Article Text

Statistics from Altmetric.com
We read with great interest the recent article by Lemoine et al,1 whereby a novel biochemical-based score was able to accurately estimate liver fibrosis among patients chronically infected with HBV in West Africa. The γ-glutamyl transpeptidase (GGT)-to-platelet ratio (GPR) has several attractive features, including parameters that are easy to quantify, a straightforward calculation, and more importantly, much lower cost than other non-invasive methods. Yet as the authors conclude, the GPR needs further evaluation in other patient populations and one of utmost importance in resource-limited settings would be those co-infected with HBV and HIV.2
We explored data from a previous validation study among HIV-HBV co-infected patients in which non-invasive biomarkers were used to predict liver fibrosis. From 2002 to 2005, a subset of patients from the French HIV-HBV Cohort underwent liver biopsies during follow-up, as detailed elsewhere.3 Of them, 95 without additional hepatitis C or D virus infection had available GPR, FibroTest (Biopredictive, Paris, France), aspartate transaminase-to-platelet ratio index (APRI), and fibrosis-4 (Fib-4) scores. Patients were a median 44 years old (IQR=39–48) and almost all male (93.7%). The overwhelming majority were antiretroviral (ARV)-experienced (95.8%) with 81 (85.3%) undergoing ARV-therapy at the time of biopsy. Accordingly, 36 (37.9%) exhibited detectable HIV-RNA (median=3.77 log10copies/mL, IQR=2.68–4.70) and median CD4+ cell count was at 409/mm3 (IQR=293–539). Hepatitis B ‘e’ antigen (HBeAg)-positive serology was observed in 75.6% of patients. Furthermore, 44.6% had detectable HBV-DNA (median HBV-DNA viral load=5.12 log10IU/mL, IQR=3.67–6.88), which was due mainly to lamivudine resistance and/or short duration of tenofovir-containing ARV-therapy.4
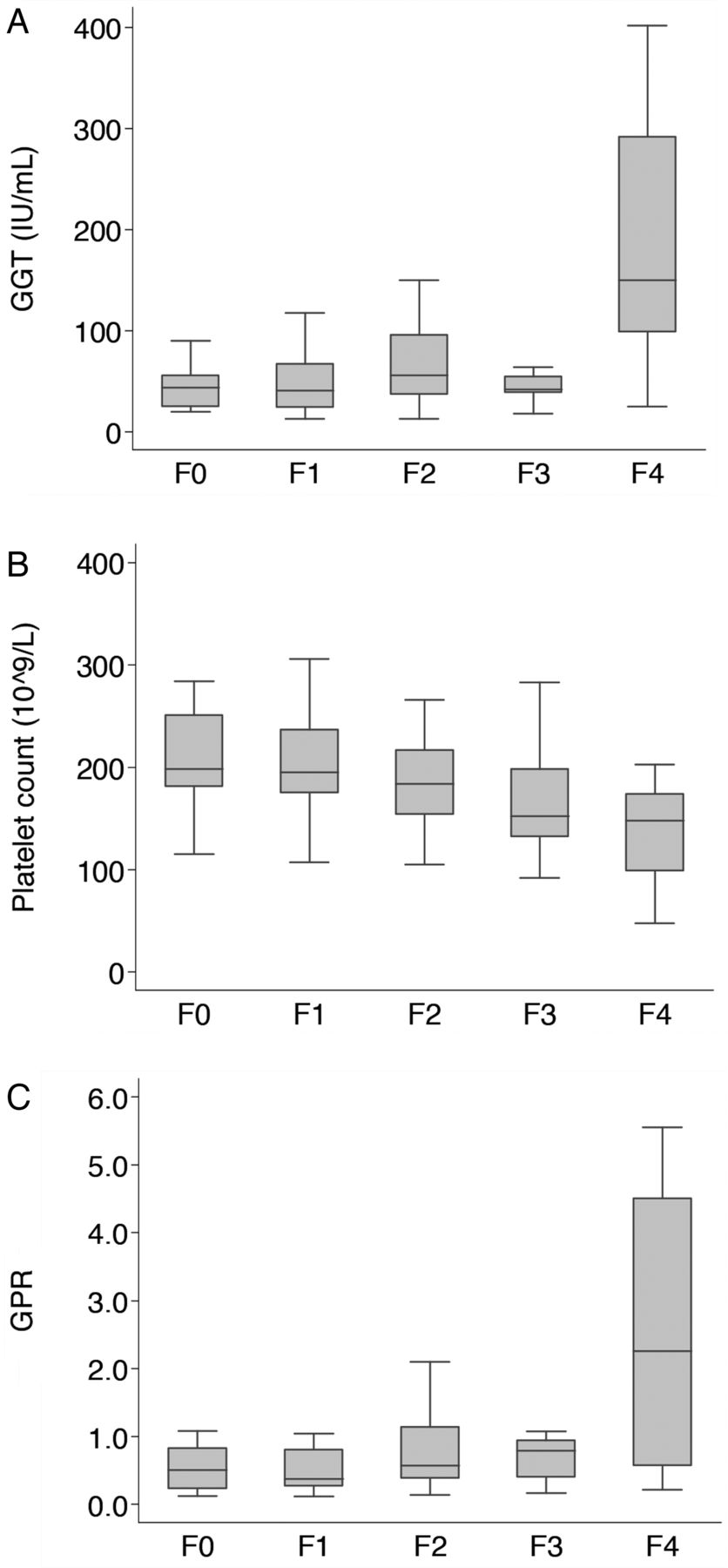
Median GGT and platelet counts were 45 IU/L (IQR=29–93) and 185 109/L (IQR=154–227), respectively, and biopsy-assessed liver fibrosis was distributed as follows: F0-F1, n=43; F2, n=26; F3, n=13; F4, n=13. Liver fibrosis significantly correlated with GGT (Spearman's ρ=0.32, p=0.002, figure 1A) and platelet count (Spearman's ρ=−0.38, p=0.0002, figure 1B), resulting in higher median GPR with increasing fibrosis (Spearman's ρ=0.38, p=0.0001, figure 1C). In multivariable analysis, both parameters were not significantly predictive of ≥F2 fibrosis, but rather ≥F3 fibrosis (GGT: adjusted-OR per times upper limit of normal=1.33, 95% CI 1.02 to 1.74; platelet: adjusted-OR per 109/L=0.98, 95% CI 0.97 to 0.99). After estimating the area under the receiving operator characteristic curve (AUROC) to predict ≥F3 fibrosis, no significant difference in performance of GPR (AUROC=0.709, 95% CI 0.583 to 0.835) was observed compared with the FibroTest (AUROC=0.826, 95% CI 0.724 to 0.929, p=0.13), APRI (AUROC=0.746, 95% CI 0.636 to 0.856, p=0.5) and Fib-4 scores (AUROC=0.754, 95% CI 0.635 to 0.873, p=0.5). As shown in table 1, performance of GPR improved when predicting higher levels of liver fibrosis, while most measures of accuracy followed closely with other non-invasive markers.
Diagnostic thresholds and performance of biochemical scores in HIV-HBV co-infected patients

{kind=link}
Levels of γ-glutamyl transpeptidase (GGT) (A), platelet count (B) and GGT-to-platelet ratio (GPR) (C) by stages of METAVIR liver fibrosis in HIV-HBV co-infected patients.
Clearly, the major caveat of using GPR to predict liver fibrosis in co-infected patients lies in the appropriate cut-off, which appears to be two to three times higher compared with HBV mono-infection.1 As GGT levels, and not platelet counts, were abnormally high overall, the need for modified thresholds would likely stem from elevated GGT. HIV-viral hepatitis co-infected patients tend to present with higher transaminase and GGT levels compared with either infection alone.5 ,6 The reasons for these increases are poorly understood for HIV-HBV co-infected patients in particular and worth further investigation. ARV-use has been implicated in elevated GGT and similar to previous studies,7 we noticed significantly higher GGT in patients undergoing treatment with non-nucleoside reverse transcriptase inhibitors (+61 IU/mL, 95% CI 29 to 94). Alternatively, excessive alcohol consumption and obesity could increase GGT; however, they were not frequent in our cohort (median g/day of alcohol intake=0, IQR=0–16; 3.5% with body mass index >30 kg/m2) making this an unlikely explanation.
Notwithstanding the small sample size and extensive ARV-experienced cohort, we validate that the GPR could be used as a non-invasive marker to predict liver fibrosis for HIV-HBV co-infected individuals, especially when compared with other measures. It should be mentioned that our treated co-infected study population, with higher prevalence of HBeAg-positivity and higher proportion of men, might not be fully representative of those in sub-Saharan Africa.8 When comparing patients of our study originating from a region of moderate or high HBV-endemicity, who share similar HBV characteristics observed in resource-limited settings, with other transmission risk-factor groups, we observed no difference in the distribution of GPR or fibrosis levels or predictive capacity of GPR. Nevertheless, we certainly hope that further evaluations will be conducted in sub-Saharan Africa or, more broadly, during effective antiviral treatment for mono-infected and co-infected patients.
Acknowledgments
The authors thank the patients and the clinical teams for their commitment to the French HIV-HBV Cohort Study. The authors also thank H Rougier, M Sébire-Le Cam, L Roguet for managing the logistics of the French HIV-HBV Cohort; G Pannetier and F Carrat for their help in the data management. The authors also thank Pr J-F Flejou and E Roux of the Tumorothèque HUEP at Saint-Antoine Hospital for storing samples.
Footnotes
Contributors AB and JB were responsible for data management, performed statistical analysis and drafted the manuscript. KL was responsible for oversight of the French HIV-HBV Cohort and provided critical edits of the manuscript. All authors approved the final version of the manuscript.
Funding This work was supported in part by the Institut de Médecine et d'Epidémiologie Appliquée and received additional grants from ANRS (Agence Nationale de Recherche sur le Sida et les Hépatites). Gilead Sciences provided an unrestricted grant for the French HIV-HBV cohort and was not involved in any part of the data collection, analysis, and writing. Postdoctoral fellowships from the ANRS and SIDACTION were awarded to AB.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Hôpital Pitié-Salpêtrière and Hôpital Saint-Antoine Ethics Committees (Paris, France).
Provenance and peer review Not commissioned; externally peer reviewed.