel movements); and (d) stool consistency assessed by the Bristol Stool Form Score22 (if more than one bowel movement per day, the Bristol Stool Form Score was averaged, and the grand mean over the 10-day period was calculated). Background stress over the last year was evaluated by the Modified Social Readjustment Scale of Holmes–Rahe.23
Jejunal biopsy
A single mucosal biopsy was obtained from the proximal jejunum (5 cm distal to the angle of Treitz) using a Watson's capsule as previously described.4 ,11 Tissue samples were immediately split into two similar pieces with a sterile scalpel. One fragment was fixed in formalin and embedded in paraffin for further microscopic examination (histology, immunohistochemistry and immunofluorescence). The other fragment was snap frozen in liquid nitrogen for protein isolation and western blot analysis or placed in RNAse free tubes containing 500 μl of RNA Later Solution (Ambion, Madrid, Spain) for RNA isolation and analysis by quantitative real-time PCR (Q-RT-PCR) (see Experimental design).
Experimental design and rationale
Clinical evaluation and jejunal biopsy were obtained at study entry in all participants. Analyses performed in each participant are detailed in supplementary table 1. Routine histology and immunohistochemistry to assess the number of mast cells and intraepithelial lymphocytes were performed in all participants (45 IBS-D patients and 30 healthy subjects). The following analyses were also performed in randomly selected subjects (see Statistical analysis below and supplementary table 1):
-
To evaluate mast cell activation, tryptase RNA and protein were analysed by Q-RT-PCR (17 IBS-D patients and 12 healthy subjects) and by western blot (seven IBS-D patients and seven healthy subjects), respectively.
-
To evaluate the expression of TJ transmembrane proteins, the protein was isolated and analysed by western blot analysis (seven IBS-D patients and seven healthy subjects).
-
To evaluate the mechanisms of AJC disassembly through modulation of cytoskeleton, protein expression of phosphorylated myosin light chain (pMLC), myosin light chain kinase (MLCK) and the catalytic subunit of myosin phosphatase (PP1cδ) was assessed by immunofluorescence (14 IBS-D patients and 14 healthy subjects) and western blot (seven IBS-D patients and seven healthy subjects).
-
To assess the impact of the above molecular alterations on AJC ultrastructure, tissue samples were analysed by transmission electron microscopy (TEM) (15 IBS-D patients and 10 healthy subjects).
Analytical procedures
Histology and immunohistochemistry
Tissue sections were processed for routine H&E staining to assess epithelial morphology. In addition, the number of mast cells was determined at ×400 magnification using antihuman c-kit (CD117) (Dako, Barcelona, Spain), as previously described.4 ,11 Specimens were blindly examined by one experienced pathologist (IT).
Immunofluorescence
Tissue sections were deparaffinised and hydrated following general procedures and blocked with Dako Blocking Solution (Dako, Barcelona, Spain) for 10 min followed by 60-min room temperature incubation in rabbit antihuman occludin (OCLN) polyclonal antibody (Invitrogen, Madrid, Spain), rabbit antihuman ppMLC or mouse antihuman pMLC (Cell Signaling Technologies, Danvers, Massachusetts, USA). Secondary antibodies were Alexa Fluor 594 goat antirabbit IgG and 488 goat antimouse IgG (Molecular Probes, Madrid, Spain). Nuclei were counterstained with 4',6-diamidino-2-phenylindole (DAPI) before mounting in Prolong antifade reagent (Molecular Probes). Negative control slides were set by exposing the serial sections under similar conditions but without the primary antibody. Images were acquired and quantified in a blinded manner using the FV-10-ASW Olympus software (Olympus, Barcelona, Spain), as previously described.11
Quantitative real-time PCR
Synthesis of cDNA was performed using 1 μg of total RNA with the High Capacity Reverse Transcription Reagents Kit (Applied Biosystems, Madrid, Spain). Q-RT-PCR was performed on an ABI PRISM® 7500 FAST Sequence Detection System (Applied Biosystems) using validated TaqMan Gene Expression Assays and the human 18S subunit ribosomal RNA gene as an endogenous control (Applied Biosystems), as previously described.11
Protein isolation and western blotting
Samples were homogenised in the FastPrep mixer (MP Biomedicals, Solon, Ohio, USA) in T-PER buffer and protease and phosphatase inhibitor cocktail (Invitrogen), following the manufacturer's recommendations. Insoluble material was removed by centrifugation (350 g, 5 min, 4°C) and the supernatant was sonicated four times for 10 s at 4°C. Protein concentration was determined by Pierce bicinchoninic acid assay (Pierce, Madrid, Spain). Equal amounts of protein were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) and transferred to a poly(vinylidene difluoride) membrane. Primary antibodies and dilutions used are listed in supplementary table 2. Peroxidase-conjugated goat antirabbit IgG or goat antimouse IgG (Pierce) and the chemiluminescence detection system SuperSignal West Femto (Thermo Scientific, Madrid, Spain) were used to detect bound antibodies. All blots were probed with mouse antihuman β-actin (Sigma-Aldrich, Madrid, Spain) as a protein loading control. Densitometric comparison was carried out on the same immunoblot using the ImageJ software (National Institutes of Health; http://rsb.info.nih.gov/ij/).
Transmission electron microscopy
Samples were fixed with 2.5% glutaraldehyde and 2% paraformaldehyde and processed for TEM following standard procedures. Ultra-thin sections were mounted on copper grids, contrasted with standard uranyle acetate and lead citrate double-staining, and observed in a Jeol JEM-1400 (Jeol LTD, Tokyo, Japan) transmission electron microscope equipped with a Gatan Ultrascan ES1000 CCD camera. To evaluate changes in AJC ultrastructure, only sections with longitudinally-oriented microvilli were examined in each sample. Examinations were performed independently by two investigators (CM and MV) in a blinded manner on a minimum of 50 junctions per subject in non-overlapping fields. The AJC architecture was evaluated by measuring: (a) the width of intercellular spaces at the largest point; (b) the number of dilated junctions (>20 nm);24 ,25 and (c) the number of junctions with increased perijunctional cytoskeleton condensation (patchy areas distinctively darker than the surrounding cytoplasm and completely blurring the intercellular membranes).26
Statistical analysis
Randomisation of patients for the different analysis was performed using a standard random number generator: a linear congruential generator was used to generate uniform random values, followed by a transformation to obtain integer values in a set with the same size as the number of patients.
Normality of data distribution was tested by the Komolgorov–Smirnov test. Normal parametric data are expressed as median (range), and otherwise by mean±SD. Normally distributed parametric data were compared by the unpaired Student t test (two-tailed); otherwise, the Mann–Whitney U test was used. p Values were adjusted to obtain strong control over the ‘false discovery rate’ using the Benjamini and Hochberg method.27 Relationships between clinical variables and gene or protein expression were assessed by Spearman's ρ correlation. Two-way ANOVA was performed to assess the potential influence of gender on gene expression in IBS-D patients and healthy subjects. Statistical analysis was performed using GraphPad Prism 5.0 software (GraphPad Software Inc., La Jolla, California, USA).
Results
Study population
No significant differences in age were detected between IBS-D patients and healthy subjects (p=0.24). IBS-D patients exhibited higher stress levels than healthy subjects (table 1). Other demographic and clinical characteristics of the participants are shown in table 1 and supplementary table 3. The clinical characteristics of the patients selected for the different analyses (age, stress levels, abdominal pain and stool frequency and consistency) did not differ from the remainder (p>0.11 for all).
Clinical and demographic characteristics of participants
Mast cell hyperplasia and activation
As in our previous study,11 IBS-D patients showed increased mast cell counts (IBS-D: 26.2±11.1; healthy subjects: 17.2±8.8 CD117+ cells/hpf; p=0.0004) and tryptase mRNA (IBS-D: 1.9±0.5; healthy subjects: 1.1±0.2 fold; p<0.0001). The present study further showed that tryptase protein was overexpressed in patients (IBS-D: 1.4±0.3; healthy subjects: 1.0±0.2 fold; p=0.03).
Expression and distribution of transmembrane TJ proteins
Our previous study11 found several genes involved in the TJ signalling pathway differentially expressed in IBS-D. In order to further assess TJ dysregulation, the expression of transmembrane TJ proteins was now analysed. No differences in protein expression of claudins (CLDNs) 1, 3 and 4 were observed, while CLDN2 was significantly upregulated in IBS-D (figure 1). Protein expression of OCLN was similar in both groups; however, OCLN phosphorylation (p-OCLN) (which is identified by the upper 85 KDa band) was significantly reduced in IBS-D (figure 1). Of note, p-OCLN correlated with the expression of CLDN3 (r=0.84, p=0.0001) and CLDN4 (r=0.73, p=0.003).

Transmembrane tight junction protein expression in jejunal mucosa. CLDN and OCLN protein expression was measured by western blot in seven IBS-D patients and seven healthy subjects (left panel). Protein fold-change (right panel) was calculated for each sample with reference to the average of the target protein to β-actin ratio of the healthy group. Intergroup comparisons were performed by the Mann–Whitney U test (significant p values shown). CLDN, claudin; IBS-D, diarrhoea-predominant irritable bowel syndrome; OCLN, occludin.
As the phosphorylation status of OCLN has been linked to its distribution in epithelial cells,28 we assessed OCLN staining by confocal immunofluorescence. IBS-D samples displayed significantly increased staining of OCLN in the cytoplasm of jejunal enterocytes, suggesting intensive internalisation of this protein, as opposed to the healthy group where OCLN was predominantly located in the TJ (figure 2).

OCLN distribution in jejunal mucosa. Upper panels show representative micrographs of jejunal epithelium (high-power field, ×1000) with OCLN labelled by immunofluorescence in red and nuclear labelling with DAPI in blue. Lower panels show quantitative analyses of fluorescence intensity performed blindly using the FV-10-ASW Olympus software. Data are average of fluorescence intensity in 10 non-overlapping fields per subject. Intergroup comparisons were performed by the unpaired Student t test (significant p values shown). IBS-D, diarrhoea-predominant irritable bowel syndrome; OCLN, occludin; TJ, tight junction.
Phosphorylation of MLC
In an attempt to identify mechanisms regulating AJC function, we evaluated MLC phosphorylation. IBS-D patients showed a significant increase in MLC phosphorylation at Ser19 (pMLC) (figure 3), which has been related to the contraction of the acto-myosin cytoskeleton and disassembly of TJ.1 ,2 By contrast, MLC phosphorylation at Thr18+Ser19 (ppMLC) remained unchanged (figure 3), suggesting that de novo TJ assembly is not impaired in IBS-D.
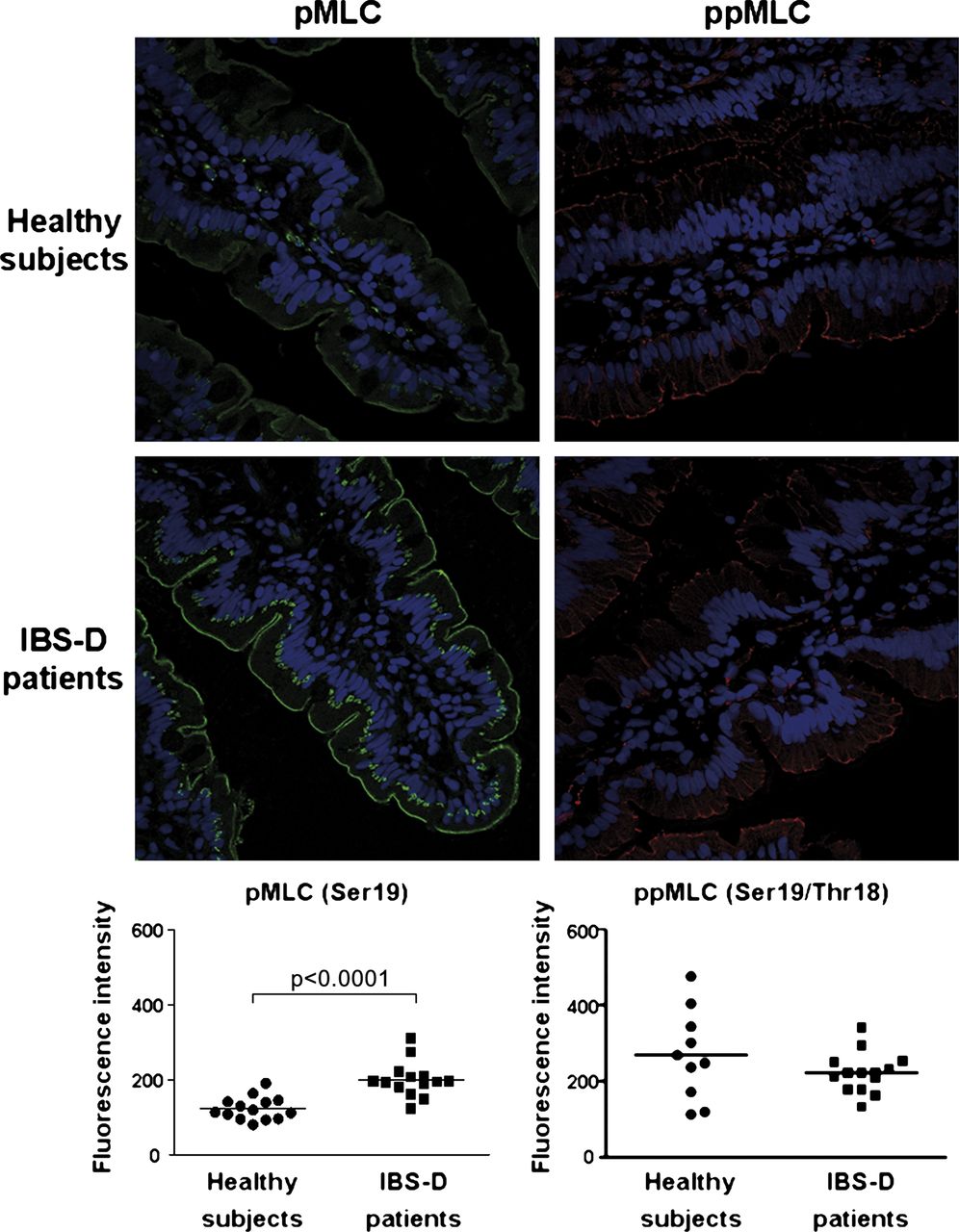
MLC phosphorylation in jejunal mucosa. Upper panels show representative micrographs of jejunal epithelium (high-power field, ×400) with Ser19-phosphorylated MLC (pMLC) labelled by immunofluorescence in green, Ser19/Thr18-phosphorylated MLC (ppMLC) in red and nuclear labelling with DAPI in blue. Lower panels show quantitative analyses of fluorescence intensity performed blindly using the FV-10-ASW Olympus software. Data are average of fluorescence intensity in 10 non-overlapping fields per subject. Intergroup comparisons were performed by the unpaired Student t test (significant p value shown). IBS-D, diarrhoea-predominant irritable bowel syndrome; MLC, myosin light chain.
In concordance with the increased pMLC, IBS-D showed increased expression of MLCK (4.9±3.7 vs 1.0±0.8 fold-change in healthy subjects, p=0.01), while PP1cδ was decreased (IBS-D: 0.7±0.2 vs1.0±0.2 fold-change in healthy subjects, p=0.02).
Ultrastructural alterations at the apical junctions
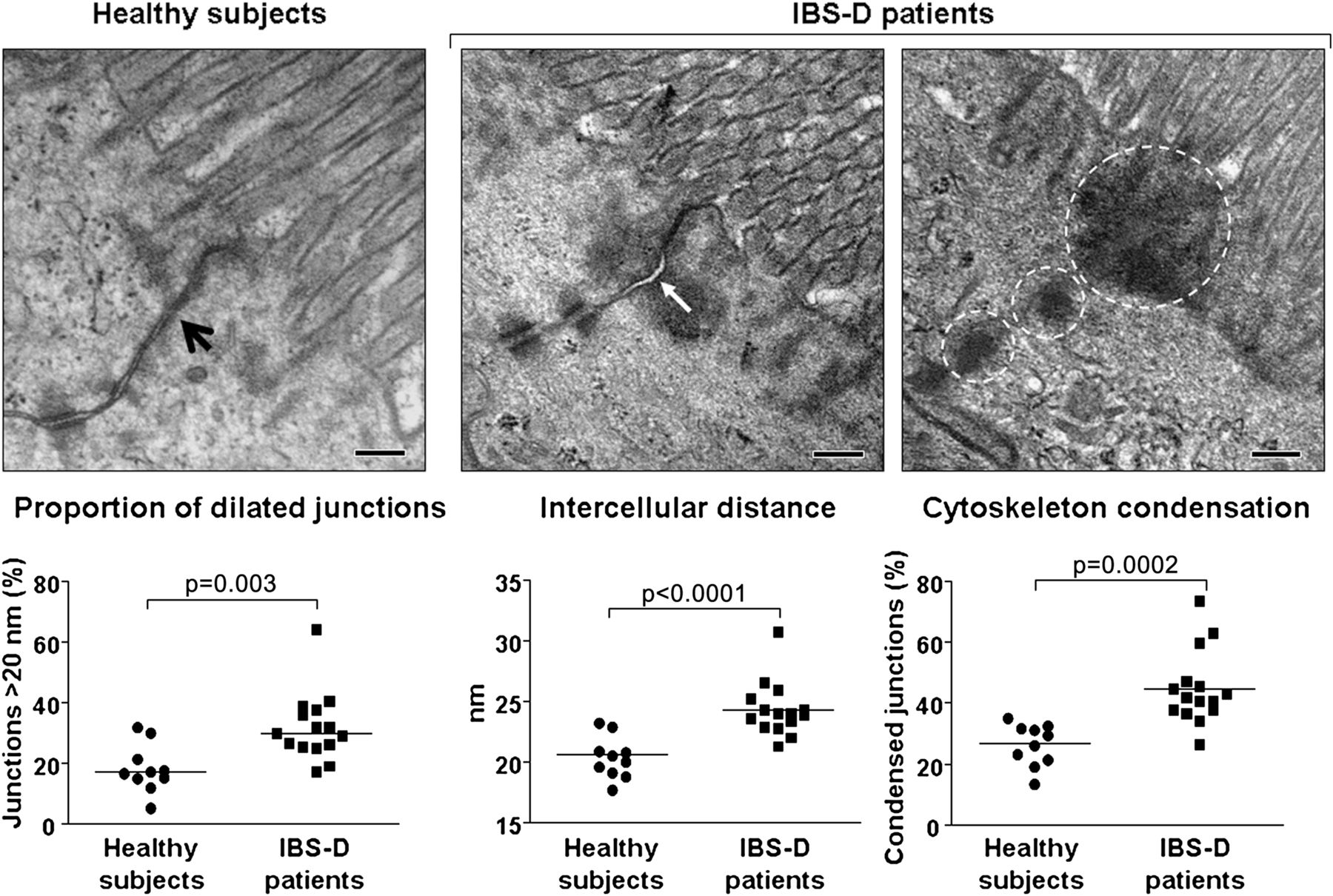
As previously described,11 routine processing of jejunal samples for H&E staining in the present study revealed no differences in epithelial architecture between IBS-D patients and healthy subjects. Using TEM, we were now able to demonstrate that the molecular alterations described above were associated with ultrastructural changes of intercellular junctions featuring a real disassembly (figure 4). Indeed, compared with healthy subjects, IBS-D patients exhibited a larger apical intercellular distance with a higher proportion of dilated (>20 nm) junctions (figure 4). Patients also had a higher percentage of junctions with perijunctional cytoskeleton condensation (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ultrastructure of apical junctional complex in the jejunal mucosa. Upper panels show representative micrographs of the jejunal epithelium (original magnification ×60 000). Note intercellular junctions in healthy subjects (black arrow, in upper left panel), widening of the intercellular space (white arrow, in upper middle panel) and perijunctional cytoskeleton condensation (dashed circles, in upper right panel) in diarrhoea-predominant irritable bowel syndrome (IBS-D) patients. The maximum width of intercellular spaces (at the largest point) was measured in a minimum of 50 junctions per subject in non-overlapping fields. The proportion of dilated junctions (>20 nm) per subject is shown in lower left panel and the average intercellular distance per subject in lower middle panel. The proportion in each subject of junctions with electron-dense material around the apical junctional complex is shown in lower right panel. Intergroup comparisons were performed by the unpaired Student t test (significant p values shown).
Correlation of molecular and ultrastructural AJC alterations with IBS-D clinical manifestations
As previously observed,11 mast cell activation, measured by tryptase mRNA expression, correlated with stool frequency and consistency in IBS-D patients (table 2), whereas their correlation with mast cell number was poor, suggesting that mast cell activation rather than number influences bowel habit. In the present study, we further demonstrated that tryptase protein expression, the end result of mast cell activation, also exhibited good correlation with bowel habit (table 2). Furthermore, tryptase protein expression correlated with AJC impairment measured by CLDN2 protein overexpression (r=0.76, p=0.002) and by increased OCLN cytoplasmic staining (r=0.75, p=0.003). Conversely, AJC impairment correlated with stool frequency and consistency (table 2). Ultrastructural AJC alterations correlated with abnormal bowel habit, as well as with abdominal pain intensity (table 2).
Clinical–biological correlations in the jejunal mucosa of IBS-D patients and healthy subjects
Correlation of mast cell-related variables and AJC alterations with gender and stress levels
To assess the potential influence of gender on mast cell infiltration/activation and on AJC alterations, we included gender as a variable in the analysis and did not find significant differences in any of the parameters evaluated (table 3).
Influence of gender on mast cell and AJC-related variables (two-way ANOVA)
To assess the influence of basal stress levels on biological parameters, we applied the Spearman ρ correlation to pooled data of patients and healthy subjects. Stress level was correlated with increased mast cell activation, measured by tryptase protein expression (r=0.53, p=0.05). However, no significant association between basal stress and the other biological parameters measured was detected, including mast cell counts (r=0.12, p=0.33), molecular alterations in TJ-related proteins (r<0.27, p>0.35 for all) and ultrastructural AJC alterations (r<0.32, p>0.12 for all).
Discussion
For the first time, we demonstrated structural abnormalities in the jejunal mucosa of IBS-D patients, which suggests that this is an organic rather than a functional disorder. Indeed, in contrast to healthy subjects, IBS-D patients exhibited disrupted architecture of the apical junctional complex, which was associated with mast cell activation and IBS symptoms.
Our research programme envisions the mast cell leading to disruption of intestinal barrier function as a pivotal element in IBS pathophysiology, as we have demonstrated mast cell hyperplasia and activation in the jejunum of IBS-D patients.4 ,11 Furthermore, in the present as well as in previous studies, mast cell activation correlated with patients' symptoms.11 Other studies showed increased numbers of mast cells in the duodenum16 ,17 and colon9 ,10 ,29 of IBS patients and, furthermore, mast cell activation has been implicated in the modulation of paracellular permeability through the release of several mediators, including cytokines and specific proteases.30 ,31
Evaluating global gene expression profiles in the jejunal mucosa of IBS-D patients and healthy subjects, we previously found a series of differentially expressed genes associated with mast cell biology, intestinal permeability and the AJC signalling pathway.11 In light of these results, the current study focused on the core proteins and ultrastructure of AJC. Barrier function in epithelial cells is regulated by the intercellular AJC in which TJ is the major constituent.32 The TJ transmembrane proteins, CLDNs and OCLN, compose the structural core of the TJ and are associated with the cytoskeleton, mainly composed of actin and myosin, through the scaffolding proteins zonula ocludens (ZO). This association with the perijunctional cytoskeleton is crucial for the dynamic regulation of paracellular permeability.2 Extending our previous results on gene expression, we now demonstrate increased CLDN2 protein expression and a trend towards decreased expression of CLDN3 and CLDN4, without detectable changes in CLDN1, in the jejunum of IBS-D patients. CLDN2 has been related to cation-selective channel activity and increased permeability,33 whereas CLDN1, 3 and 4 strengthen the barrier and reduce permeability through the paracellular space.34 The net alteration in the CLDN family of proteins detected in our study would lead to an increase in intestinal permeability. Indeed, a previous study in IBS-D patients showed increased small bowel permeability.6 Moreover, recent studies in the colonic mucosa of IBS patients have shown altered expression and cellular distribution of TJ-related proteins, specifically, downregulation of ZO-17 and OCLN14 ,35 and redistribution of CLDN1.35
Besides protein expression, specific phosphorylation of transmembrane and cytoskeleton proteins is also crucial for the assembly and maintenance of AJC integrity.2 ,36 When separated by SDS-PAGE, OCLN resolves into two bands of 65 and 85 KDa. The 85 KDa band represents ser/thr-phosphorylated OCLN28 ,37 that selectively concentrates at the TJ, while the 65 KDa weight band represents non-phosphorylated or less phosphorylated OCLN and is localised in the cytoplasm.28 No differences in global OCLN protein expression were found; however, our study is unique in reporting a reduction in the 85 KDa band, and a consequent redistribution of OCLN from the membrane into the cytoplasm, as has been identified in the colonic mucosa of IBS-D patients.35 Phosporylation and internalisation of OCLN have been shown to disturb the integrity of the AJC, leading therefore to increased epithelial permeability.38 Cytoskeleton contraction involves enhanced phosphorylation of MLC. We found both increased expression of the enzyme that catalyses MLC phosphorylation (MLCK) and reduced expression of the counteracting enzyme that catalyses dephosphorylation (PP1cδ). As a logical consequence of this enzymatic environment, we also found increased MLC phosphorylation. This is a crucial finding since cytoskeleton phosphorylation/contraction has been related to AJC disassembly and barrier disruption.39 ,40 In line with our results, MLCK-dependent phosphorylation of MLC has been reported to be the mechanism responsible for increasing intestinal permeability in the colon of mice infused with colonic supernatants from IBS patients.41
These findings fit well with the ultrastructural alterations found by TEM in the present study. Indeed, the electron-dense material observed around the AJC in IBS-D samples may represent the contraction of the perijunctional cytoskeleton.41 Another remarkable finding of this study was the significant increase in the paracellular space between adjacent enterocytes in the jejunum of IBS-D patients that may be the result of AJC disassembly and failure to maintain the tightness of the epithelial barrier. The significant correlation of regulatory and structural alterations with clinical parameters supports the hypothesis that AJC disassembly may play a key role in IBS-D pathophysiology; however, we acknowledge that these correlations have to be interpreted with caution as long as the whole spectrum of IBS has not been investigated.
The results presented in this study point at the mast cell as a pivotal element in the physiopathology of IBS. Indeed, mast cell activation, rather than their number, could explain the AJC alterations observed in this study. In principle, the opposite explanation could be equally possible, which is that increased permeability leads to a more general mast cell activation and hyperplasia. However, previous studies in acute stress models observed both mast cell activation and increased intestinal permeability, and the latter was prevented by mast cell stabilisers.42 ,43
We wish to acknowledge the relatively small sample size included in the different examinations in our study due to the limited tissue availability. To counterbalance this limitation, we strived at recruiting a homogeneous population by using stringent inclusion criteria, and we proved that each subset of subjects did not differ from the remainder, suggesting that the subgroups were representative of the whole study group. In this regard, we wish to highlight that the results of the various tests performed in different subsets of subjects are concordant and together support our working hypothesis. However, our results should be interpreted with caution especially regarding their translational relevance to the clinical practice, as we acknowledge that correlation is not causation and there are other models that could be constructed to explain our observations.
In summary, the results of the present and previous studies support the pathogenic model of IBS-D envisioning mast cell activation, alteration of TJ-related protein expression/distribution, ultrastructural damage of AJC and IBS disturbances as a chain of events. These results challenge the classical conception of IBS-D as a functional disorder and provide evidence of organicity in a significant proportion of patients.
Acknowledgments
The authors thank Milagros Gallart, Montse Casellas and Carmen Alastrue for help in sample analysis; Anna Aparici, Maria Teresa Casaus and Purificación Rodríguez for their invaluable assistance in the performance of jejunal biopsies; Dr Marta Valeri from the Scientific and Technical Support Unit of Vall d'Hebron Research Institute for excellent technical support in confocal microscopy; Servei de Microscopia of Universitat Autonoma de Barcelona for excellent technical support; Christine O'Hara for English editing of the manuscript; Dr. María Antolin for critically reviewing the manuscript; and Gloria Santaliestra for secretarial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Funding Supported in part by the Fondo de Investigación Sanitaria and CIBERehd, Instituto Carlos III, Subdirección General de Investigación Sanitaria, Ministerio de Ciencia e Innovación: CM08/00229 (B Lobo); CM05/00055 (L Ramos); CM10/00155 (M Pigrau); CM04/00019 (C Alonso); PI05/1423, EC07/90148 & PI/080940 (J Santos); CP10/00502 (M Vicario); Ministerio de Educación, Dirección General de Investigación: SAF 2009-07416 (F Azpiroz); Agència de Gestió d'Ajuts Universitaris i de Recerca, de la Generalitat de Catalunya: 2009 SGR 219 (F Azpiroz and J Santos); the International Foundation for Functional Gastrointestinal Disorders (2008 IFFGD) and the 2010 Rome Foundation Award (J Santos); and Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas: CB06/04/0021 (F Azpiroz and J Santos). CIBERehd is funded by the Instituto de Salud Carlos III.
-
Competing interests None.
-
Ethics approval Approval provided by the Ethics Committee of the Hospital Vall d'Hebron.
-
Provenance and peer review Not commissioned; externally peer reviewed.