Article Text

Statistics from Altmetric.com
One of the few aspects of the epidemiology of inflammatory bowel disease (IBD) that seems indisputable is the emergence of both ulcerative colitis and Crohn’s disease in the economically developed nations of Western Europe and North America during the past century.1 Some of the apparent increase in incidence undoubtedly reflects a receding tide of mimicking infectious diseases and developments in endoscopic and other diagnostic techniques. Nevertheless, most epidemiologists accept that there were considerable real increases in ulcerative colitis incidence during the first half of this century and of Crohn’s disease incidence during the middle half-century in these countries.2 As the millennium approaches, are the incidences of each disease continuing to increase? Some reports suggest they are, whereas claims that Crohn’s disease incidence is no longer increasing can provoke a rapid response from some clinicians.3-6 At a time when basic science is making progress by leaps and bounds, why should such an apparently simple epidemiological question prove so difficult to answer, and does it matter?
Assessing time trends in the incidence of most chronic diseases is difficult and IBD poses particular problems. Firstly, the data routinely collected on mortality and morbidity from IBD are of little help. In most countries over 75% of deaths attributed to IBD are in the elderly and mortality rates are a twentieth or less of the incidence figures for the same period. Although national mortality statistics show a broad correlation with individual incidence studies from those countries, the relation between mortality and incidence within countries is weak, such that during the 1950s and 1960s mortality rates from Crohn’s disease in England and Wales and the USA showed a small less than twofold increase when individual studies of Crohn’s disease incidence were showing much larger increases.7 ,8 Over the same period ulcerative colitis mortality rates in these countries declined sharply when other studies showed ulcerative colitis incidence was unchanged or increasing. In recent years deaths attributed to ulcerative colitis and Crohn’s disease in England and Wales have gradually fallen, although the trend has been affected by changes in the coding rules for death certification.9
Data on hospital admissions for IBD look more promising and have been collected for some years in several countries including the UK.10 However, it is not possible in the UK to separate first admissions from repeat admissions except in Scotland and in the Oxford region where record linked systems are available. This has become an even greater problem since 1989 as the data now collected refer to finished consultant episodes, several of which can be generated by a single admission. A second problem is the effect of changing thresholds for admission—increasingly patients with IBD are being managed as outpatients with fewer hospital admissions. With this in mind it is notable that data from the Oxford Record Linkage study for the period 1970 to 1986 showed an increase in episode based admission rates for Crohn’s disease but not for ulcerative colitis.11 However, when the admissions were linked to individuals the hospitalised incidence of Crohn’s disease showed no increase over this period, whereas the rates for ulcerative colitis showed a small increase. In contrast, recently published figures from the Danish national registry of (in)patients showed the annual incidence of Crohn’s disease between 1981–84 and 1989–92 to have increased from 46 to 62/106 and from 33 to 41/106 in women and men respectively, and the annual incidence of ulcerative colitis to have fallen slightly from 154 to 133/106 and from 141 to 126/106.12
In the absence of reliable routinely collected statistics, most data on IBD incidence come from ad hoc studies carried out by interested gastroenterologists and usually involving no more than a few hospitals. As a whole these studies are relatively small with the total number of cases often being under 200 and consequently wide confidence limits for the incidence figures produced. The labour involved in doing these studies is considerable and few cover more than a 10 year period. They are usually retrospective, which poses particular difficulties in assessing time trends as case ascertainment is invariably greater for more recently diagnosed cases. Other problems that have not always been carefully tackled include definition of the date of IBD onset, criteria for diagnosis, residence criteria and cross-boundary referrals. Many of these studies have ignored differences in the age structures of the populations and simply compare crude incidence rates over time or place. Although these studies are of some value in establishing a benchmark for IBD incidence in a given population they clearly have major limitations when assessing time trends.
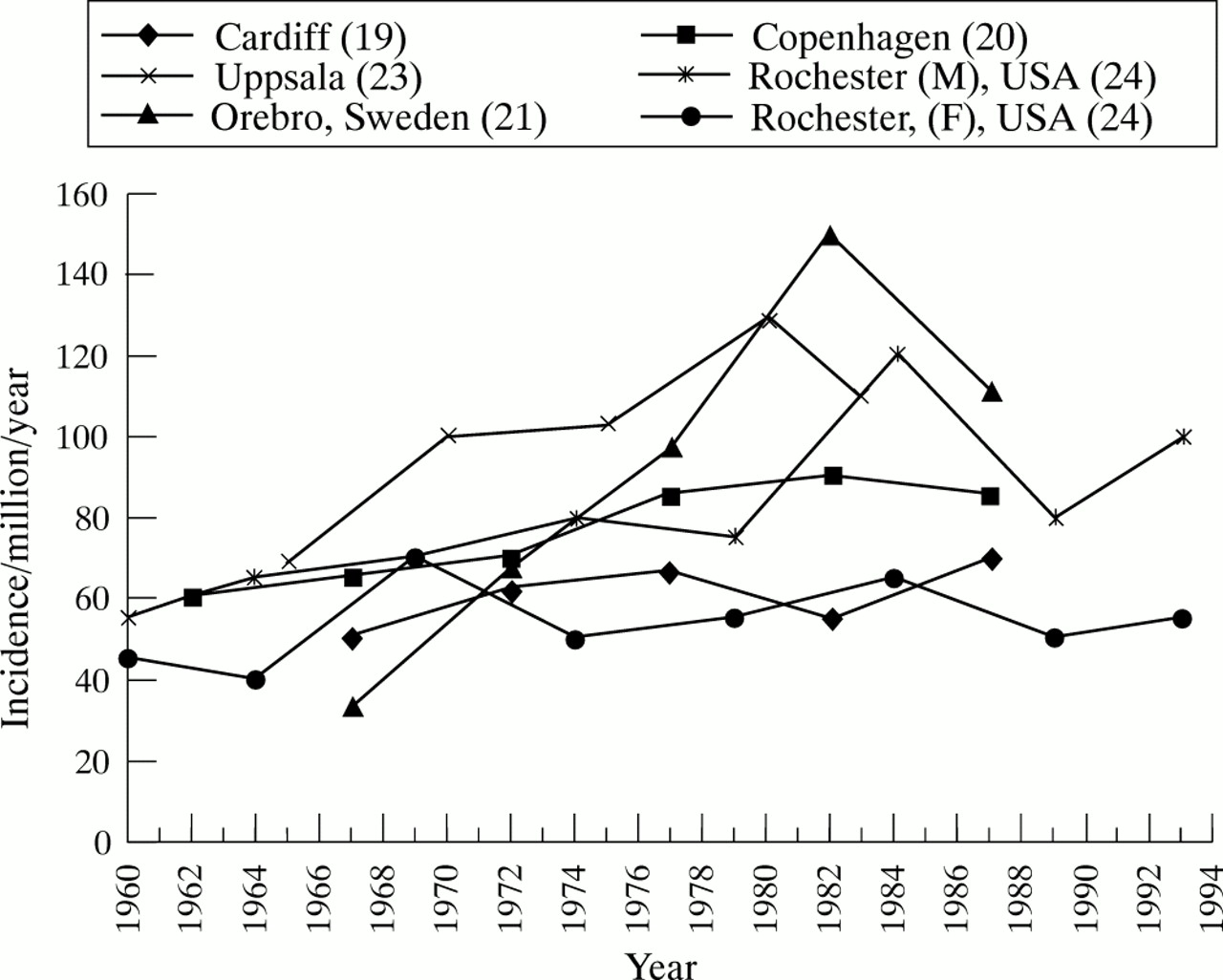
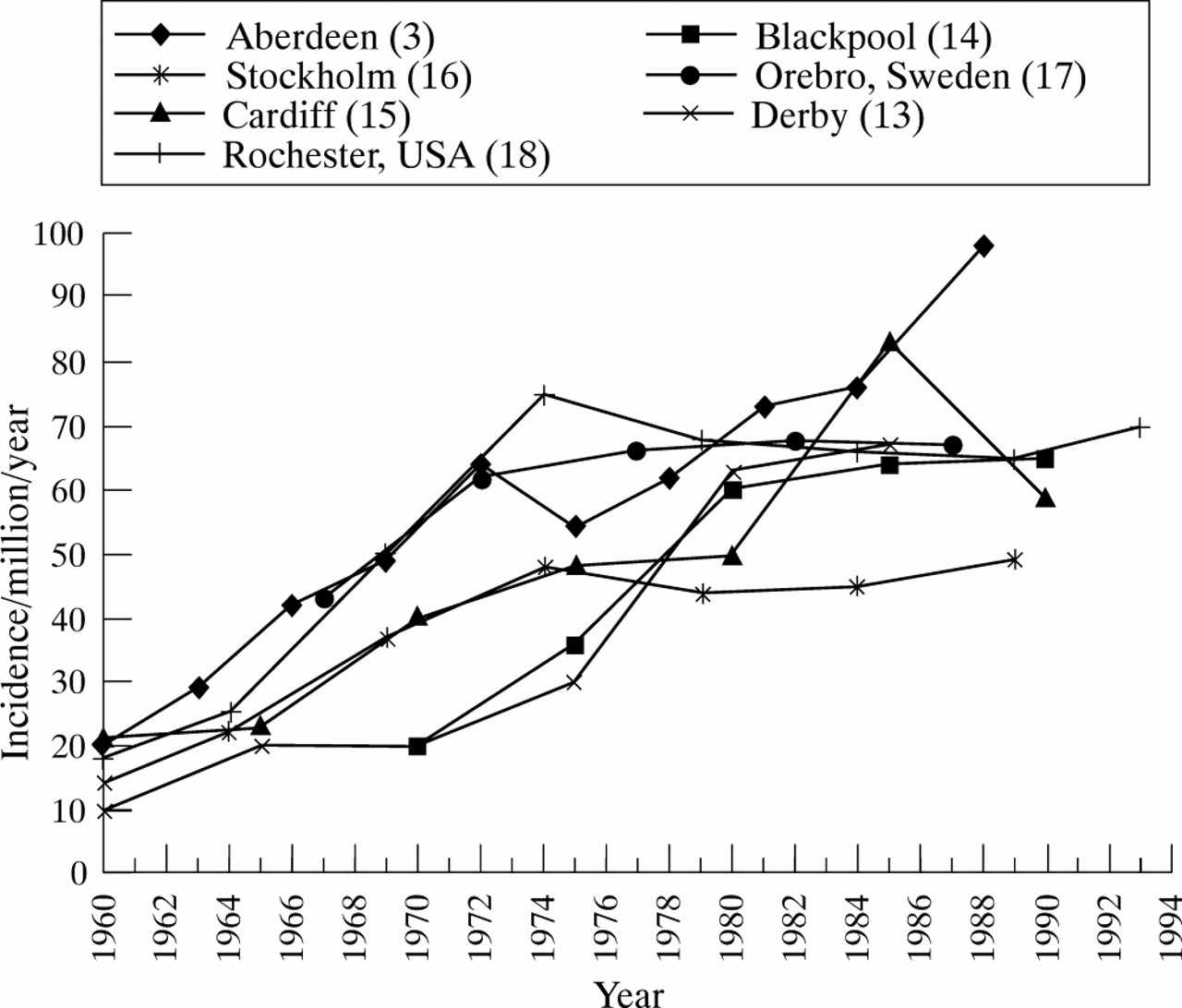
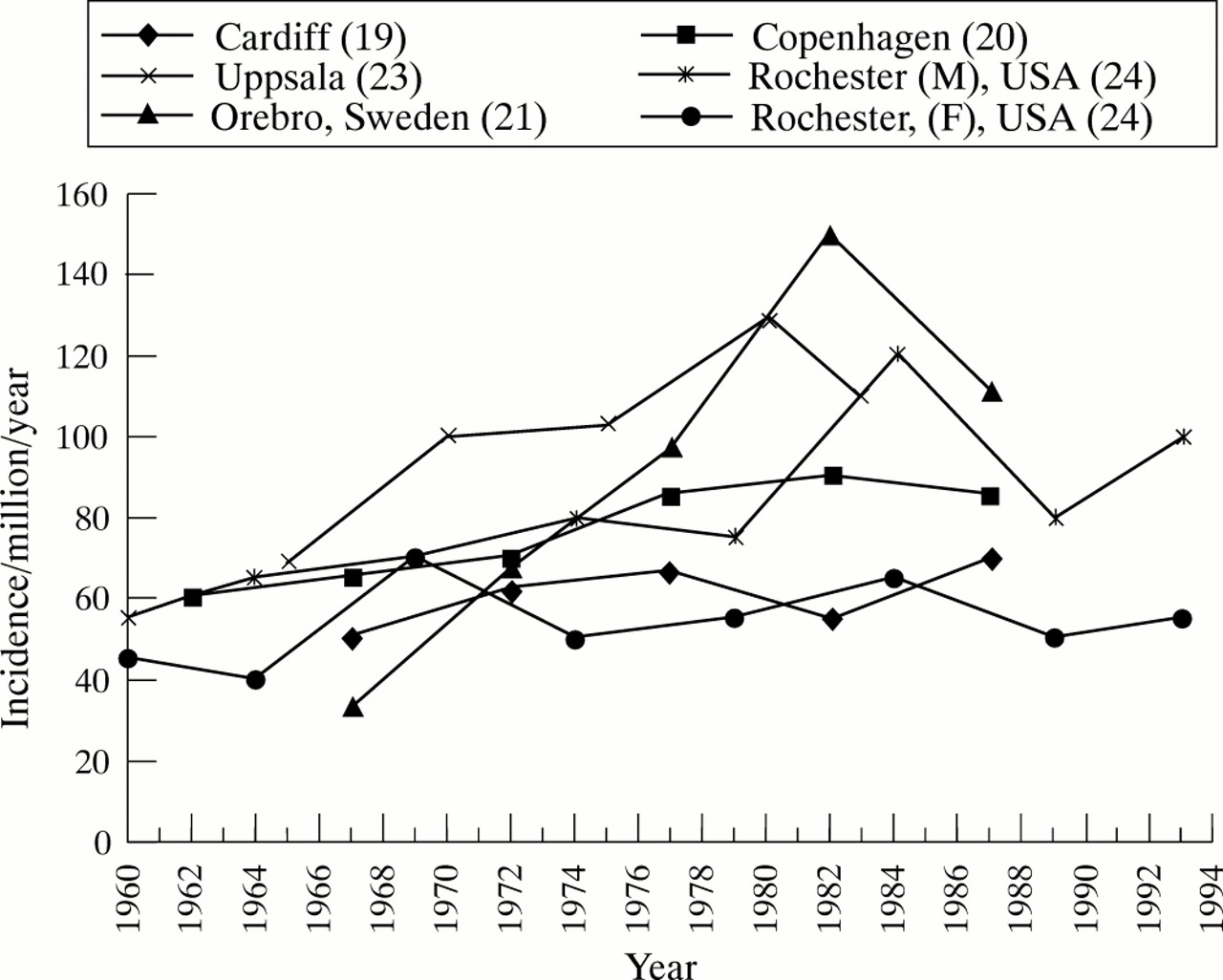
Fortunately, in a few parts of the world IBD incidence has been monitored either prospectively or retrospectively by regularly repeated studies, and it is to these one needs to turn for an accurate assessment of trends. The most recent incidence rates from several of these areas are plotted in figs 1 and 2.3 ,13-24 For the purposes of comparability the rates have been plotted according to the last year of each time period rather than the mid-point. In most of these areas, the rates have also been age standardised to correct for changes over time in their population’s age structure.
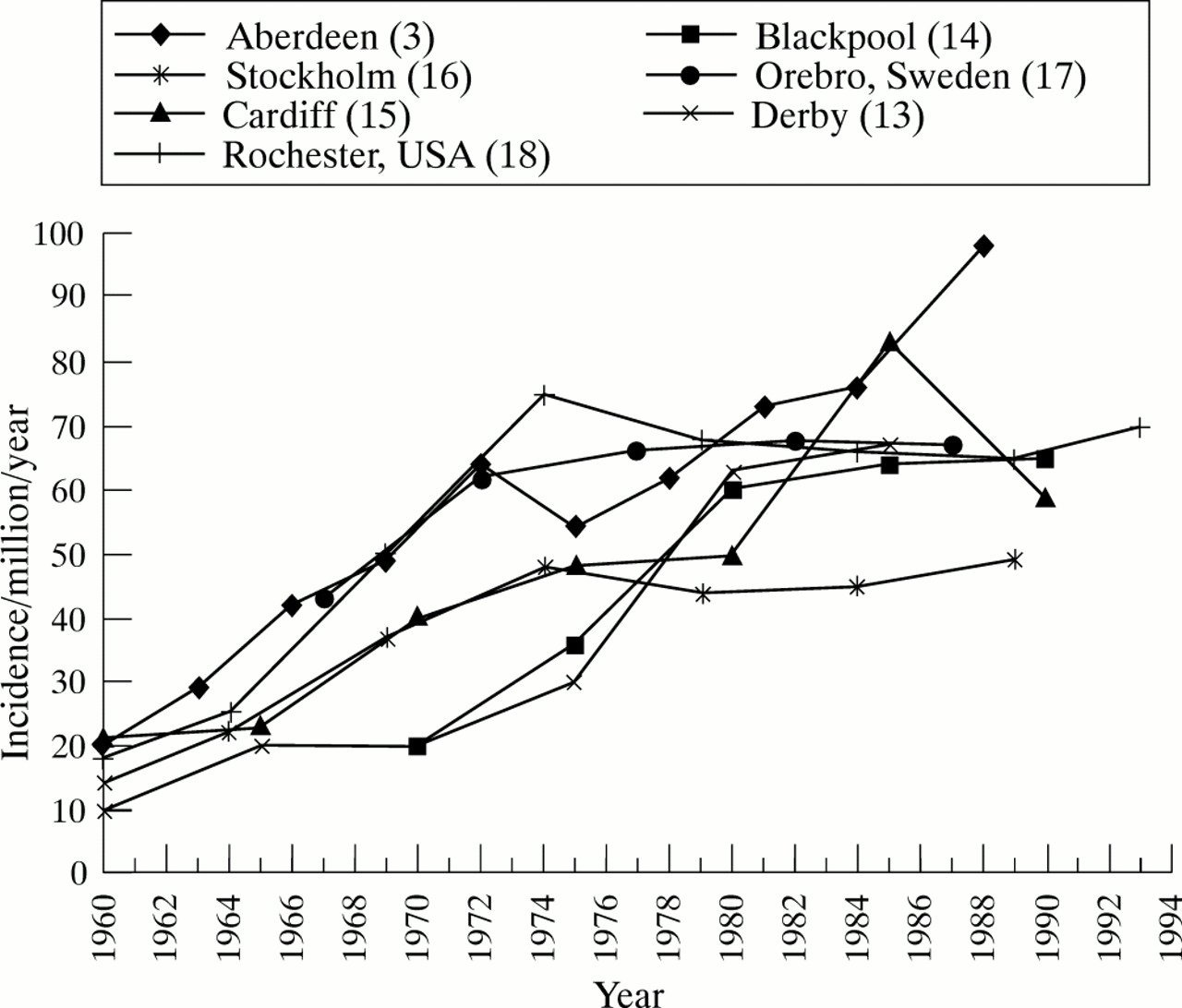
Recent time trends in the incidence of Crohn’s disease.
{kind=link}
{kind=link}
Recent time trends in the incidence of ulcerative colitis.
Is the incidence of Crohn’s disease still increasing?
It is clear that throughout the 1950s and 1960s there was a noticeable increase in the incidence of Crohn’s disease in the northerly nations of Western Europe and in North America.25 The increase was evident in all the areas shown in fig 1 and is mirrored in hospital admission data.10 In some areas of the UK such as Blackpool and Derby, the rapid increase in Crohn’s disease incidence in the early 1970s reflected the appointment of specialist gastroenterologists to the local district general hospitals.13 ,14 Other factors contributing to the general increase include greater awareness of Crohn’s disease, recognition of Crohn’s colitis and transfer from ulcerative colitis.
As shown in fig 1 this general increase seems to have ceased by the beginning of the 1980s. Indeed, other than in Aberdeen and the northeast of Scotland Crohn’s disease incidence rates in these areas are now concentrated in a relatively narrow band between 50 and 70/million/year. At present, it is unclear whether the Scottish figure, which is not age standardised, reflects a sustained increased.3 The growth of the oil industry in the area resulted in a substantial influx of people in age groups at highest risk of Crohn’s disease and in any future analyses it will be interesting to see whether the current high incidence is maintained and whether it is high in all age and sex groups.
Crohn’s disease incidence in children
Stable overall incidence rates might conceal changes in incidence in particular age groups and it has been suggested that Crohn’s disease incidence in children is particularly increasing. Few studies have specifically looked at children, and those that have are divided in choosing age 14 or 15 as the upper limit of childhood. Normally this small difference would matter little. However, because of the steep rise in age specific incidence during the teenage years, the effect of these varying definitions of childhood is difficult to gauge. Furthermore, most studies have used time of diagnosis to define Crohn’s disease onset and any shortening of the time between symptom onset and diagnosis could also have a disproportionate effect on childhood incidence. How these considerations might affect childhood incidence can be seen in figure 2 from the recent paper from Stockholm where Crohn’s disease incidence at age 10–14 has increased from 30 to 50 per million in the most recent time period, but fallen at ages 15–19.16
Judging by hospital admissions of children (age <16) in Scotland, there was a threefold increase in childhood incidence between 1968 and 1983 which, after allowing for a short lag, would seem to parallel the increase seen in adults.26 The final figure of 23/106/year is remarkably similar to the 25/106/year reported from western Norway in 1984–85 and the 22/106/year incidence reported recently in a retrospective study from South Wales for 1983–93.21 ,27In South Wales there was an increase from 13 to 31/106/year between the two halves of the study period. Another Norwegian study carried out prospectively during 1990–93 found an incidence of 20/106/year with rates of 9/106/year for age 0–12 years rising to 72/106/year for those aged 13–15.27 Although incidence seems lower in Denmark, hospital admissions for 0–14 year olds have shown an annual increase of 2–5% since 1981.12 ,28 On balance, it seem there may have been a modest increase in incidence in children which is probably the result of earlier diagnosis rather than a more general increase in incidence in young people.
What has happened to the incidence of ulcerative colitis?
Compared with Crohn’s disease, ulcerative colitis incidence rates have tended to show greater variation with crude rates as high as 200/106/year being found in some prospective studies.2 ,29 Studies of ulcerative colitis incidence face additional problems of ascertainment of mild or asymptomatic disease that nevertheless can be extensive, inclusion or exclusion of proctitis, and single episodes of colitis possibly induced by non-steroidal anti-inflammatory drugs or infection.30 ,31It is therefore reassuring that Moum et al found that although a diagnosis of ulcerative colitis could not be confirmed in 12% of their patients one year after presentation the net effect on the incidence figure was minimal.32
The incidence of ulcerative colitis is generally regarded as having changed little for some time.2 In the areas shown in fig 2there seems to have been a modest increase, but perhaps less than might have been expected given increasing access and uptake of medical care and developments in diagnostic techniques. If hospital admission and mortality rates are an indication of severe disease then the frequency of life threatening fulminant ulcerative colitis seems to be less.8 ,22 This would be consistent with earlier diagnosis and better treatment of more patients with less severe disease.22
One change that does seem to have occurred is in the age specific incidence pattern with an increasing incidence of ulcerative colitis in older men but not women. Traditionally ulcerative colitis incidence has been found to peak at age 15–25 with some studies showing a small second peak at older ages.2 ,20 In contrast, in the recent EC-IBD study incidence peaked later at age 25–34 and in men then showed no significant decline with age whereas the rates in women declined to half those for the men.29 This pattern was consistently seen in both northern and southern Europe but it is not yet known whether it applies to proctitis or to all extents of ulcerative colitis. Although one explanation might be the increasing number of older men who have given up smoking it seems unlikely that this is sufficient to account for all the change.
What do changes in IBD incidence imply?
In general, studies of disease incidence have two purposes: firstly, to generate or test hypotheses about disease aetiology and, secondly, to guide provision of health services. Aetiologically the most striking finding is the recent levelling off in Crohn’s disease incidence which in the face of increasing measles vaccination rates and the notable decline in measles incidence, provides no support for either as causes of Crohn’s disease. Attention is turning to other environmental exposures, both early and later in life. The narrow range of Crohn’s disease incidence seen across the high incidence countries suggests that whatever exposures are responsible they are distributed fairly evenly in these areas. In terms of health service provision one consequence of the earlier increases in incidence of both diseases coupled with their low fatality is that the prevalence of IBD continues to increase. Latest data indicating an IBD incidence of around 200/106/year suggests that in the UK and many parts of Europe as many as 1 in 100 people will suffer one or more often prolonged episodes of IBD in their lifetime.
References
Footnotes
Leading articles express the views of the author and not those of the editor and editorial board.