Measles, measles vaccination, and Crohn's disease
BMJ 1998; 316 doi: https://doi.org/10.1136/bmj.316.7146.1745 (Published 06 June 1998) Cite this as: BMJ 1998;316:1745
Second immunisation has not affected incidence in England
- Elizabeth Miller, Head of immunisation division,
- Pauline Waight, Principal scientist
- Public Health Laboratory Service Communicable Disease Surveillance Centre, London NW9 5EQ
- European Programme of Intervention Epidemiology Training, Helsinki, Finland
- University of Helsinki, Department of Public Health, Helsinki, Finland
- Department of Infectious Disease Epidemiology, National Public Health Institute, Helsinki, Finland
- Department of Epidemiology and Public Health, Imperial College School of Medicine, London SW10 9NH
EDITOR—Metcalf concludes that the scientific evidence does not support a causal link between measles virus and Crohn's disease.1 Though few readers of the BMJ are likely to disagree with her appraisal of the science, parental concern about the safety of the vaccine remains high fuelled by continuing media interest in this controversial topic. More worrying is the recent decline in MMR vaccine coverage2 and evidence which suggests that most practice nurses would not give their own child a second dose of MMR vaccine because of concerns about vaccine safety.3
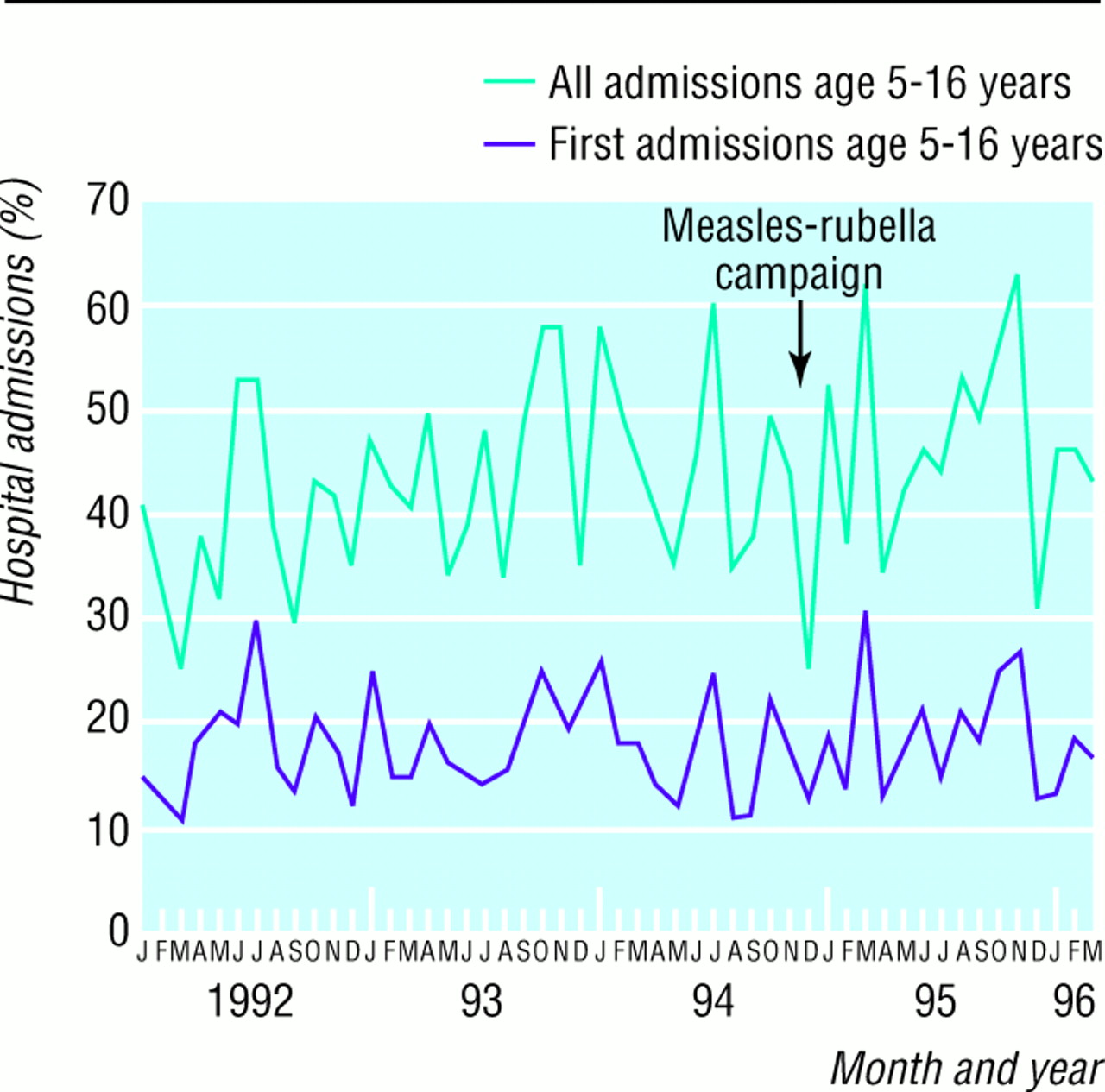
Hospital admissions for Crohn's disease, January 1992 to March 1996
{kind=link}
One of the claims made by the leading proponent of the hypothesis that measles vaccine causes Crohn's disease is that there has been a “dramatic escalation” in paediatric cases in the wake of the 1994 national measles-rubella vaccination campaign targeted at school aged children.4 We have monitored hospital discharge diagnoses for Crohn's disease (ICD-9 code 555 until March 1995, ICD-10 code K55 from April 1995) in children aged 5-16 years before and after the campaign using computerised hospital episode statistics from all districts in England (figure). Children with new cases of Crohn's disease are almost always admitted to hospital, and this is a well established method of monitoring trends in incidence of the disease. Repeat admissions in the same child were identified by matching sex, date of birth, and postcode.
No increase was evident in either first admissions or all admissions for Crohn's disease since the campaign. Although the latent period between exposure to measles-rubella vaccine and alleged onset of Crohn's disease was not stated by Wakefield, our data exclude an effect within the first 16 months. This technique can be reapplied annually, allowing the cohort immunised in the 1994 campaign to be followed longer term.
We are not aware of any published evidence to support the hypothesis that re-exposure to measles vaccine can provoke the onset of Crohn's disease. However, evidence which counters unsubstantiated allegations may help health professionals reassure themselves, as well as concerned parents, about the safety of measles vaccine given as a second dose in combination with another live viral vaccine.
References
Crohn's disease has not increased in Finland
- R G Pebody, Fellow,
- M Paunio, Senior researcher,
- P Ruutu, Chief of Infectious Disease Surveillance Unit
- Public Health Laboratory Service Communicable Disease Surveillance Centre, London NW9 5EQ
- European Programme of Intervention Epidemiology Training, Helsinki, Finland
- University of Helsinki, Department of Public Health, Helsinki, Finland
- Department of Infectious Disease Epidemiology, National Public Health Institute, Helsinki, Finland
- Department of Epidemiology and Public Health, Imperial College School of Medicine, London SW10 9NH
EDITOR—We believe Finnish data can add to the discussion about exposure to wild measles virus or MMR vaccine and subsequent development of Crohn's disease.1 Finland has had a national register of those prescribed long term treatment for Crohn's disease since 1986. We used the register to obtain the annual number of incident Crohn's cases from 1986-92 in those aged 0-14 and 15-24 years.
Transmission of wild measles virus was still occurring in Finland in the 1970s despite 70% coverage with monovalent Schwarz vaccine since 1975. In 1982, a two dose MMR vaccination programme was launched for 14-18 month and 6 year old children; coverage for the two doses was over 90%,2 and wild virus was eradicated.3 In 1992 we randomly sampled 453 children from the National Population Register who had remained healthy during the last measles outbreak in Finland in 1988. Vaccination status and measles history were determined from the child's home or health care centre vaccination card (unpublished data). We calculated the proportion of each annual birth cohort for 1967-87 who received 0, one, two, and three doses of measles vaccine (some received one dose of Schwarz and two doses of MMR vaccine) or had wild measles infection regardless of vaccination status.
From 1986 to 1992 the proportion of 15-19 year olds infected by wild virus fell sharply (figure), with a significant increase in the proportion receiving one or more doses of measles vaccine. Over the same period the proportion of 10-14 year olds receiving two or more doses of MMR vaccine increased. Few 10-14 year olds have had measles.
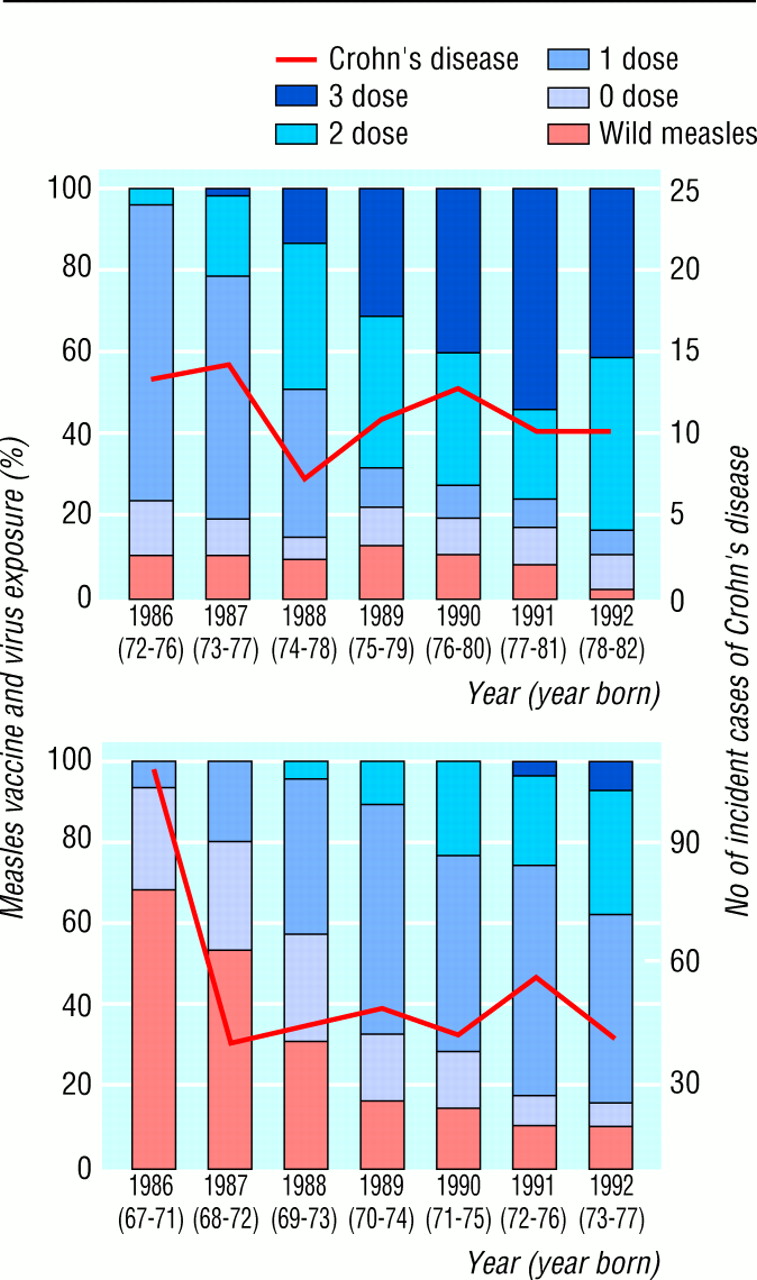
Annual incident cases of Crohn's disease and lifetime measles vaccination and wild measles virus exposure in 10-14 and 15-19 year olds in Finland, 1986-92
{kind=link}
The annual number of incident cases of Crohn's disease for 15 to 24 year olds fell the year after the registry was started. This is probably due to inclusion of previously diagnosed cases. The annual number of cases has since remained stable for both age groups (8/100 000/year for 15-24 year olds and 1/100 000/year for 0-14 year olds).
Over the 10 years widespread exposure to wild virus at 1-9 years of age has changed to multiple doses of live attenuated vaccine starting at 14 months of age. However there has been no difference in the incidence of Crohn's disease after follow up for up to 19 years. Although these data do not exclude a possible association between wild measles virus and Crohn's disease, if early exposure to MMR vaccine increased the risk we would expect an increasing incidence of Crohn's disease in Finland in these age groups.
Age specific prevalences do not suggest association with in utero exposure
- Ross Lawrenson, Senior lecturer in public health,
- Richard Farmer, Professor
- Public Health Laboratory Service Communicable Disease Surveillance Centre, London NW9 5EQ
- European Programme of Intervention Epidemiology Training, Helsinki, Finland
- University of Helsinki, Department of Public Health, Helsinki, Finland
- Department of Infectious Disease Epidemiology, National Public Health Institute, Helsinki, Finland
- Department of Epidemiology and Public Health, Imperial College School of Medicine, London SW10 9NH
EDITOR—Before immunisation was introduced in 1963 there was a regular pattern of measles epidemics every two years in England and Wales. If the proposed association between exposure to measles in utero and subsequent development of Crohn's disease1 truly exists then it would be expected that babies born in the year of a measles epidemic would have a higher risk of subsequently developing Crohn's disease. Consequently the age specific prevalence of Crohn's disease should vary from year to year.

Prevalence of Crohn's disease by year of birth and annual notification of measles
{kind=link}
Data on the notification of measles are available from 1942, and the UK primary care database (UKPCD) can be used to estimate the age specific prevalence of Crohn's disease. We identified 924 553 patients from England and Wales aged 20-55 years (born between 1942 and 1977), of whom 1036 had a diagnosis of Crohn's disease—a prevalence of 11.2 per 10 000. The age specific prevalence for each year shows no obvious association with the pattern of measles epidemics (figure). The highest prevalence of Crohn's disease was in those born between 1949 and 1954. The age specific prevalence since then has been relatively steady and does not support the proposition from Hermon-Taylor et al of a rise in incidence in the disease.2 We support Metcalf in her conclusion that there is unlikely to be a causal association between exposure to measles in utero and subsequent Crohn's disease.