Article Text

Statistics from Altmetric.com
Vandeputte et al 1 recently reported a strong effect of stool consistency—as measured by the Bristol Stool Scale (BSS)—on the composition of the gut microbiota in 53 healthy females. This work potentially has a large impact on future microbiome studies as it suggests that such studies may need to be corrected for BSS scores. However, the generalisability of their study is not immediately evident as it did not include a replication cohort and was limited to females aged 20–55 years.
We analysed gut microbiota in relation to BSS in LifeLines-DEEP, a large population-based cohort.2 From 1126 LifeLines-DEEP participants, with both males (n=454) and females (n=672) aged 18–81 years (table 1), the BSS score was recorded for seven consecutive days and a fresh-frozen stool sample was collected in the same week. We calculated the average stool type of 7-day records for each participant. Stool DNA was isolated using AllPrep DNA/RNA Mini Kit (Qiagen; cat. #80204), and subsequently we performed 16s rRNA gene sequencing using forward primer 515F (GTGCCAGCMGCCGCGGTAA) and reverse primer 806R (GGAC TACHVGGGTWTCTAAT), similar to the study by Vandeputte et al.1 As a reference for operational taxonomic unit (OTU) picking and taxonomy annotation, we used a primer-specific version of GreenGenes 13.8, as described previously.3 The association analysis of microbiota to BSS was corrected for sequence depth, age, gender, body mass index (BMI) and drugs that evoke an effect on the microbiome (ie, antibiotics and proton pump inhibitors).
Baseline characteristics of the LifeLines-DEEP participants, including their BSS scores
The mean BSS score in our study population was 3.9 (range 1–6.5), including 69 (6.1%) participants who generally displayed a hard stool pattern (BSS<2.5) and 30 (2.7%) participants with a generally loose stool pattern (BSS≥5.5) (table 1). We identified a total of 208 bacterial taxa.
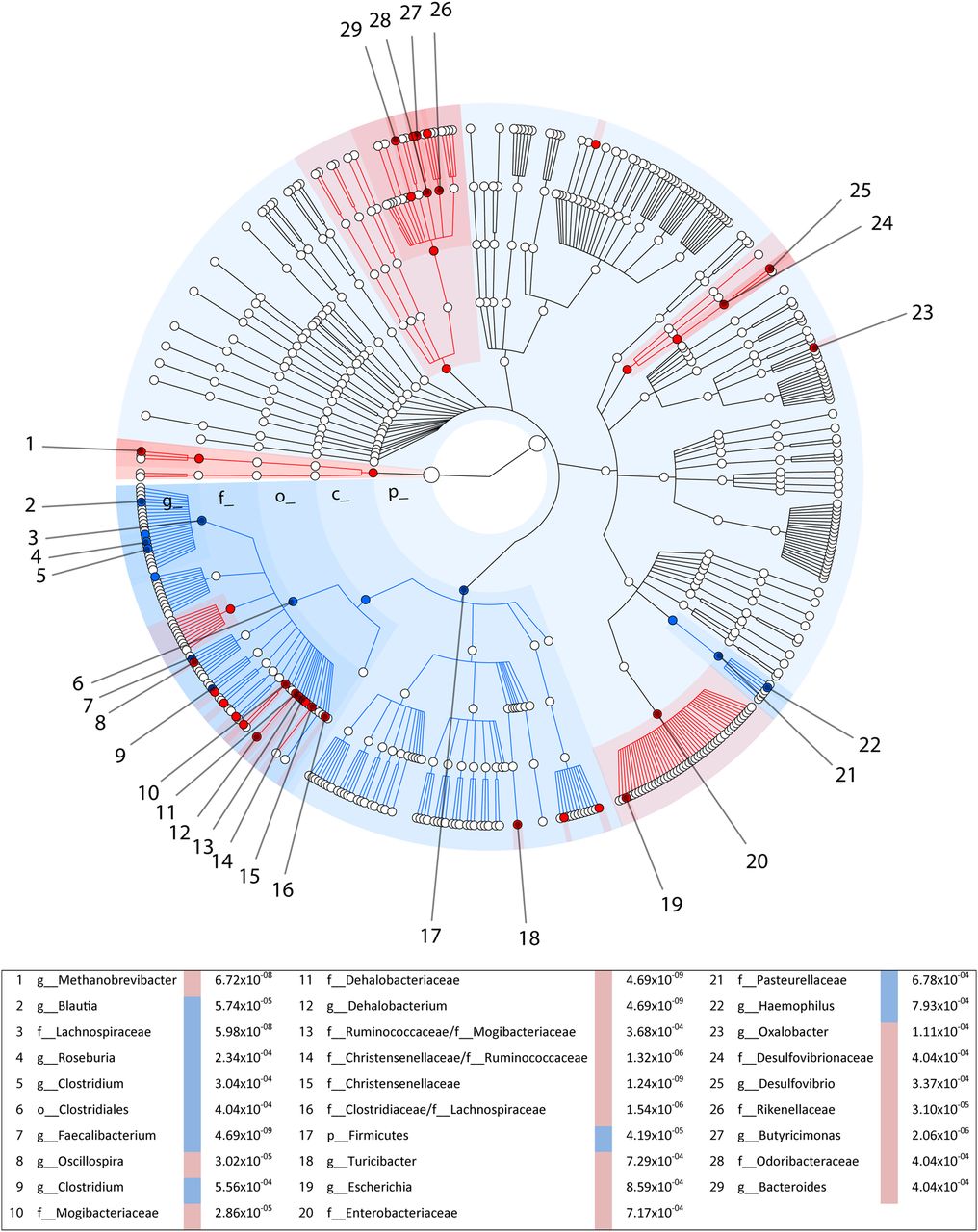
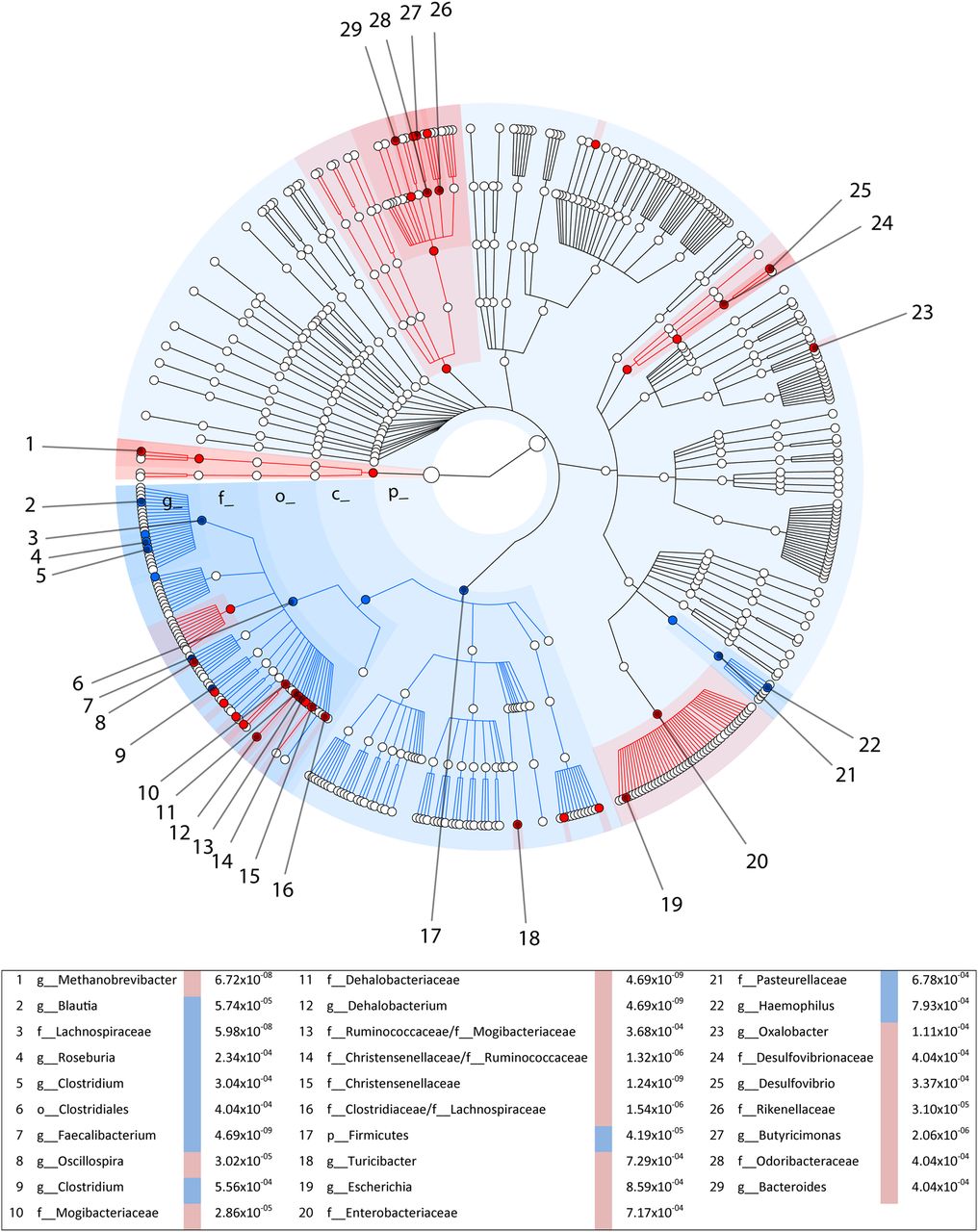
In contrast to Vandeputte et al, we did not find a significant correlation of BSS and observed species richness (Spearman's r=−0.01, p=0.85), however, we did observe significant associations (q<0.05) of stool consistency with 67 intestinal bacteria (figure 1). We also found a similar though less strong association of stool type with the Firmicutes:Bacteroidetes ratio (Spearman's r=−0.076, p=0.01). The highest positive correlations with an increasing BSS score were observed with Faecalibacterium prausnitzii (q=4.69×10−09) and the family Lachnospiraceae (q=5.98×10−08), whereas two members of the Clostridia class (Christensenellaceae, q=1.24×10−9 and Dehalobacteriaceae, q=4.69×10−09) and the Archaea kingdom (q=6.72×10−08) were most significantly associated with a decreasing BSS score (ie, with harder stools). Many of these bacteria have previously been associated with various phenotypes, including the association of Christensenellaceae and Archaea with a lower BMI,4 and decreased abundance of F. prausnitzii in patients with IBD.5 Consistent with these findings, we observed a moderate but significant correlation of BMI with BSS type (Spearman's r=0.07, p=0.016).
{kind=link}
Bacteria significantly differentially associated with stool consistency. Background colours highlight the 67 bacteria with q<0.05; blue is positively correlated with looser stool consistency and red is negatively correlated with looser stool consistency. The numbers list the bacteria (q<0.001) up to genus level, the direction of the association and the q-values. Shells from the inside to the outside represent: p_, phylum, c_, class, o_, order, f_, family and g_, genus.
Vandeputte et al 1 reported a stronger correlation of BSS to microbiota composition in females. In our gender-specific analysis, we observed no heterogeneity between male and female samples (Cochran's Q p value for heterogeneity >0.01 for all of the 67 associated taxa), indicating that the majority of bacteria show similar correlations with BSS in males and females.
Like Vandeputte et al, we observed strong associations of stool consistency with microbiota composition, although we did not confirm their association of BSS with either microbial richness or gender differences. Our results were obtained in a large population cohort, including males and females and covering a wide age range. Our data do provide independent evidence for the association of BSS score with gut microbiota composition, and we thus underscore the importance of including information on BSS in future studies of gut microbiota.
Acknowledgments
We thank Arnau Vich for technical assistance and Jackie Senior for editing this letter.
Footnotes
Contributors CW, JF and AZ were involved in the conception and design of the study. EFT, MJB, SAJ, JF and AZ were involved in data collection, analysis and interpretation. EFT and AZ drafted the work. All authors have critically revised this letter and approved the final version to be published.
Funding This project was funded by a grant from the Top Institute Food and Nutrition, Wageningen (GH001) to CW and a Netherlands Organization for Scientific Research grant (NWO-VIDI 864.13.013) to JF. AZ holds a Rosalind Franklin Fellowship (University of Groningen).
Competing interests None declared.
Ethics approval The LifeLines-DEEP study was approved by the ethics committee of the University Medical Centre Groningen, document no. METC UMCG LLDEEP: M12.113965. All participants signed an informed consent form prior to study enrolment.
Provenance and peer review Not commissioned; internally peer reviewed.