Article Text

Statistics from Altmetric.com
Non-invasive imaging techniques such as ultrasound (US) or computed tomography (CT) are widely used for the diagnosis and monitoring of many pancreatic and biliary tract diseases. However, these techniques have limitations, such as the low sensitivity of ultrasound for detecting common duct calculi, which means that the diagnosis of several common conditions including tumours (benign and malignant), calculi, sclerosing cholangitis and chronic pancreatitis may still require invasive procedures such as endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC).
These invasive techniques also have disadvantages—for example, ERCP requires direct cannulation of the common bile or pancreatic duct, sedation, the use of ionising radiation and a team of trained, experienced personnel. Complications include haemorrhage, sepsis, pancreatitis, bile leakage, as well as a recognised mortality.1 ERCP may not be technically possible and this, along with the complication rate, has been related to operator experience.2 In clinical practice these complications are usually offset by the diagnostic information obtained and the ability to proceed immediately to therapeutic intervention when required.
Magnetic resonance cholangiopancreatography (MRCP) is a relatively new technique for non-invasive imaging of the biliary and pancreatic duct systems. Early trials suggest that it may have a useful role in clinical practice.
The MRCP technique
“MR cholangiopancreatography” refers to a range of techniques for imaging the biliary tree and pancreatic duct that all exploit the intrinsically long T2 relaxation value of many fluids, including biliary and pancreatic duct secretions. The techniques may be classified by: the MR “refocussing” method used (that is, gradient echo or spin echo), image data collection (that is, 2D or 3D), requirement for image processing to suppress background tissues, type of “receiver” coil (that is, body or specialised surface coils), and the approach used to minimise motion related artefacts especially those related to respiration.
Early attempts to image the biliary and pancreatic ducts used gradient echo methods3-6 with body receiver coils. More recently, spin echo refocussed methods based on RARE (rapid acquisition with relaxation enhancement)7 and its variants combined with specialised surface receiver coils have permitted notable improvements in image quality and permitted faster image acquisition.8-13 Respiratory motion induced blurring has limited demonstration of the pancreatic duct and different approaches have been taken to overcome this.8-12 Specialised receiver coils have also improved image quality.9 ,14 ,15Most techniques have included image post processing, such as the MIP (maximum intensity projection) algorithm, although by using a prolonged echo time this can be avoided.16 A version of this technique is in use at our institution and was used for the MRCP illustrations in this article, each obtained during a single 16 second breath-hold (figs 1-3). Improved MR system performance and new pulse sequences will become more widely available in the near future, permitting further improvements.17 ,18
Volunteer and patient studies
NORMAL STRUCTURES
There have been few studies of normal volunteers: Wallner et al’s early work with a 2D gradient echo technique3failed to identify the undilated biliary tree in three of five volunteers. Reinhold et al 13 compared a 3D gradient echo technique with a 2D MIP RARE technique in 26 patients with suspected bile duct abnormalities; a body coil was used for both sequences. The RARE approach consistently outperformed the gradient echo technique demonstrating one or more intrahepatic ducts, the extrahepatic ducts and a portion of the main pancreatic duct in 100%, 96% and 65% as opposed to 42%, 44% and 23% of patients, respectively. Using a 2D RARE breath-hold projection technique and a body coil, Laubenberger et al 16 demonstrated the undilated intrahepatic and extrahepatic ducts in all 30 normal volunteers studied. In the same study part or all of the main pancreatic duct was visualised in all the volunteers. Using a similar technique with a torso phased array coil, Lomas19demonstrated the normal pancreatic duct in 10 normal volunteers, showing the entire duct in eight, and the duct within the pancreatic head only in the remaining two.
NORMAL VARIANTS
Anatomical variants of the common bile duct and the insertion of the cystic duct are particularly important to the laparoscopic surgeon. Taourel et al,20 using a 3D MIP RARE technique with a torso phased array coil, successfully identified the cystic duct in 74 % of 171 patients: a low cystic duct insertion was shown in 11 (9%) of these patients, a medial cystic duct insertion in 22 (17%), a parallel course of the cystic and hepatic ducts in 31 (25%), and an aberrant right main hepatic duct in 12 (9%).
Using a non-breath-hold 3D MIP RARE technique and a body coil, Sotoet al 21 reported a sensitivity for detecting pancreas divisum of 66%. Improved results were achieved by Bretet al,15 using a similar approach but with a phased array torso coil and one or multiple breath-holds. They accurately identified pancreas divisum in six of 108 patients in whom ERCP correlation was also available.
BILIARY OBSTRUCTION
Although the earlier gradient echo techniques could detect the presence of biliary obstruction in 100%4-6 and its level in up to 90%5 of cases, they could not be used to determine accurately the underlying cause of obstruction and high grade stenosis and complete obstruction were difficult to distinguish. Improved results were again achieved with RARE based techniques. The largest series of 126 patients,10 with good correlation of the findings, used a 3D MIP RARE technique with a phased array torso coil. Imaging was performed with an extended breath-hold (64 seconds, 100% oxygen presaturation) or quiet respiration. Obstruction was identified with a sensitivity, specificity and accuracy of 91%, 100% and 94%, respectively. The diagnosis of the underlying aetiology of the obstruction was identified with positive and negative predictive values of 93% and 94% for calculi, and 86% and 98% for malignant stricture. In addition, MRCP routinely identifies the dilated biliary tree upstream of an obstruction, allowing synchronous strictures to be identified. This is not always possible with ERCP where visualisation of an obstructed part of the biliary tract may not be possible.
Using a rapid breath-hold 2D RARE projection technique with a body coil, Laubenberger et al 16 diagnosed with 100% accuracy the presence of obstruction, its level and extent and the underlying aetiology in all 30 patients when compared with ERCP. The undilated ducts downstream of the obstruction could be identified in addition to the dilated obstructed ducts upstream. Figures 1 and 2 are of patients with biliary obstruction imaged using a similar technique.

: An oblique sagittal MRCP projection image obtained in a 16 second breath-hold in a 72 year old man with obstructive jaundice owing to multiple common duct calculi, confirmed at ERCP.

: A 41 year old man with multiple hilar biliary strictures secondary to right hepatic artery occlusion. (A) Coronal MRCP image obtained in a 16 second breath-hold which demonstrates the strictures and the dilated obstructed left biliary ducts (arrows) not visualised on (B) the corresponding ERCP examination.
CHRONIC PANCREATITIS
The main indications for ERCP in chronic pancreatitis are to assist the diagnosis, and to detect anatomical variations such as pancreas divisum. ERCP plays a key part in the diagnosis of chronic pancreatitis,22 23 although the radiological findings in mild disease are inconsistent.24
MRCP has not been to shown to have a role in mild disease and currently has limited spatial resolution for demonstrating side branch abnormalities (fig 3). MRCP may be of value in the diagnosis of moderate and severe disease when main duct abnormalities and filling defects may occur. Soto et al used a respiratory triggered 3D MIP RARE technique to image the pancreatic duct during quiet respiration,21 achieving a sensitivity of 87–100% for duct dilatation, and a sensitivity and specificity of 75% and 69%, respectively, for stricture detection, although the latter was increased to 81% by reviewing the source images themselves. Takeharaet al assessed a breath-hold 3D MIP RARE technique with a phased array surface coil in 39 patients with known severe chronic pancreatitis.9 Agreement with ERCP in this selected group was 82–92% for ductal dilatation, 70–92% for ductal narrowing and 92–100% for filling defects with low interobserver variation overall.
{kind=link}
{kind=link}
{kind=link}
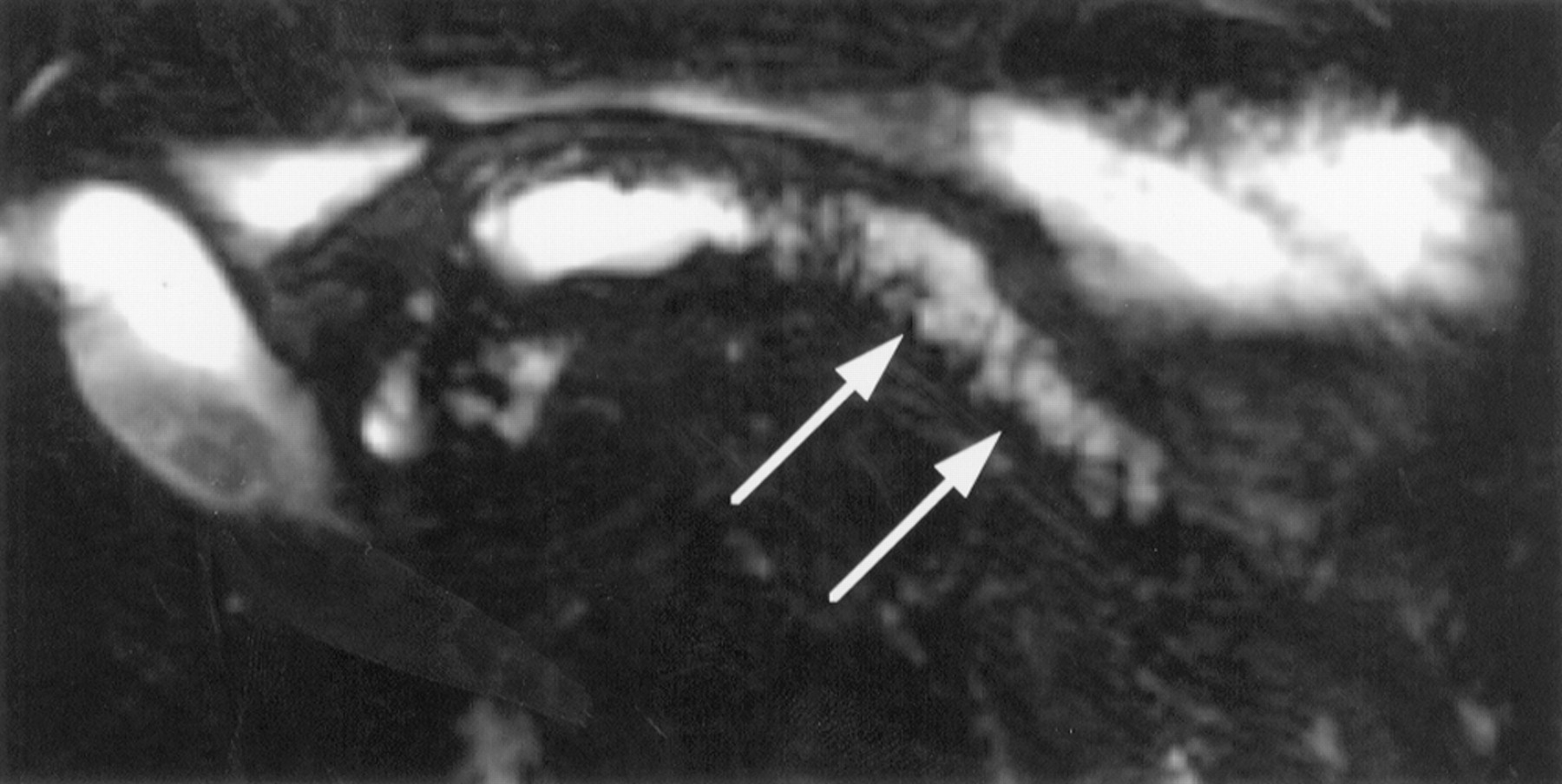
: A 48 year old man with severe chronic pancreatitis. An axial image from his MRCP examination demonstrates the abnormally dilated main duct and side branch ducts in the pancreatic tail (arrows) which could not be demonstrated at ERCP.
ACUTE AND RECURRENT PANCREATITIS
ERCP may be used to detect an underlying cause for acute or recurrent pancreatitis, particularly choledocholithiasis, and evidence suggests that early ERCP and sphincterotomy may be beneficial,25 although it is associated with an increased complication rate. As far as we are aware there have been no MRCP studies addressing this aspect, although anecdotally we have used MRCP successfully for recurrent pancreatitis to detect a communicating pseudocyst not demonstrated at ERCP.
AFTER FAILED ERCP
ERCP may be technically impossible after gastric or duodenal surgery where the antral and duodenal anatomy has been altered, and when normal variants or obstruction are encountered. Soto et al 27 studied 39 consecutive patients in whom ERCP had been unsuccessful using a non-breath-hold 3D MIP RARE technique and a body coil. MRCP was successful in all patients and of particular relevance is that normal examinations were obtained in 11 patients, and minor abnormalities requiring conservative management only in a further eight cases.
ERCP may fail to visualise parts of the biliary and pancreatic duct system upstream of an obstruction, making it difficult to exclude synchronous lesions and to plan appropriate therapeutic intervention. Because of the need at ERCP to pass the obstruction to inject contrast media, the visualisation of an obstructed upstream system in this way is associated with an increased risk of sepsis. In such cases MRCP has been shown to visualise reliably the upstream ductal systems often made more conspicuous by their increased diameter (fig2).18 ,26
Present limitations
Certain patients are excluded routinely from MRI because of risks associated with the static magnetic field—for example, patients with cardiac pacemakers and ferromagnetic cerebral aneurysm clips, and a small percentage (1–5%) will not tolerate the procedure because of claustrophobia. Fluid collections external to the biliary and pancreatic ducts, such as ascites, may obscure the region of interest or generate motion related artefacts. In our experience the ability to obtain targeted 2D images in any desired plane can reduce such problems.
Ferromagnetic clips close to the area being imaged may distort the image and make it non-diagnostic, although RARE sequences are relatively resistant to these effects. MR compatible titanium surgical clips and stents are becoming available and may avoid this problem.
The spatial resolution of MRCP is limited when compared with ERCP. Stones less than 4 mm in diameter can be imaged routinely,10 even with MIP techniques, and the sensitivity may be improved by reviewing the source images, or performing projection RARE sequences. Undoubtedly, further studies will be required to assess fully the best technique and the diagnostic performance of MRCP for detecting duct calculi. Other factors may influence this as the diagnosis relies upon demonstrating intraluminal filling defects and there are likely to be false positive results from other causes such as blood clots, protein plugs, and gas bubbles. Finally, MRCP is a purely diagnostic technique and a positive result may require a more invasive therapeutic technique, such as ERCP or surgery.
Conclusion
MRCP is a relatively new diagnostic technique with several advantages over other non-invasive and invasive methods of imaging the biliary and pancreatic duct systems. Recent technical developments in MRI now allow diagnostic quality images to be obtained within acceptable breath-holding times on conventional commercial MRI systems. Despite relatively low spatial resolution when compared with ERCP the early assessments of diagnostic performance suggest that MRCP can (1) reliably demonstrate normal and abnormal pancreatic and biliary ducts; (2) accurately diagnose the site and cause of obstruction; (3) be of diagnostic value when ERCP is unsuccessful.
MRCP may ultimately prove to be of value in selecting those patients who require a therapeutic ERCP (or PTC), thereby reducing the number of these studies which are found to be normal. In addition it may have a role in planning therapeutic drainage procedures by providing a more complete picture of the duct system anatomy than may be available by other techniques. Further technical refinements are likely and MRCP techniques are expected to become more widely available on current MR systems within the few next years.
Acknowledgments
We would like to thank Dr Alex Gimson for his assistance in the preparation of this article.