Article Text

Abstract
Objective To develop a consensus on the classification, diagnosis and multidisciplinary treatment of perianal fistulising Crohn's disease (pCD), based on best available evidence.
Methods Based on a systematic literature review, statements were formed, discussed and approved in multiple rounds by the 20 working group participants. Consensus was defined as at least 80% agreement among voters. Evidence was assessed using the modified GRADE (Grading of Recommendations Assessment, Development, and Evaluation) criteria.
Results Highest diagnostic accuracy can only be established if a combination of modalities is used. Drainage of sepsis is always first line therapy before initiating immunosuppressive treatment. Mucosal healing is the goal in the presence of proctitis. Whereas antibiotics and thiopurines have a role as adjunctive treatments in pCD, anti-tumour necrosis factor (anti-TNF) is the current gold standard. The efficacy of infliximab is best documented although adalimumab and certolizumab pegol are moderately effective. Oral tacrolimus could be used in patients failing anti-TNF therapy. Definite surgical repair is only of consideration in the absence of luminal inflammation.
Conclusions Based on a multidisciplinary approach, items relevant for fistula management were identified and algorithms on diagnosis and treatment of pCD were developed.
- Crohn's Disease
- Gastrointestinal Fistulae
- IBD Clinical
- Infliximab
Statistics from Altmetric.com
Introduction
Penner and Crohn first described perianal fistulas as complications of Crohn's disease (CD) 75 years ago.1 Population based studies confirmed that perianal fistulas are the most common manifestation of fistulising CD, developing in 20% of Crohn's patients and recurring in approximately 30% of the cases.2 ,3 The cumulative incidence of perianal fistulising CD (pCD) is 12% after 1 year and this doubles 20 years after diagnosis.2 The risk of developing a fistula depends on disease location, being most frequent in colonic disease with rectal involvement.3 Perianal fistulas impose a significant burden on the patients. Unfortunately there are limitations in the available literature, making it challenging to develop an evidence based approach to pCD. The objective of the working group was to develop a consensus on the classification, diagnosis and treatment of pCD, based on best available evidence and expert opinion in order to offer guidance to clinicians.
Methods
Working group
The World Congress of Gastroenterology 2013 called for the development of state-of-the-art, evidence based views for designated areas of gastroenterology. An expert consensus group on pCD was formed and a literature review process (summarised in online supplementary figure S1) followed, covering all relevant papers and abstracts until March 2014. The search initially identified 4680 references. A selection process by the research committee members and additional references identified by manual search led to 247 retained articles.
Consensus process
Four areas of interest were identified: (1) classification and scoring, (2) diagnosis, (3) medical treatment, and (4) surgical management. For each of these areas the research committee drafted statements based on the systematic literature review and developed potential algorithms. These were discussed and revised by the group during their meetings. As a final step all participants voted on each statement, using definitions of agreement previously reported by Bitton et al.4 Consensus was a priori defined as at least 80% agreement. The modified GRADE (Grading of Recommendations Assessment, Development, and Evaluation) criteria were used to establish the strength of recommendations and the quality of evidence (see online supplementary table S1).5
Consensus statements
Section 1: Classification and scoring
Statement 1—General considerations for classification and scoring
1.1 A clinically useful classification of perianal fistulas in CD should enable the treating physician to determine optimal management strategy.
Vote: A+=80%, A=15%, D=5%; grade of recommendation: 1C
1.2 Scoring of perianal fistula activity in CD should enable the treating physician to evaluate disease severity and response to therapy.
Vote: A+=70%, A=20%, A−=5%, D−=5%; grade of recommendation: 1C
Discussion Several classification and scoring systems have been developed in an attempt to quantify disease extent and severity of pCD.6–16 We propose that a distinction is made between a detailed anatomic description of perianal fistulas (ie, classification) and the assessment of fistula activity (scoring), a dynamic measure that is sensitive to change under treatment. However, both components are necessary to design an optimal therapeutic strategy and are relevant for prognosis (table 1).
Descriptive and dynamic measures to evaluate perianal fistulas
Statement 2—Fistula activity
Evaluation of fistula activity is recommended both by clinical and radiological (MRI) features.
Vote: A+=70%, A=20%, A−=5%, D+=5%; grade of recommendation: 2C
Discussion The Perianal Disease Activity Index (PDAI) is based on the assessment of quality of life (pain/restriction of activities and restriction of sexual activities) and perianal disease severity (fistula discharge, type of perianal disease, and degree of induration) rated on a five-point Likert scale.13 It was tested for reliability and responsiveness and was validated against physicians’ and patients’ global assessments.13 A cut-off PDAI score >4 resulted in 87% accuracy when using clinical assessment (active fistula drainage and/or signs of local inflammation) as reference.17 ‘Fistula drainage assessment’ was first used to quantify fistula healing in a randomised controlled trial (RCT) with infliximab.14 A fistula was considered ‘closed’ when it no longer drained despite gentle finger compression. A response was defined as a reduction of 50% or more in the number of draining fistulas on at least two consecutives visits. Fistula remission was defined as the absence of any draining fistulas on two consecutive visits. Although this clinical assessment has been used in further RCTs, it has several drawbacks.18–20 ‘Gentle finger compression’ is largely investigator dependent and is an approach that has never been formally validated. Persistent tracts without fluid drainage are scored as ‘remission’. Moreover, the external appearance of the fistula is used as a surrogate for the whole internal fistula tract. MRI studies have shown that internal fistula healing lags behind clinical remission by a median of 12 months.21 The site of a former/residual fistula tract could be the path of least resistance for a new or recurrent fistula tract to occur.22 In an attempt to combine anatomical fistula description and features reflecting active inflammation, van Assche et al16 developed an MRI based scoring system. Anatomical components include the number and course of the fistula tracts, while the activity of inflammation was evaluated by hyperintensity of fistula tracts on T2 weighted MRI images, the presence of abscess and proctitis.16 The score was validated against the PDAI but had a weak correlation (r=0.371, p=0.036).22 One year of infliximab therapy was associated with significant improvement of the Van Assche score, particularly for the item T2 hyperintensity.23 Disappearance of contrast enhancement was the only MR feature associated with clinical remission.23 In a more recent study, this score was found to be insensitive to change in patients with reduced fistula calibre during long term follow-up.21 Recently, perianal fistula length assessed by MRI was found to be a predictor of response to treatment.24 In conclusion, improved instruments to score perianal CD fistula activity are needed.
Statement 3—Fistula anatomy
3.1 The course of the fistula tract in relation to the anal sphincter and the levator plate (superficial, intersphincteric, transsphincteric, suprasphincteric, extrasphincteric, and supralevator or infralevator) is an important component for classification.
Vote: A+=90%, A=5%, D−=5%; grade of recommendation: 2B
3.2 High and low transsphincteric fistulas should be distinguished in the classification. Fistulas are defined as low when the tract runs through the lower one third of the external anal sphincter.
Vote: A+=70%, A=20%, A−=10%; grade of recommendation: 2C
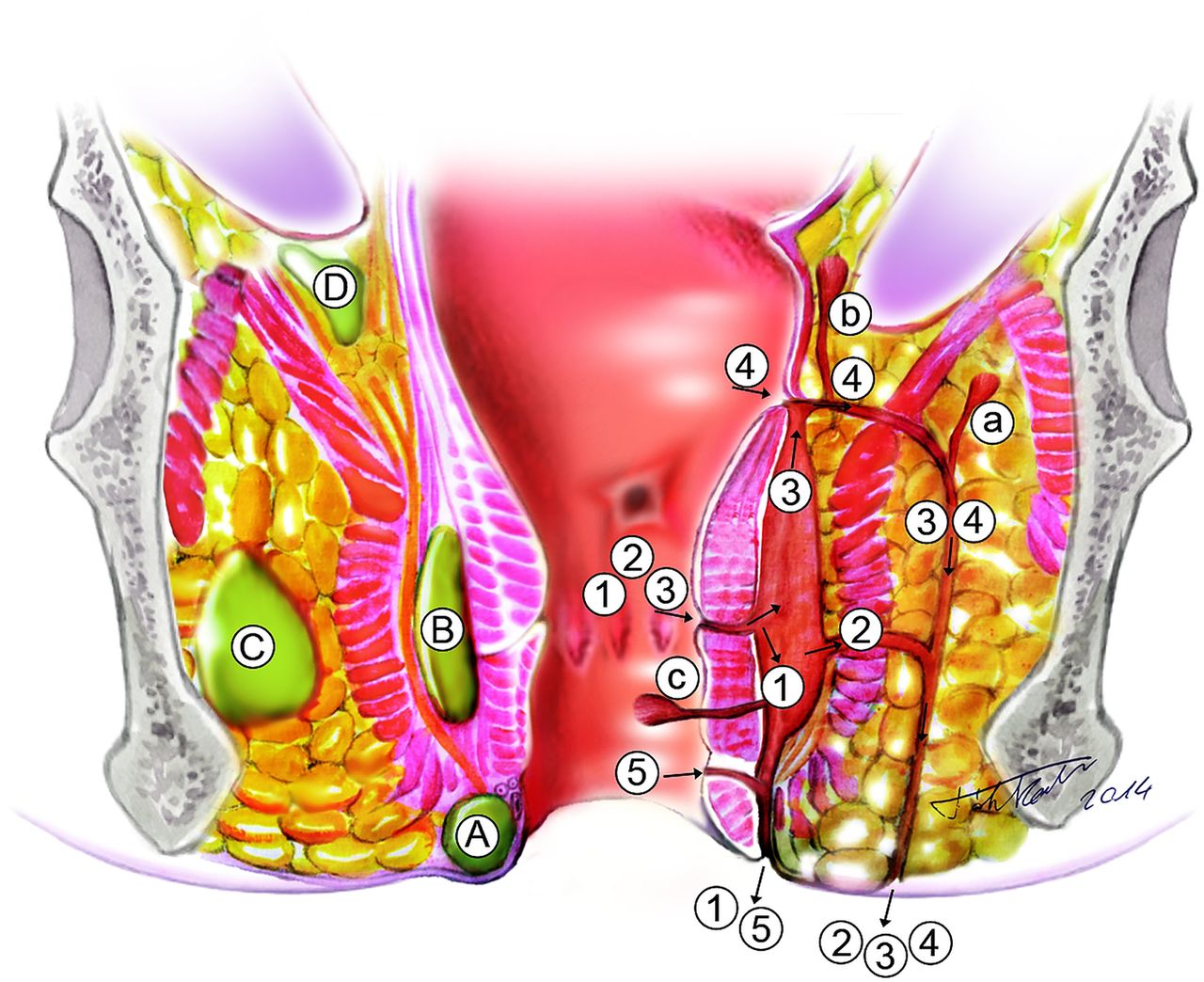
Discussion Parks et al6 studied the anatomy of perianal fistulas and the associated risk of post-surgical incontinence in 400 consecutive patients, as illustrated in figure 1. Section 4 describes the impact of fistula anatomy on surgical treatment.

Disease characteristics relevant for fistula management. A fistula is a tract of pus and/or granulation tissue between two epithelial surfaces lined with a fibrous wall.10 Primary tracts are connections between the internal and external openings (1–5), while secondary tracts are blind extensions (a–c). A tract is defined ‘low’ when it runs through the lower one third of the external anal sphincter.6 The course of the fistula tracts is described by the Parks classification. The external sphincter complex, defined by the external sphincter and the puborectal muscle, serves as reference: (1) intersphincteric: the tract penetrates the internal sphincter and runs through the intersphincteric space to the perianal skin; (2) transsphincteric: the tract penetrates both the internal and the external sphincter or the puborectal muscle; (3) suprasphincteric: tract runs first upwards in the intersphincteric space, then downwards crossing the levator ani muscle and then reaching the perianal skin; (4) extrasphincteric: tract originates from the rectal wall and runs down through the levator ani muscle, without penetrating the external sphincter or the puborectal muscle.6 Later a fifth category was added for superficial tracts (5) that did not involve the sphincter complex. Secondary tracts and their relationship to the levator plate (a) infralevator or (b) supralevator and (c) horizontal extension, also known as ‘horseshoes’, are distinguished. Furthermore proctitis and the presence of abscesses with regard to their localisation (A, perianal; B, intersphincteric; C, ischiorectal; D, suprasphincteric) are also noted.
Statement 4—Proctitis
The presence of proctitis, defined as any ulceration and/or stricture in the rectum, or inflammation and/or stricture of the anal canal, is an important component for fistula assessment.
Vote: A+=90%, A=10%; grade of recommendation: 1C
Discussion The presence of proctitis is highly relevant for fistula management and prognosis as discussed in detail in sections 3 and 4.
Statement 5—Abscess
A perianal abscess clinically defined as fluctuation and radiologically defined as a confined fluid collection (a hyperintense lesion on T2 weighted MRI images and/or a hypo- or anechoic area with endoanal ultrasound (EUS)) with a rim of inflammatory tissue (rim enhancement on post-contrast T1 weighted MRI images and/or often poorly demarcated lesions on EUS) is an important component for classification.
Vote: A+=55%, A=35%, A−=10%; grade of recommendation: 2C
Discussion Perianal CD fistulas are frequently accompanied by abscess formation. Timely detection and management of abscesses minimises the risk of further septic complications. Items found to be clinically relevant for fistula management are depicted in figure 1.
Section 2: Diagnosis and follow-up
Statement 6—Endoscopy
Endoscopic assessment of the rectum is essential to determine the most appropriate management strategy.
Vote: A+=85%, A=10%, A−=5%; grade of recommendation: 1C
Discussion Endoscopy allows assessment of the extent and severity of luminal inflammation, and the presence of internal openings and other complications such as strictures and cancer.25 Proctitis is a predictive factor of persistent non-healed fistula tracts and higher proctectomy rate.26
Statement 7—Examination under anaesthesia
Examination under anaesthesia (EUA) has an important role in the diagnosis and classification of pCD. It also allows immediate therapeutic intervention such as abscess drainage and/or seton placement. If a perianal abscess is suspected, EUA with drainage is the procedure of choice and should not be delayed if MRI is not immediately available. However, if additional collections are suspected, imaging is necessary.
Vote: A+=50%, A=35%, A−=10%, D−=5%; grade of recommendation: 1C
Discussion Experienced colorectal surgeons are up to 90% accurate (95% CI 78% to 98%) in detecting and classifying perianal fistulas, sinuses, and abscesses.27 As shown in a study with infliximab, higher success rates and lower recurrence rates were attained in patients who underwent EUA with abscess drainage and seton placement before starting anti-tumour necrosis factor (anti-TNF) treatment.28
Statement 8—MRI
8.1 Pelvic MRI is a highly accurate non-invasive modality for the diagnosis and classification of perianal fistulas; therefore it is considered the gold standard imaging technique for perianal CD. MRI provides additional detailed information on luminal disease location, disease severity, and fluid collections.
Vote: A+=90%, A=10%; grade of recommendation: 1B
Discussion MRI accurately visualises the anal sphincter and the pelvic floor muscles, as well as the fistula tracts and abscesses, with an accuracy ranging from 76–100% (figure 2).29–32 In addition, MRI may identify clinically ‘silent’ abscesses and luminal inflammation (figure 3).33 T2 weighted sequence with fat suppression is the optimal technique for MR fistula imaging. A gadolinium enhanced T1 weighted sequence is useful for the differentiation between fluid/pus and granulation tissue (table 2). Phased-array external coils have larger field of view with good coverage for supralevator fistulae.30 Endoanal coils provide an advantage in identifying internal openings; however, they are less widely available and have a restricted field of view.34
Interpretation of MRI

Representative MR image of a male patient with perianal fistulising Crohn's disease. (A) Coronal oblique T2 weighted turbo spin-echo sequence and (B) axial oblique fat saturated T1 weighted turbo spin-echo sequence demonstrate a transsphincteric fistula (arrow) with a seton in place (thin arrow), an intersphincteric abscess (curved arrow) with bilateral granulation tissue filled extensions (arrowheads) in the puborectal muscle.

Representative MR image of a female patient with perianal fistulising Crohn's disease and proctitis. (A) Axial oblique T2 weighted turbo spin-echo sequence and (B) axial oblique fat saturated T1 weighted turbo spin-echo sequence show a thickened rectal wall (arrow), with increased enhancement and surrounding infiltrate (arrowheads).
Statement 9—Endoanal ultrasound
EUS (with or without hydrogen peroxide) is a useful alternative to MRI in diagnosing perianal CD fistulas; however, accuracy can be limited by its restricted view.
Vote: A+=50%, A=45%, D−=5%; grade of recommendation: 2B
Discussion EUS (with a frequency between 5–16 MHz) allows a detailed visualisation of the anal sphincter complex with accuracy between 86–95% for correct classification and 62–94% for identification of internal openings.35–37 However, EUS cannot accurately identify ischioanal fossa or supralevator abscesses, as the penetration is limited.27 The use of endoluminal probes can be restricted by luminal stenosis. In selected cases, local infusion of hydrogen peroxide or colour Doppler EUS with saline injection improves visualisation.38–40 When prospectively comparing hydrogen peroxide enhanced three dimensional EUS and endoluminal MRI with surgical assessment as reference, 81% and 90% agreement was found, respectively.41 Furthermore, the Crohn’s Ultrasound Fistula Sign (CUFS) can differentiate between Crohn's related and cryptogenic fistulae-in-ano with a positive and negative predictive value of 87% and 93%, respectively.42 As a complementary method, the accuracy of transperineal ultrasound to detect and classify fistulas was found to be comparable to EUS. However, its accuracy to diagnose deep abscesses is low (47.1%) due to restricted field of view.43 Transperineal ultrasound may offer an advantage in detecting anovulvar fistulae (88.9% vs 44.4% when compared with MRI).43 Both EUS and MRI are superior to clinical examination when assessing and monitoring perianal fistulas.27 ,44–46 In a meta-analysis of four studies comparing EUS and MRI, performance characteristics for MRI (0.87, 95% CI 0.63 to 0.96) and EUS (0.87, 95% CI 0.70 to 0.95) demonstrated comparable sensitivities in detecting perianal fistulas. The specificity for MRI (0.69, 95% CI 0.51 to 0.82) was higher than that for EUS (0.43, 95% CI 0.21 to 0.69).47 A comparison of EUS and MRI diagnostic features is summarised in table 3. The choice mainly depends on local availability, expertise and the complexity of the pCD.
EUS and MRI in the diagnosis of Crohn's perianal fistulas
Statement 10—Fistulography and CT
The diagnostic accuracy of fistulography and CT is poor in the diagnosis and classification of Crohn's perianal fistulas. Fistulography can, however, provide additional information in some exceptionally complex fistulas.
Vote: A+=50%, A=35%, A−=5%, D=5%, D−=5%; grade of recommendation: 1C
Discussion Fistulography and CT are outdated modalities in the diagnostic evaluation of pCD because of exposure to radiation and poor visualisation of the anatomic relationship of the fistulas to the pelvic floor muscles.48 Only in highly selected cases may fistulograms offer additional information and influence surgical management.49
Statement 11—Combination of diagnostic modalities
To ensure diagnostic accuracy and to determine an optimal management strategy, a combination of diagnostic modalities is recommended, namely endoscopy and MRI/EUS (depending on availability and expertise) and EUA.
Vote: A+=60%, A=20%, D=10%, D−=10%; grade of recommendation: 2C
Discussion In a prospective study of 32 patients with perianal CD the accuracy of each diagnostic modality was excellent (EUS 91%, EUA 91%, MRI 87%) and the combination of EUA with MRI or EUS increased accuracy to 100%.27 A diagnostic algorithm for Crohn's perianal fistulas is proposed in figure 4.
Section 3: Medical treatment
Statement 12—Treatment goals
The short term goals in the treatment of pCD are abscess drainage and reduction of symptoms. The long term goals are resolving fistula discharge, improvement in quality of life, fistula healing, preserving continence, and avoiding proctectomy with stoma.
Vote: A+=90%, A=10%; grade of recommendation: 1C
Statement 13—Corticosteroids and aminosalicylates
There is no demonstrated role for aminosalicylates or corticosteroids in perianal CD.
Vote: A+=90%, A=10%; grade of recommendation: 1C
Discussion Aminosalicylates have no clinical effect on perianal CD.50 Studies evaluating the effect of corticosteroid treatment in fistulising CD showed worsening of discharge and increased need for surgery.51
Statement 14
Antibiotics, namely metronidazole and ciprofloxacin, improve fistula symptoms and may contribute to healing.
Grade of recommendation: 1C
Therefore, antibiotics are only recommended as adjunctive treatments for fistulas.
Vote: A+=74%, A=16%, A−=10%; grade of recommendation: 2C
Discussion
Early small and uncontrolled series reported fistula improvement after 6–8 weeks of antibiotic therapy (metronidazole 750–1500 mg/day, ciprofloxacin 500–1000 mg/day) with frequent relapse upon discontinuation and commonly occurring side effects.52–54 Only one RCT comparing ciprofloxacin, metronidazole and placebo assessed the efficacy of systematic antibiotics for pCD.55 This short (10 weeks) and underpowered study (n=25) showed no difference between antibiotics and placebo for fistula closure.55 Neither topical nor systemic metronidazole led to improvement of PDAI in prospective though small trials.56 ,57
Two double blind RCTs assessed the efficacy of ciprofloxacin combined with anti-TNF therapy.58 ,59 The first study combined ciprofloxacin with infliximab (n=24) and reported fistula response at week 18 in 73% of patients, versus 39% with infliximab alone (p=0.12).58 In another RCT the effect of combination therapy with ciprofloxacin and adalimumab was superior to adalimumab monotherapy (in the reduction of at least 50% of the number of draining fistula in 70.6% vs 47.2% (p=0.047)) at week 12.59 However, after discontinuation of ciprofloxacin the difference between the two groups diminished. Overall these results support the efficacy of antibiotics in reducing fistula drainage but not fistula healing.
Statement 15
Thiopurines may have a moderate effect in the treatment of pCD. Evidence for the efficacy of methotrexate and ciclosporin is limited. Tacrolimus is effective for treating active fistulas; when used, therapeutic drug monitoring is required to minimise toxicity.
Vote: A+=32%, A=32%, A−=26%, D+=10%; grade of recommendation: 2C
Discussion
Thiopurines There is no prospective controlled trial involving azathioprine or 6-mercaptopurine with fistula outcome assessed as the primary end point. Available results are derived from a subgroup analysis of a randomised double blind study, where 31% of patients treated with 6-mercaptopurine experienced complete fistula closure compared to 6% of the placebo patients.11 A recent meta-analysis excluding the above study did not show any efficacy of azathioprine for improving or closing fistulae (OR 4.68, 95% CI 0.6 to 36.69; p=0.14, n=18).60 In contrast, an earlier meta-analysis assessing the efficacy of thiopurines in 70 patients showed that 54% of patients treated with thiopurines had fistula healing versus 21% of patients treated with placebo (OR 4.44, 95% CI 1.5 to 13.2).61 The effect of antibiotic and azathioprine combination therapy was evaluated in a prospective open label study and showed the superiority of the combination therapy (p=0.03).62
Methotrexate There are no clinically relevant trial data on the effect of methotrexate on draining fistulas.
Tacrolimus A single, short term, placebo controlled trial randomised 46 patients with actively draining Crohn's fistulas to treatment with oral tacrolimus or placebo.18 The primary end point—defined as the closure of at least 50% of fistulas maintained for at least 4 weeks—was reached in 43% on active treatment versus 8% on placebo (p=0.004). However, complete closure of all fistulas was not more common in the tacrolimus group.18 There was more nephrotoxicity with tacrolimus, which was managed by dose reduction.18 Topical tacrolimus showed no significant benefit.63
Ciclosporin Several observational studies reported on the efficacy of ciclosporin for fistulising CD. Clinical improvement was rapid, but relapse rates were high after drug discontinuation.64–66 Related adverse events limited further use of ciclosporin.
Statement 16
Infliximab (grade of recommendation: 1A) and adalimumab (1B) are moderately effective for the induction and maintenance of fistula closure. Evidence for efficacy of certolizumab pegol is weaker (1C). Anti-TNF and thiopurine combination therapy may lead to higher fistula healing response and closure rate compared to monotherapy (2C).
Vote: A+=26%, A=42%, A−=16%, D=11%, D+=5%.
Discussion
Infliximab Two RCTs have assessed the efficacy of infliximab in fistulising CD. In the first placebo controlled trial an induction regimen induced closure of at least 50% of fistulas for at least 4 weeks in 56–68% of patients compared with 26% treated with placebo (p=0.002 and p = 0.02, respectively). Closure of all fistulas was achieved in 38–55% on infliximab.67 The ACCENT II trial further evaluated infliximab maintenance therapy for this indication. Week 14 responders to the induction regimen were randomised to further treatment with placebo or infliximab 5 mg/kg every 8 weeks.68 Time to loss of response was significantly longer on infliximab (>40 weeks) than on placebo (14 weeks, p=0.001). Moreover, 39% of patients who received infliximab maintenance therapy had complete closure of all draining fistulas at week 54.68
Adalimumab There has not been a dedicated controlled trial for fistulising CD with adalimumab. In two placebo controlled trials, CLASSIC-1 and GAIN, the rates of fistula improvement and remission did not differ significantly in adalimumab treated patients at week 4 compared to placebo.69 ,70 In the CHARM trial—a 56-week phase III trial to assess the efficacy of maintenance treatment with adalimumab among responders to induction treatment—a subgroup analysis in patients with draining fistula(s) at baseline showed complete fistula healing in 33% of adalimumab treated patients versus in 13% of placebo treated patients (p<0.05).20 An open label extension of this trial showed sustained healing in 90% of patients on adalimumab treatment at 2 years follow-up.71 In further open label studies, adalimumab was effective in 23–29% of patients with fistulising CD who had lost response or become intolerant to infliximab.72–74
Certolizumab Subgroup analysis of PRECiSE 1 and 2—two large trials assessing the efficacy of certolizumab pegol for moderate to severe CD—looked at fistula response. At week 26, 36% of patients on certolizumab pegol had complete fistula closure compared with 17% on placebo (p=0.038).75 In contrast, no statistical difference was found in the rate of fistula response, defined as >50% closure at two consecutive visits.75 A meta-analysis also evaluated the efficacy of anti-TNFs in pCD, and infliximab was found to have the most available evidence.76
Immunosuppression + anti-TNFs Data remain conflicting concerning the efficacy of concomitant immunosuppression with anti-TNF agents in pCD. Subgroup analysis of the ACCENT II trial found that concomitant immunosuppressants did not improve response rates to infliximab at 1 year.68 In the SONIC trial 12% of patients had perianal fistulas, but no separate analysis was performed in this group. Nevertheless, the gain with combination therapy is of particular interest in patients with proctitis.77 In support, recent studies suggest a clear association between combination therapy and fistula closure.78
Surgery and anti-TNFs In a large retrospective cohort, 218 patients underwent surgery alone or surgery plus biological therapy. Surgery included seton drainage, fistulotomy, rectal advancement flap, fistulotomy plus seton or other procedures. Clinical response was 35.9% in the surgery treated group and 71.3% in the combined treatment group (p=0.001), suggesting that combined treatment modalities offer a better outcome.79
Experimental medical treatments are discussed in the online supplementary material.
Section 4: Surgical management
Statement 17—Abscess drainage
Surgical drainage of perianal abscesses is generally recommended before initiating medical therapy.
Vote: A+=100%; grade of recommendation: 1C
Discussion In symptomatic perianal CD fistulas are frequently preceded or accompanied by perianal abscesses.80 Surgical drainage as opposed to spontaneous drainage minimises the risk of further septic complications aggravated by concomitant immunosuppressive treatment.81
Statement 18—Setons
Non-cutting seton placement is useful in order to prevent (recurrent) abscess formation.
Vote: A+=85%, A=15%; grade of recommendation: 1C
Discussion As all fistulas are potential sources of pelvic sepsis, ensuring adequate drainage is fundamental. Seton drains maintain patency of the fistula tracts and hence limit recurrent abscess formation.82 Loose setons preserve the integrity of the external anal sphincter and are to be preferred.83 In contrast, cutting setons carry a high risk of anal incontinence (54%) due to scarring of the anal canal.84 A disadvantage of setons is that the fistula tract cannot ‘close’ with the seton in place. The optimal timing for seton removal is not well established. In the ACCENT 2 study, all setons were removed by week 2 and the overall new abscess rate was 15%. Several other studies report maintaining seton(s) in situ for longer, thus seton removal at week 2 may be too early.19 ,85 In a small prospective trial, where setons were maintained for the duration of infliximab induction, the overall new abscess rate was 0%.81 These results show that loose seton drainage is an efficient and safe method in the treatment of Crohn's perianal fistulas. It is recommended to keep the seton in place until at least the induction of the anti-TNF treatment period has been completed. Fistula closure can be achieved after seton removal.
Statement 19—Proctitis
The surgical treatment of pCD in patients with proctitis is limited to abscess drainage and non-cutting seton placement. Further surgical attempt for fistula closure is recommended only after endoscopic remission of the proctitis has been achieved.
Vote: A+=70%, A=30%; grade of recommendation: 1C
Discussion Both proximally active luminal disease, causing increased bowel frequency, and proctitis are associated with problematic wound healing.86 Combined infliximab therapy and surgery has been more successful in the absence of luminal inflammation, especially when localised in the rectum.87 Proctitis is also associated with a higher proctectomy rate (29–77.6%).26 ,88 Therefore, active luminal disease in pCD is an indication for aggressive medical treatment.88
Statement 20—Fistulotomy
Fistulotomy is a treatment option for symptomatic superficial and, occasionally, low intersphincteric fistulas, always with consideration for preservation of continence. Performing fistulotomy in low transsphincteric fistulas, especially if anteriorly located in women, is associated with a high risk of incontinence.
Vote: A+=60%, A=35% A−=5%; grade of recommendation: 2C
Discussion In symptomatic superficial, low intersphincteric and selected low transsphincteric fistulas, fistulotomy or lay-open is a safe method, which preserves the continence and offers high healing and low recurrence rates in the absence of proctitis (table 4). In contrast, fistulotomy for high transsphincteric, suprasphincteric and extrasphincteric fistulas is associated with decreased healing and increased incontinence rates.89 Furthermore, as the anterior part of the external anal sphincter is shorter in women, fistulotomy for low transsphincteric fistulas carries a higher risk of incontinence.
Fistulotomy in low fistulas
Statement 21—Definitive surgical repair
Options for definitive surgical repair of pCD include fistulotomy, mucosal advancement flaps (MAFs), bioprosthetic plugs, and ligation of the intersphincteric fistula tract (LIFT). The use of fibrin glue and stem cell injections is not well established yet.
Vote: A+=20%, A=35%, a−=40%, D=5%; grade of recommendation: 2C
Discussion
Mucosal advancement flap (MAF) is a surgical treatment option for the closure of internal fistula openings. It entails mobilisation of a rectal mucosal flap to cover the primary fistula opening, thereby closing the high pressure end of the fistula, whereas the sphincter complex remains untouched. The excluded fistula segment is expected to dry out over time. In a systematic review of 35 studies with an average follow-up of 28.9 months, the success rate of MAF for Crohn's fistulas was 64% (range 33.3–92.9%). The incontinence rate was 9.4% with a wide interstudy variability (range 0–28.6%). Re-interventions were needed in almost 50% of patients.90
Plugs, made of collagen, or more recently porcine intestinal submucosa, are inserted via the internal fistula opening to fill the fistula tract and leave the sphincter apparatus untouched. Success rates in retrospective cohorts and one open label study with a median follow-up of 6–15 months varied between 24–88%.91–94 One of the studies reported that failure was caused by dislodgement of the plug in 22% of the cases; however, the closure rate was reported as excellent (87%) when a suturable bioprosthetic plug was used.95 In general, plugs may offer a valid first line option for surgical treatment; measures to prevent dislodgement and perioperative antibiotics may increase success and safety, although costs can be a major concern.
Ligation of the intersphincteric fistula tract (LIFT) is a surgical option in the management of transsphincteric fistulas when the tract has matured into a fibrotic tube with granulation tissue enabling ligation and transection.96 The procedure is based on closure of the internal opening and removal of infected tissue via an intersphincteric approach. In the first small case series, a 94% success rate was reported and these results were confirmed by a pilot study including 40 patients96 ,97 A recent study showed more moderate success rates (56% healing >1 year) and all recurrences were within 2 months after the surgery.98 Prospective studies with higher numbers of Crohn's patients are further awaited.
Fibrin glue consists of fibrinogen and thrombin. Upon mixing, a fibrin clot is formed, which is thought to stimulate wound healing by inducing angiogenesis and fibroblast growth. Data show varying success rates for fistula closure, which may be due to the heterogeneity of the studies regarding fistula origin (Crohn's vs cryptoglandular) and follow-up (table 5). A meta-analysis found no significant difference between fibrin glue and conventional surgery with regard to recurrence and faecal incontinence rates.99
Fibrin glue
Stem cell based therapy Mesenchymal stem cells have a high degree of plasticity and ability to modulate immune cells. Peri- or intrafistular injection of autologous expended adipose derived stem cells, as well as bone marrow derived stem cells, were previously proven to be feasible and safe.100–102 Initial results show that stem cell±fibrin glue treatment induces fistula closure in 56–82% of patients (vs 16% in the fibrin glue treated patients, p<0.001), and 53% and 30% of patients sustained fistula remission at 1 and 3 years, respectively.103–106 Although these initial results on stem cell based therapy seem promising, results of further randomised, placebo controlled, ongoing trials on Crohn's fistulas are needed.
Gracilis muscle transposition In a single retrospective study including 18 CD patients, gracilis transposition was successful for complex fistulas in 64% and for persistent non-healing perineal sinuses in 50% of the cases with maintained efficacy (90% upon 10 months median follow-up).107
Statement 22—Diverting stoma
A diverting temporary stoma is an option for patients with severe, complicated, therapy refractory pCD.
Vote: A+=80%, A=20%; grade of recommendation: 1C
Statement 23—Proctectomy
Transperineal intersphincteric close rectal proctectomy with permanent stoma is the treatment of last resort in severe, therapy refractory fistulising disease.
Vote: A+=60%, A=35%, A−=5%; grade of recommendation: 1C
Discussion In complicated, therapy refractory perianal disease a defunctioning stoma should be considered. Based on retrospective data, early remission rates are quite high (up to 81%); however, sustained remission can only be achieved in 26–50% of cases (table 6). Most patients with a stoma ultimately require proctectomy and intestinal continuity can only be restored in a minority of patients.26 The only study that was conducted in the era of biologicals showed a reduced need for completion proctectomy and a relatively higher rate of restoration. Main risks of proctectomy include damage to the pelvic nerves, presacral abscesses, and delayed perineal wound healing. Overall, the use of a diverting stoma should be reserved for patients who have uncontrollable sepsis and tissue destruction, or for patients who have failed conservative therapy. Alternatively, in selected patients, permanent faecal diversion can be avoided by coloanal pull-through or Turnbull-Cutait abdominoanal pull-through procedures, provided that the colon and the anus are intact.
Diverting stoma and proctectomy

Diagnostic algorithm for perianal fistulising Crohn's disease. In perianal abscess is suspected, MRI is an optional diagnostic method, if readily available, before surgical incision and drainage. Alternatively diagnostic endoscopy can also be performed during examination under anaesthesia (EUA), to minimise patient discomfort. A second EUA might be necessary if seton placement is needed or was not successful upon the first EUA. When stricture is present, Bougie or gentle finger dilation is preferable to preserve sphincter function. EUS, endoanal ultrasound.
Conclusions
Optimal management of pCD requires a multidisciplinary approach. Diagnostic accuracy is usually achieved by a combination of modalities. Surgical drainage of sepsis is the first line therapy before initiating immunosuppressive treatment. Antibiotics and thiopurines are recommended as adjunctive treatments in Crohn's fistulas. Of all available anti-TNF agents, the efficacy of infliximab is best documented. Anti-TNF can be used as first line medical treatment, optionally in combination with antibiotics and/or thiopurines. Oral tacrolimus is an option in therapy refractory patients in an attempt to avoid surgical stoma. Definitive surgical repair of fistulas, including fistulotomy, MAF, LIFT, plug and glue, is only of consideration in the absence of luminal inflammation. Proctectomy with permanent stoma is the last resort for severe, therapy refractory disease. A combined medical and surgical treatment algorithm is proposed in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment algorithm for perianal fistulising Crohn's disease. AB, antibiotics; ADA, adalimumab; AF, advancement flap; D, drainage; I, incision; IFX, infliximab; IS, immunosuppressants; LIFT, ligation of the intersphincteric fistula tract.
Acknowledgments
We thank Adam Baker from the University of Western Ontario for his help in conducting the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators On behalf of the WCOG Working Party: Guillaume Bouguen: Robarts Research Institute, Amsterdam, The Netherlands, London, Ontario, Canada and San Diego, California, USA, and Service des Maladies de l'Appareil Digestif et INSERM U991, Centre Hospitalier Universitaire Pontchiallou et Université de Rennes 1, Rennes, France; Andreas Sturm: Department of Gastroenterology, Krankenhaus Waldfriede, Charité Universitätsmedizin, Berlin, Germany; Andre D'Hoore Department of Surgery, University of Leuven, Leuven, Belgium; David Laharie: CHU de Bordeaux, Hospital Haut-Lévêque, Bordeaux, France; Brian Feagan: Robarts Research Institute, Amsterdam, The Netherlands, London, Ontario, Canada and San Diego, California, USA and University of Western Ontario, London, Ontario, Canada; William Sandborn: Robarts Research Institute, Amsterdam, The Netherlands, London, Ontario, Canada and San Diego, California, USA and Division of Gastroenterology, University of California San Diego, La Jolla, California, USA; Bruce Sands: Mont Sinai Medical Center, New York, New York, USA; Jean-Frederic Colombel: Mont Sinai Medical Center, New York, New York, USA.
-
Contributors KG performed systematic literature searches, drafted statements and algorithms and drafted the supporting text for the manuscript. WAB contributed with surgical aspects on finalising statements about classification and surgical treatment, revised the algorithm on management and the supporting text on surgical treatment. MAK contributed with practical aspects on improving all statements, revised the algorithms and the supporting text. JS contributed to optimising statements and the algorithm on diagnosis and carefully revised the corresponding supporting text. RK performed systematic literature searches and drafted statements on diagnosis. SCN, JP, GvA, ZL and AH contributed to optimising statements and algorithms during the whole preparation process and carefully revised the supporting text. BGL performed systematic literature searches, drafted statements on medical treatment and drafted the corresponding supporting text. GD'H took the initiative for this Expert Consensus, supervised each step of the process, and made final revisions of the supporting text.
-
Funding Financial support was provided by a standard grant for Working Party Report from the World Gastroenterology Organization (WGO) and Robarts Research Institute. The proposal was initially developed and supported by the International Organization for the study of Inflammatory Bowel Diseases (IOIBD) and the European Society of Coloproctology (ESCP). The pharmaceutical industry was excluded from all stages of the process.
-
Competing interests KBG reports having received speakers’ honoraria from MSD. JS has a consultancy agreement with Robarts Clinical Trials. RK and ZL have no conflicts of interest to declare. JP reports grants and personal fees from Abbvie and MSD, and personal fees from BMS, Boehringer-Ingelheim, BMS, Janssen, Roche–Genentech, Novo Nordisk, Nutrition Science Partners, Pfizer, Tygenix, and Topivert. SCN reports having received speakers’ honoraria from Janssen and Ferring Pharmaceuticals. She has received research grants from Janssen and Ferring Hong Kong. AH has received consulting fees from Abbott Laboratories/AbbVie, Atlantic Healthcare Limited, Bristol Meyers Squibb, Ferring Pharmaceuticals, Shire Pharmaceuticals, Schering Plough Corporation (acquired by Merck), Warner Chilcott UK Limited and Tillotts Pharma. She has received lecture honoraria from Abbott Laboratories/AbbVie, Ferring Pharmaceuticals, Shire Pharmaceuticals, Schering Plough Corporation (acquired by Merck), Warner Chilcott UK Limited. She has received research funding from Abbott Laboratories/AbbVie, Cook Pharmaceutical, MSD. GB has received lecture fees from Abbvie, Ferring, and MSD Pharma. WS reports having received consulting fees from Abbott Laboratories, ActoGeniX NV, AGI Therapeutics Inc, Alba Therapeutics Corporation, Albireo, Alfa Wasserman, Amgen, AM-Pharma BV, Anaphore, Astellas Pharma, Athersys, Inc., Atlantic Healthcare Limited, Axcan Pharma (now Aptalis), BioBalance Corporation, Boehringer-Ingelheim Inc, Bristol Meyers Squibb, Celegene, Celek Pharmaceuticals, Cellerix SL, Cerimon Pharmaceuticals, ChemoCentryx, CoMentis, Cosmo Technologies, Coronado Biosciences, Cytokine Pharmasciences, Eagle Pharmaceuticals, Eisai Medical Research Inc, Elan Pharmaceuticals, EnGene, Inc, Eli Lilly, Enteromedics, Exagen Diagnostics, Inc, Ferring Pharmaceuticals, Flexion Therapeutics, Inc, Funxional Therapeutics Limited, Genzyme Corporation, Genentech (now Roche), Gilead Sciences, Given Imaging, Glaxo Smith Kline, Human Genome Sciences, Ironwood Pharmaceuticals (previously Microbia Inc), Janssen (previously Centocor), KaloBios Pharmaceuticals, Inc, Lexicon Pharmaceuticals, Lycera Corporation, Meda Pharmaceuticals (previously Alaven Pharmaceuticals), Merck Research Laboratories, MerckSerono, Millennium Pharmaceuticals (subsequently merged with Takeda), Nisshin Kyorin Pharmaceuticals Co, Ltd, Novo Nordisk A/S, NPS Pharmaceuticals, Optimer Pharmaceuticals, Orexigen Therapeutics, Inc, PDL Biopharma, Pfizer, Procter and Gamble, Prometheus Laboratories, ProtAb Limited, Purgenesis Technologies, Inc, Receptos, Relypsa, Inc, Salient Pharmaceuticals, Salix Pharmaceuticals, Inc, Santarus, Schering Plough Corporation (acquired by Merck), Shire Pharmaceuticals, Sigmoid Pharma Limited, Sirtris Pharmaceuticals, Inc (a GSK company), S.L.A. Pharma (UK) Limited, Targacept, Teva Pharmaceuticals, Therakos, Tillotts Pharma AG (acquired by Zeria Pharmaceutical Co, Ltd), TxCell SA, UCB Pharma, Viamet Pharmaceuticals, Vascular Biogenics Limited (VBL), Warner Chilcott UK Limited, Wyeth (now Pfizer). He has received lecture fees from Abbott Laboratories, Bristol Meyers Squibb, and Janssen (previously Centocor). He has received research support from Abbott Laboratories, Bristol Meyers Squibb, Genentech, Glaxo Smith Kline, Janssen (previously Centocor), Millennium Pharmaceuticals (now Takeda), Novartis, Pfizer, Procter and Gamble Pharmaceuticals, Shire Pharmaceuticals, and UCB Pharma. BGL reports having received consulting fees from Prometheus Labs, and Santarus Inc, speakers’ honoraria from Warner Chilcott, and UCB Pharma. GD'H has received consultancy fees from Abbott Laboratories, Actogenix, Boerhinger Ingelheim, Centocor, Cosmo Technologies, Engene, Ferring Pharmaceuticals, GlaxoSmithKline, Jansen Biologics, Millenium Pharmaceuticals, Mitsubishi Pharma, Merck Research Laboratories, Novo Nordisk, PDL Biopharma, Pfizer, Schering Plough, SetPoint, Shire Pharmaceuticals, Sigmoid Pharma Ltd, Takeda, Teva, Tillotts Pharma, UCB Pharma; research grants from Abbott Laboratories, Jansen Biologics, Given Imaging, MSD, DrFalk Pharma, Photopill; speaking honoraria from Abbott Laboratories, Jansen Biologics, Tillotts, Tramedico, Ferring, MSD, UCB, Norgine and Shire; stock options from Engene Inc.
-
Provenance and peer review Not commissioned; externally peer reviewed.