Article Text

Statistics from Altmetric.com
In the last few years, there have developments in many aspects of liver transplantation. This review will focus on those areas where adult clinical practice has developed1–3; the topics selected are those which, it is hoped, will be of interest and relevance to those health care professionals who refer patients to transplant centres and share in their follow up. In such a review, it is not possible to be comprehensive.
CHANGING INDICATIONS (TABLE 1)
Transplant activity and indications in Europe (data from the European Liver Transplant Registry, kindly provided by Dr Vincent Karam)
Indications for transplantation are evolving: liver failure from hepatitis C virus (HCV) infection and alcohol now represent the commonest indications for liver transplantation both in Europe and North America (table 1).
Alcoholic liver disease (ALD)
ALD remains a controversial indication for liver transplantation and adverse publicity surrounding selected high profile cases can impact on organ donation. None the less, both short and long term outcomes in those transplanted for ALD are similar to those seen in patients transplanted for other causes of cirrhosis, with respect to survival and quality of life. However, this simplistic analysis takes no account of case mix (see box 1).
Box 1 Alcoholic liver disease
-
Alcoholic liver disease remains a good indications for liver transplantation with survival similar to those for other indications.
-
Indications for transplantation need refining as estimated short term gain is small.
-
The role of transplantation for alcoholic hepatitis is uncertain.
-
Transplantation is not indicated in those who are likely to return to a pattern of drinking that will either result in graft damage or lead to non-compliance.
-
The number of reported cases of graft damage or loss associated with a return to alcohol is small.
-
Potential candidates need to be assessed by a multidisciplinary team.
-
A fixed period of abstinence is not indicated but there should be a period of stable abstinence.
-
Extrahepatic alcohol induced organ damage may preclude liver transplantation.
-
Abstinence should be recommended after transplantation.
The major issues with respect to alcohol centre on whether the patient will return to a pattern of drinking after transplantation that will lead to graft damage and/or to non-compliance. Available data suggest that while many patients grafted for ALD do return to some pattern of alcohol consumption, less than 5% damage their graft.4,5
There remains controversy about the need for and duration of abstinence pre-transplant. There is no good evidence suggesting that a fixed period of abstinence (such as six months) will help identify those at risk of subsequent relapse. However, a period of abstinence allows time
-
to identify those patients whose liver function will improve to an extent transplantation is no longer indicated (about 10% referrals in our centre);
-
to identify reasons for excess alcohol consumptions and put in place measures to ensure abstinence post-transplantation.
Most centres advise strict abstinence post-transplant as it is difficult to identify in advance those who can effectively return to a pattern of controlled drinking. Monitoring of patients, pre and post liver transplantation for alcohol consumption, is difficult: measurements of blood, urine, or breath alcohol will identify those who have drunk recently; the value of carbohydrate deficient transferrin in identifying those who continue to drink alcohol remains uncertain.
Alcoholic hepatitis
It still remains uncertain whether liver transplantation is an appropriate therapy for those who present with alcoholic hepatitis: such patients are often very sick with renal failure and malnutrition. There is rarely time to assess fully the likelihood for further abstinence. Initial studies showed a poor outcome after transplantation but some more recent studies suggested that good survival can be achieved. Since indications and contraindications are not well defined in this group, a prospective trial has been advocated but may prove difficult to set up.6
Viral hepatitis
Hepatitis B viral infection (HBV)
Historically, those with evidence of active viral replication were not considered as liver transplant candidates because of the high risk of viral damage to the graft; those with no replication could be successfully grafted with the risk of graft infection greatly reduced by the use of hepatitis B immunoglobulin (HBIg). Introduction of effective antiviral treatments has allowed successful transplantation of HBV infected patients. Currently there are three approaches to prevention of graft infection.7
-
Lamuvidine monotherapy: given before and after transplantation is associated with inhibition of viral replication and prevention of graft damage and loss, but viral breakthrough may occur; this is more likely when the pretreatment viral load is high.
-
HBIg monotherapy: for those with HBV infection but without replication, post-transplant treatment has been with immunoglobulin, given to maintain antibody levels above 100–500 IU/l. The duration of treatment and level of antibody required to maintain freedom from recurrence is uncertain. At present, many centres use immunoglobulin long term, others for just one year or until viral breakthrough develops.
-
Combination therapy: a combination of HBIg and lamivudine increases the freedom from recurrence and is currently the management of choice, but even in those without evidence of recurrent disease HBV DNA may persist.8 However, because of the expense of HBIg, many centres are evaluating the effectiveness of discontinuation of HBIg after a few months and maintaining the patient on lamivudine monotherapy.
Viral breakthrough may occur in approximately 20% of patients taking lamivudine therapy, with resulting graft damage9; in such patients newer antiviral agents such as adefovir and entecavir are effective in inhibiting viral replication.10
Other approaches to prevent infection of the graft include the use of vaccination and adoptive transfer of immunity. The latter has been reported to occur when the donor is immune to the virus.11 While this may offer an effective therapy, especially in living donors who can be pretreated, more work is required to confirm the clinical significance of this observation.
Hepatitis C viral infection (HCV)
Recurrence of HCV after liver transplantation is almost universal but the natural history of recurrent disease is highly variable and accelerated compared with HCV in the native liver; indeed, cirrhosis may develop within one year of transplantation. Characteristics of recurrent HCV infection of the graft are shown in box 2. The rate of development of graft damage is greater in those grafted more recently; the reasons for this phenomenon are not clear but may relate in part to increasing donor age and greater use of split livers. Identification of those factors associated with recurrence may lead to development of strategies to reduce the impact of recurrence: avoidance of rejection is important as treatment of rejection is associated with an increased level of viral RNA, although more potent immunosuppressive agents (such as mycophenolate) are associated with an increased rate of fibrosis.12 Antiviral treatment pre-transplant to reduce the viral load is of some benefit.
Box 2 Characteristics of HCV reinfection
-
Average time to graft cirrhosis 9–12 years.
-
Decompensation occurs in up to 50% within one year of onset of cirrhosis.
-
Levels of HCV RNA rise after transplantation.
-
Risk factors for HCV recurrence:
-
HCV RNA levels pre-transplant;
-
episodes of acute rejection;
-
donor age;
-
use of more potent immunosuppressive drugs;
-
use of corticosteroids and OKT3;
-
year of transplant.
-
-
Factors possibly associated with recurrence:
genotype 1b;
split or living donor grafts.
-
Treatment: pre-emptive or as required.
Following transplant, treatment may be pre-emptive or when significant hepatitis occurs. Preliminary data suggest that pre-emptive treatment is less effective. Treatment with interferon and ribavirin is associated with viral clearance in about one third of patients.13,14 However, there is a significant rate of withdrawal from treatment due to toxicity. Erythropoetin and GCSF are often required to counter bone marrow suppression. Most centres are now using pegylated interferon with ribavirin. The cost of treatment is relatively high: an estimate based on Markov modelling in the US is $29 100 per life year saved.15
Human immunodeficiency virus (HIV)
The introduction of HAART (highly effective antiretroviral therapy) is associated with increased survival in HIV infected patients; many patients die from end stage liver disease associated with HCV or HBV. HIV coinfection appears to accelerate the rate of progression of viral hepatitis. Outcomes in HIV infected patients who have had a satisfactory response to HAART have suggested that liver transplantation is now a therapeutic option and some centres are now accepting HIV infected patients for consideration of transplantation (see box 3).16,17 Although indications will vary, most centres have adopted criteria similar to those shown below:
-
end-stage liver disease;
-
low or undetectable levels of HIV RNA;
-
CD4 count >200/ml;
-
no AIDS defining conditions.
Box 3 Issues surrounding HIV and liver transplantation (from Samuel et al16)
-
HAART has revolutionised the natural history of HIV infection.
-
Orthotopic liver transplantation is indicated in some people with HIV infection.
-
While short term outcomes are good, long term outcomes are unknown.
-
Optimal timing remains uncertain.
-
Some authors have suggested worse outcomes in HCV coinfected patients compared with HBV coinfected patients.
-
Polypharmacy associated with HIV, immunosuppression, and prevention of infection will increase the risk of non-compliance.
-
There is a potential for adverse drug interaction (such as ribavirin may increase HAART associated mitochondrial toxicity; HAART strongly inhibits CNI metabolism).
As many of the drugs associated with HAART are potent enzyme inhibitors, the dose of calcineurin inhibitor required to maintain adequate immunosuppression is usually very low, with many patients requiring treatment just once a week.
Liver cancer
Hepatocellular carcinoma (HCC)
The therapeutic options for patients with HCC are increasing (chemotherapy, resection, transarterial chemoembolisation, percutaneous ethanol injection, radiofrequency ablation, cryotherapy, gene therapy) and the outcomes associated with these therapies has led to a reconsideration of transplantation as the optimal therapy.18 The benefits of different strategies will depend on the general health of the patient, the cause and severity of underlying liver disease, the number and size of identified lesions, the absence of vascular invasion and extrahepatic spread, and the length of time awaiting a graft.
Hitherto, transplantation was indicated in those who met the Mazzaferro19 criteria:
-
single tumours measuring less than 5 cm or less (on ultrasound examination of the patient); or
-
fewer than three nodules measuring less than 3 cm in size.
More recently, the group from San Francisco have suggested that the indications should be widened to include a single lesion ⩽6.5 cm in diameter, three or fewer lesions none greater than 3 cm in diameter, or a total tumour diameter ⩽8 cm.20
There have been few randomised controlled studies assessing the various approaches to treatment. Di Carlis and colleagues21 compared outcomes in 154 liver resections with 121 liver transplants, performed between 1985 and 1999: five and 10 year survival was better in the transplant group (62% and 60% for orthotopic liver transplantation and 47% and 28% for liver resection, respectively (p = 0.08); disease free survival at both time points was statistically significantly better for transplantation). In contrast, Shabahang and colleagues22 found no statistically significant difference in either overall survival or disease free survival at 36 months in Child A patients with HCC who underwent resection or transplantation.
Adjuvant therapies have been assessed in the context of observational studies, and controlled prospective studies are needed to determine the extent of any benefit in combination with transplantation.23 It remains to be shown whether procedures that down-size a tumour to meet the accepted criteria for untreated tumours will allow for effective use of liver transplantation. Introduction of the MELD system of allocation of donor organs in the USA has reduced the waiting time for those with liver cancer and this reduced wait has been associated with improved survival.
Cholangiocarcinoma
Pre-transplant diagnosis remains difficult. Cholangiocarcinoma is considered an absolute contraindication for liver transplantation in most centres: early spread along nerves and lymphatics mean that curative treatment is rarely possible and long term outcomes after transplantation are poor. However, a recent analysis from the Mayo Clinic24 has shown that an aggressive approach using a combination of chemotherapy, brachytherapy, and laparotomy can identify a small proportion of patients who will benefit from liver transplant.
Early diagnosis of cholangiocarcinoma may allow effective use of transplantation: serum markers of cholangiocarcinoma are not sufficiently accurate for clinical use. It has been suggested that biliary cell dysplasia is a reliable marker for cholangiocarcinoma25; further work is required to confirm this association and to determine if the presence of dysplasia might be an indication for transplantation.
THE DONOR SHORTAGE
The major factor limiting the availability of transplantation is the shortage of donor livers, so not all patients who could benefit from the procedure can receive a graft; not all patients who might benefit from liver transplantation are referred to transplant centres.
The gap between the number of donor organs and the number of potential recipients is widening: there are many causes for this.
-
Indications are increasing.
-
Surgical and anaesthetic advances have lessened contraindications.
-
The mortality from liver disease is increasing.
-
More patients are being referred as transplantation has become an accepted form of therapy.
Increasing organ donation
Organ donation varies between countries, and the potential for cadaveric organs is not exhausted (table 2). Evidence from Spain and more recently in Italy and the UK has shown that increasing resources to provide trained donor coordinators will increase organ donation.26
Organ donation and transplant activity in Europe in 2002 (data taken from UK Transplant (www.uktransplant.org.uk)
Greater use of cadaveric organs
A variety of approaches have been adopted to increase organ use.
-
Extending the use of marginal livers: not all organs that are offered for transplantation are accepted because of concerns as to whether the graft will function adequately or the graft may transmit infection or malignancy to the recipient. For example, transplantation of a graft from a donor who is hepatitis B core antibody positive may lead to graft dysfunction but use of antiviral agents may minimise this effect and so allow this source of livers to be used.27 Good outcomes have been reported with the use of livers from HCV positive donors for HCV infected recipients.28 It may be possible to use safely organs from donors with non-melanoma skin cancers and with some brain tumours.29,30 Better understanding of the factors that identify a marginal liver and improved management of the donor and graft will help reduce the rate of primary non-function.
-
Split-liver, where one liver is split and used for two recipients.
-
Domino liver transplantation: an example is where a patient with familial amyloid polyneuropathy is grafted to halt progression and palliate associated symptoms, and the otherwise normal liver is used for selected recipients.31
-
Non-heart beating donors: these may be controlled or non-controlled. Many centres have abandoned the use of non-controlled donors (where death occurs outside a controlled situation) as the prolonged ischaemic time is associated with a high level of graft problems. Controlled non-heart beating donors (where death occurs in a hospital setting) can provide a source of donor livers. With increasing experience, criteria for such donors are being developed32 and outcomes are good although there is an increased risk of biliary complications.33
-
Reduced liver: reduction of the size of the graft, while not increasing the donor pool, allows children and small adults access to a larger pool of organs.
Living liver donation
Living organ donation was introduced by Raia, Strong, Broelsch, and others in 1989 and has been widely adopted, not only in the Far East where cadaveric donors are few but also in Europe and North America.34–36 Initially, the left lobe was used but as understanding of the anatomy of the liver increased, it became possible safely to transplant the right lobe. It is important to ensure an appropriate volume of liver for both donor and recipient. The ethics of living liver donation have been widely discussed and have largely focused on the morbidity and mortality of the procedure. For right lobe donation, the donor mortality is approximately 0.5–1% and morbidity around 25%. For left lobe donation, the risks to the donor are significantly less. There is no doubt that living liver donation has advantages for the recipient: mortality on the waiting list has fallen, the procedure can be planned, be done before the patient deteriorates, and ischaemia times kept to a minimum. Not all recipients have suitable donors.
Donor shortage and recipient listing
There are several approaches to listing and organ allocation: for example, in the USA, organs are allocated primarily to the patient, according to priority as assessed by the MELD (model for end stage disease) or PELD (pediatric end stage disease model) score35,37; the score is assessed using objective laboratory measures with adjustment being made for the presence of cancer. As a consequence, the waiting list mortality in the USA has fallen. In the UK, where patients are listed if they meet the indications for transplantation and are estimated to have a more than 50% probability of survival after transplantation with a quality of life acceptable to the patient, organs are allocated to the centre.38 This allows the centre to match better the donor organ and the recipient. This approach restricts transplantation to those who are most likely to benefit from the procedure: but the emphasis of utility rather than equity has ethical issues. Whatever method is adopted, the procedures should be transparent and agreed after full public debate.
To make effective use of the donor livers available, it is important to identify risk factors so that selection can be optimised. Mortality risk factors were evaluated in 22 089 liver allograft recipients listed in the European Liver Transplant Registry.39 The risk factors identified are shown in table 3.
Risk factors for mortality after liver transplantation (from European Liver Transplant Registry39)
MANAGEMENT ON THE LIST
Management of the liver transplant candidate while awaiting liver transplantation is little different from that of the patient with chronic liver disease. This period does allow for immunisation with hepatitis B vaccines to reduce the small risk of acquisition of B viral infection with the graft. Nutrition needs to be maintained with oral or even nasogastric supplements if required. The consequences of portal hypertension and cirrhosis screened for and prophylaxis introduced where indicated, for prevention of spontaneous bacterial peritonitis, variceal bleeding, HCC development, or progression and portal vein thrombosis.
Transjugular intrahepatic portosystemic shunts (TIPS) are being used increasingly in the management of intractable ascites, hepatic hydrothorax, hepatorenal syndrome, and variceal bleeding. While the use of TIPS is associated with a reduction in portal hypertension, complications such as occlusion and placement of the stent at the site of potential anastomoses may add to the problems of surgery. Overall, a stent does not impact significantly on the course of liver transplant surgery; the use of TIPS should be when clinically indicated; a stent may provide a bridge to transplantation in selected patients but there is no indication for its use solely to reduce portal hypertension.40
The molecular adsorbents recycling systems based on albumin dialysis may have a place in maintaining liver function in those with severely decompensated liver disease and fulminant hepatic failure.41 Preliminary results suggest that this approach may help in stabilising the patient while awaiting a liver.
POST-TRANSPLANT MANAGEMENT
Management of the patient post-transplant requires collaboration between the recipient, the transplant centre, and the local clinicians.
Immunosuppression
Immunosuppressive agents
An increasing number of immunosuppressive agents are being introduced into clinical practice which provides the clinician with exciting opportunities to tailor immunosuppression for the individual.
Drugs currently licensed for treatment in liver transplantation
Calcineurin inhibitors
The two calcineurin inhibitors (CNIs) in current use are tacrolimus and cyclosporin. These are the mainstay of immunosuppression. Usually, doses are titrated according to trough blood levels. More recently, C2 monitoring (changing the dose of cyclosporin to achieve a target concentration two hours post dose rather than trough levels (C0)) has been suggested as a more effective method of titrating the dose.42
Mycophenolate mofetil
A well established drug, this is now used increasingly in place of azathioprine. Unlike azathioprine, mycophenolate is not metabolised by thiopurine methytransferase. The main side effects are gastrointestinal upset and bone marrow suppression. It is licensed for use with other agents, not as monotherapy, and is not indicated in pregnancy. As it may take several days to achieve therapeutic levels with oral medication, intravenous use should be considered if the drug is introduced early. Most centres do not measure trough levels routinely. Mycophenolate is well tolerated in both acute and chronic rejection and helps reduce the adverse effects of the CNIs.
Sirolimus and everolimus
Sirolimus acts through a signal transduction pathway, distinct from that used by cyclosporin and tacrolimus. In addition to its antiproliferative effects, it has in vitro effects which may be of clinical relevance: the drug inhibits fibrosis and fibroblast proliferation. It is also antineoplastic and inhibits CMV replication. Whether these effects are relevant in vivo remains to be confirmed. Initial studies suggested that its early use was associated with a high risk of hepatic artery thrombosis but this has not been confirmed in subsequent studies. Other significant side effects include its association with hyperlipidaemia and impaired wound healing.44–46 Everolimus is related to but structurally similar to sirolimus.
IL-2 receptor antibody blockade
Two monoclonal antibody preparations to the interleukin 2 (IL-2) receptor have been introduced: dacluzimab and basiliximab. The former is a humanised monoclonal antibody and the latter a chimeric antibody. Both antibodies are effective in reducing acute rejection in renal transplantation but the evidence for liver transplantation is less clear.47 None the less, these agents are safe and well tolerated; they are being used increasingly and may be of particular benefit in those with pre-transplant renal impairment to allow either delayed introduction or lower doses of CNIs.
Drugs available but not licensed for use in liver transplantation
Leflunomide
Leflunomide is now used in the treatment of rheumatoid arthritis where it has a synergy with CNIs. It appears to be well tolerated in liver allograft recipients; anaemia and liver damage have been reported especially in the first six months of use.48 It has a long half life so monitoring will be important but a short lived derivative is currently being assessed. Its use is contraindicated in pregnancy.
Alemtuzumab (Campath-1H)
Licensed for use in some forms of chronic lymphatic leukaemia, the antibody has been used as part of a conditioning regimen.49
Drugs not yet licensed
FTY720 is a novel synthetic immunosuppressive drug50 that induces a reduction in the peripheral lymphocyte count by increasing homing to lymphatic tissues and apoptotic T cell death.
Immunosuppressive strategies
Initial regimens for immunosuppression were extrapolated from experience in renal transplantation and focused on a heavy induction regimen to prevent early acute allograft rejection. With the realisation that in the liver allograft recipient (in contrast with the kidney graft) early acute rejection may not only be unimportant but may be associated with better graft outcome than no rejection (HCV infected patients is an important exception as increased immunosuppression for the treatment of rejection is associated with greatly enhanced viral replication), these strategies have been revised.
Calne51 has suggested that early immunological engagement may help tolerance and so introduced his concept of a window for immunological engagement. Preliminary results using less immunosuppression in renal grafts are reported to be encouraging: Starzl and colleagues52 used a regimen of early treatment with ATG and tacrolimus given at increasingly long intervals. Preliminary outcomes in patients given a variety of solid organ grafts are reported as good with tacrolimus given up to once a week. Others have shown in living donor liver recipients that immunosuppression can be given up to once weekly or withdrawn entirely.53 These findings need confirmation.
Current immunosuppressive regimens
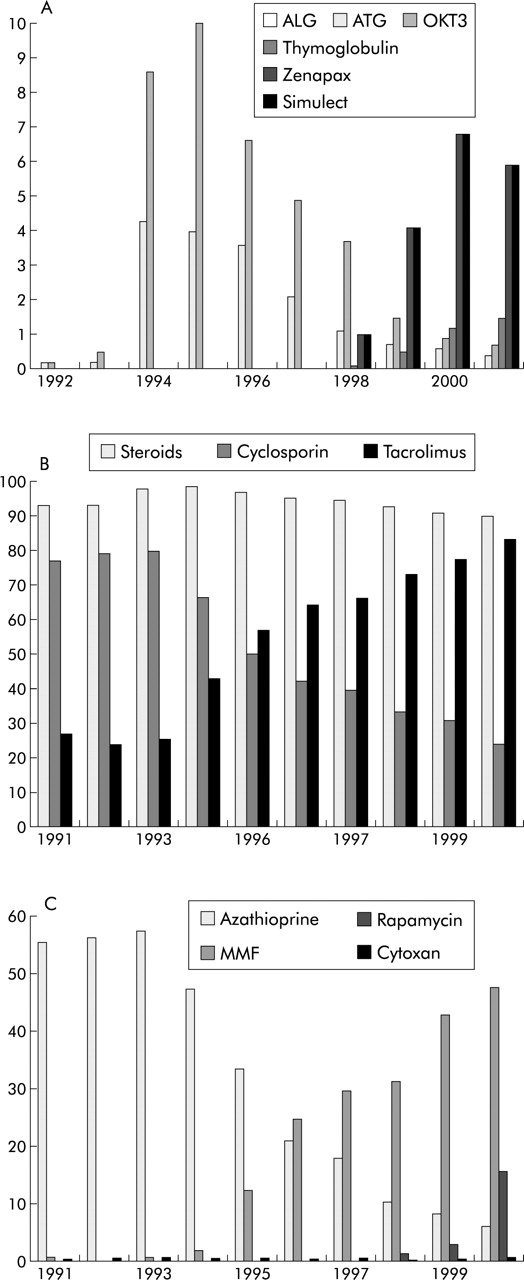
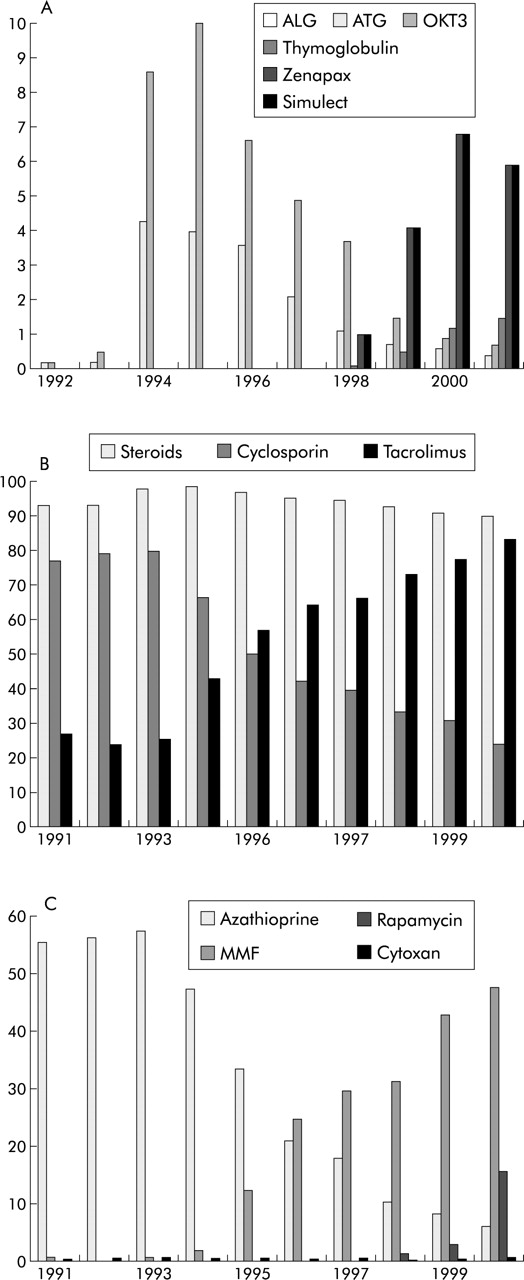
In North America, the pattern of immunosuppression has changed over the last decade (fig 1).37 No such data are available for Europe but personal impression suggests the majority of transplant units use triple immunosuppression with a CNI (usually tacrolimus), corticosteroids, and azathioprine.
{kind=link}
Immunosuppressive therapy in liver transplant recipients (data from UNOS).37 (A) Induction therapy. (B) Maintenance immunosuppression. (C) Other immunosuppressive agents.
Induction therapy
Induction therapy with antilymphocyte preparations (such as OKT3 or ATG) is used less frequently. Trends in North America show that the use of IL-2 receptor antibodies is increasing
Maintenance therapy
More centres are using mycophenolate in place of azathioprine. Increasingly, centres are withdrawing corticosteroids during the first postoperative year; some centres are using steroid free regimens. Those grafted for autoimmune hepatitis may require long term steroids. There remains uncertainty whether patients can be maintained safely on monotherapy with mycophenolate.
Tacrolimus or cyclosporin? There remains debate about the most appropriate CNI to use. A recent study comparing tacrolimus with microemulsified cyclosporin found that the primary outcome (death, retransplantation, treatment failure for immunological reasons) was reached more in the cyclosporin treated group than the tacrolimus treated group (32% and 21%); the main causes of death (sepsis and multiple organ failure) were similar in both groups but the incidence of hepatic artery thrombosis was greater in the cyclosporin treated group.54 Whether these conclusions can be extrapolated to the use of C2 monitoring is unclear.
Treatment withdrawal
From the 1990s, it became clear that not all liver allograft recipients require long term immunosuppression. Mazariegos and colleagues55 showed that 19% of 95 patients could be safely weaned off immunosuppression. Chimerism is not associated with the probability of successful weaning. Features suggesting the possible option of treatment withdrawal include55,56:
-
transplantation for non-immune mediated disease;
-
fewer HLA A, B, and DR mismatch;
-
low incidence of early acute rejection;
-
no evidence of graft hepatitis at five years.
However, there remain concerns in many units about the safety of immunosuppression withdrawal and most centres maintain life long immunosuppression.
SURVIVAL AFTER TRANSPLANTATION
Causes of late death after transplantation are due to either graft-related problems (primarily recurrent disease) or non-graft related problems; about two thirds of these are due either to cardiovascular disease or malignancy
Premature death
The major causes of late death after transplantation will vary according to the age and indication, but most series report broadly similar findings.57–59
Graft related
Approximately 50% of late deaths are graft related: these are mainly recurrent disease (especially HCV). Chronic rejection is now rarely seen and vascular complications are uncommon after the first year.
Extrahepatic
These are predominantly vascular (cardiac and cerebrovascular); malignancy accounts for about one third. Renal failure and infections are significant causes for premature death
Medical problems need monitoring after transplantation60
Obesity is common after liver transplantation, affecting over 60% of recipients. Obesity usually develops within the first year and is not related specifically to any one immunosuppressive agent.
Hyperlipidaemia may be related to use of CNI, steroids, and sirolimus. Increased blood cholesterol and triglycerides are seen in up to 40% recipients and should be treated with diet and medication. There is a potential for interaction between cyclosporin and the statins and there is an increased risk of myopathy.
Hypertension is common, affecting up to 70% of patients and is related to immunosuppression and renal impairment. Thiazides are usually ineffective and ACE inhibitors or calcium channel antagonists are the treatments of choice.
Bone disease: osteopenia is common in those with end stage disease; after initial loss, bone mass usually improves. In those with osteopenia, early steroid withdrawal is important together with conventional measures to retard bone loss.
Renal impairment: late renal failure is being recognised as a major cause of morbidity and mortality after liver transplantation. The cumulative risk of renal failure approaches 10% at 10 years.61,62 Although there are many potential causes of renal impairment in the allograft recipient, use of CNI is a major factor. Late renal failure can be predicted by estimations of renal function in the first year and are related to dose and levels of the calcineurin inhibitor during the first 6–12 months after transplantation. There is no apparent difference between cyclosporin and tacrolimus with respect to their nephrotoxic potential. Hypertension should be treated aggressively and nephrotoxic drugs avoided; use of CNIs should be minimised during the first year, possibly by concomitant use of other agents. Early recognition of the potential renal failure should prompt consideration of alternative strategies before the onset of irreversible damage. Substitution of CNIs with mycophenolate or sirolimus may be associated with an improvement or stabilisation of renal function and blood pressure but monotherapy is associated with the risk of acute and chronic graft rejection.63–65 Therapeutic studies are underway as to the optimal management of post-transplant nephrotoxicity.
Post-transplant lymphoproliferative disease (PTLD): PTLD may complicate the outcome of approximately 2% liver allograft recipients within 10 years of transplant. Over half may occur in the first year and may be of donor origin. These are often associated with Epstein-Barr virus infection and often present atypically, with extranodal and hepatic involvement being common. Risk factors include excessive immunosuppression and heavy induction regimens and de novo Epstein-Barr virus infection. Treatment needs to be aggressive, with reduction or even cessation of immunosuppression, introduction of antiviral therapy, antilymphoma treatment with chemotherapy, and Rituximab (anti-CD20 monoclonal antibody). Withdrawal of immunosuppression may lead to acute or chronic rejection and graft loss.
Adolescents
The increasing survival of children receiving liver transplants has meant that more children are surviving into adulthood and will require transfer to an adult unit. Problems, such as non-compliance, are commonly encountered. Adolescence, never an easy time, is hard for liver allograft recipients and most units have introduced handover clinics.
Quality of life after liver transplantation
Several studies have addressed the issues of quality of life following transplantation. Within the first year after transplant, there is dramatic improvement in the quality of life in all five domains (measure of disease, psychological distress, personal and social function, and general health perception); although psychological distress associated with obesity increased, levels of assessment were close but not identical to the normal population.66–68 Many female liver allograft recipients have normal pregnancies, despite the use of immunosuppression, although low birth weight and preterm delivery are more common.69 Some immunosuppressive agents should be avoided and breast feeding is usually not advised.
Cost effectiveness
Comparisons between studies are not simple as different methodologies are used, different health care systems have different costs, and there is not always a clear differentiation between costs and charges. Costs will change with survival as many of the costs (candidacy and early postoperative period) will be greatest in the first year. Furthermore, costs will change with time and with the success and size of the programme.
In the Netherlands, Ouwens and colleagues70 estimated that the follow up costs of liver transplantation in the first three years was $95 300 and, with a survival gain of 14.7 years, the cost per life year gained was $26 000. Filipponi and colleagues71 estimated that in Italy the average cost per patient alive ranged between €107 000 and 118 000, and the average cost per transplant lay between €75 747 and €83 846. Similar findings were reported from Canada where the overall mean cost of liver transplantation was estimated to be Can$89 066.72 In the UK, a recent study showed that the mean incremental cost per QALY from the time of listing varied were £21 000, £29 000, and £48 000 for patients grafted for primary biliary cirrhosis, primary sclerosing cholangitis, and alcoholic liver disease, respectively. The higher cost for patients grafted for ALD reflects in part the greater number of patients assessed for transplantation but not transplanted.73 Donor acquisition fees are about £7000 in the UK, compared with $5k to $65k in the USA. In Switzerland, Sagmeister and colleagues74 estimated costs per QALY of €22 451 for cadaveric liver transplantation and of €23 530 for living liver donation.
Recurrent non-viral disease (table 4)
Some recurrent diseases after transplantation
Recognising recurrent disease in the allograft may be difficult because conventional diagnostic criteria may not apply; and the clinical, serological, and histological features and the natural history may be modified by concurrent immunosuppression and by the mismatched host/graft immune environment. Recognition and early intervention for reduction in risk factors for vascular disease may help reduce this risk.
Autoimmune hepatitis
Recurrent AIH may develop in up to 30% of patients grafted for AIH: treatment with increased corticosteroids is usually but not invariably effective in treating the hepatic inflammation75 Of note, evidence of recurrence may be first detected more than 10 years after transplantation and histological changes may precede the biochemical abnormalities, suggesting that protocol liver biopsies should be done regardless of biochemistry.76 Because of the consequences of recurrent AIH, many centres now use corticosteroids for at least the first year.
De novo autoimmune hepatitis
Graft hepatitis with features of autoimmune processes (such as raised serum transaminases, elevated immunoglobulins, and autoantibodies) may develop in allograft recipients transplanted for non-autoimmune indications. This syndrome develops in approximately 1% adults and 4% children. There is usually, but not always, a good response to steroids. A recent report77 of de novo autoimmune hepatitis affecting an auxiliary partial graft and not the native liver adds additional support to the concept that de novo hepatitis is a variant of rejection.
Primary biliary cirrhosis
Evidence of histological recurrence of PBC is found in approximately 35% of patients at 10 years.78 It is rare that cirrhosis develops and the effect on graft survival is small. Whether ursodeoxycholic acid affects rates of progression is not known. We have found that immunosuppression with tacrolimus compared with cyclosporin is associated with more rapid progression.
Primary sclerosing cholangitis
The diagnosis of recurrent PSC is difficult to make as it can be difficult to distinguish recurrent PSC from secondary sclerosing cholangitis. Secondary sclerosing cholangitis which is associated with:
-
prolonged ischaemic times,
-
ABO incompatibility,
-
bacterial or viral cholangitis,
-
hepatic artery thrombosis
-
rejection.
The diagnosis is made on imaging the biliary tree or finding characteristic histological features of PSC (such as fibro-obliterative lesions) on histology, in the absence of other causes of sclerosing cholangitis. Recurrent PSC is thought to occur in approximately 50% of patients at five years after transplant and leads to graft loss in 10%.79 The only risk factor identified to date is colectomy (before or during transplantation appears to protect against recurrence).80
FUTURE DEVELOPMENTS
Ideally, medical treatments will become effective and so liver transplantation will become redundant. New strategies to replace organ transplantation are being developed but remain some years away from introduction into clinical practice.
Xenotransplantation is still banned in humans; while the introduction of genetically modified pigs has overcome some of the problems of hyperacute rejection, there are many problems to be overcome before this technology can be transferred into the clinical arena.81 Baboon to human liver transplantation has been done with initial success.82
Stem cell technology in time may provide an alternative to organ transplantation.83
Isolated hepatocytes transplantation has been used to treat metabolic defects such as urea cycle disorders. Cells can be isolated readily from donor livers considered unsuitable for organ transplantation, and can be infused repeatedly.84,85 Such an approach can also be used for gene therapy.86