Article Text

Statistics from Altmetric.com
Dear Sir,
Primary sclerosing cholangitis (PSC) is a progressive disease of unknown aetiology. The presumed involvement of the gut–liver axis in disease pathogenesis1 has prompted investigations into mucosal2 and faecal intestinal microbiota composition, as has been reported by Kummen et al3 in this journal. Microbiota as diagnostic biomarkers of disease are of interest from the clinician’s point of view and Kummen et al3 have suggested a panel of taxa and even a single genus (Veillonella) with a reasonable diagnostic accuracy differentiating PSC and healthy controls (HCs).
We here report on a cohort study from northern Germany, using stool samples of 98 HC subjects, 73 patients with well-characterised PSC and 88 subjects with UC for 16S rDNA sequencing of the V1-V2 variable region. The PSC subgroup included 38 subjects with concomitant UC (PSC-UC). The data were subjected to quality control and operational taxonomic units (OTU) picking according to the methods described.3 Of the 12 taxa proposed to be differentially abundant in PSC cases and controls, 10 could be re-obtained in our dataset, whereas the taxa RF32 and Succinivibrio could not be recovered. Logistic regressions were fitted for the classification between HC and all PSC cases, all PSC and UC cases and PSC cases with and without concomitant UC, using either the arcsine square root transformed abundance of the Veillonella genus only, or all of the ten taxa proposed by Kummen et al.
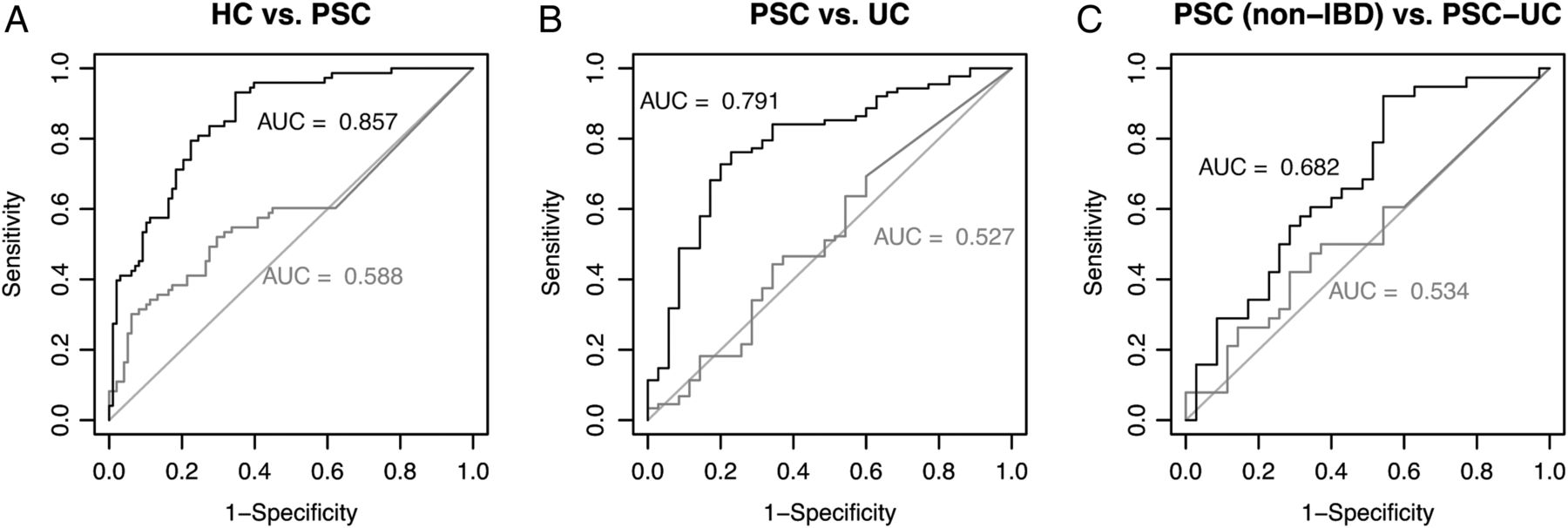
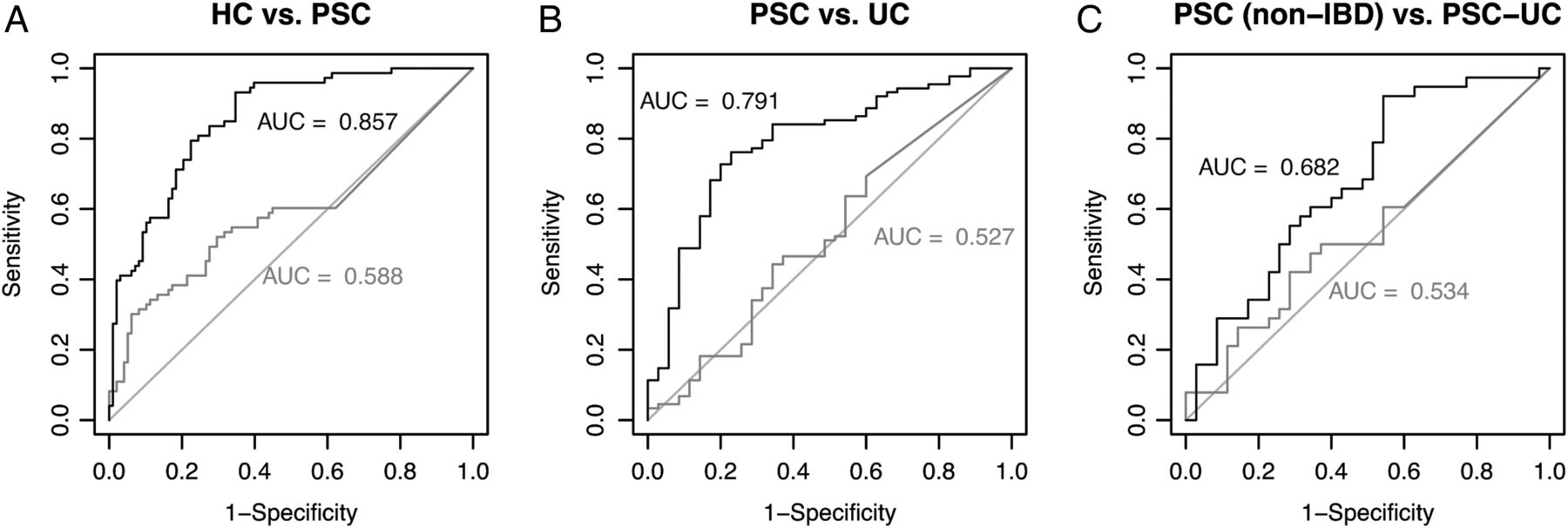
Whereas we can confirm in our study that Veillonella are more abundant in PSC compared with HC, there was no difference between PSC and UC, contrasting the results of Kummen et al (figure 1). Area under receiver operating characteristic (AUROC) analysis showed, that the Veillonella abundance is not sufficient to make a distinction between any of the groups in the dataset, resulting in area under the curve (AUC) <0.6 in each of the pairwise comparisons (figure 2). Using the transformed abundances of the complete set of 10 taxa and subjecting the same data for classification increases the AUC to 0.857 and 0.791 for HC versus PSC and PSC versus UC, respectively, presenting similar values as in the original publication. Splitting the dataset into training (2/3) and evaluation set (1/3) and repeating fitting and classification 1000 times yields a mean AUC of 0.7942 and 0.5816 for HC versus PSC and PSC versus UC, respectively. The distinction between PSC (non-IBD) and PSC-UC was not possible using these 10 taxa (AUCPSC (non-IBD) versus PSC-UC=0.682).

Abundance of the genus Veillonella in the different subgroups of the dataset. p Values obtained from pairwise Wilcoxon rank-sum tests. HC, healthy control; PSC, primary sclerosing cholangitis. n.s., not significant; Rel, relative.
{kind=link}
{kind=link}
Gut microbiota-based classification using logistic regression models based on Veillonella abundance only (grey) and the combined taxa identified in Kummen et al3 (black). (A) Healthy controls versus patients with primary sclerosing cholangitis (PSC), (B) patients with PSC versus patients with UC, (C) patients with PSC (non- IBD) versus patients with PSC-UC.
Applying a Wald test to the maximum likelihood estimators of the model coefficient for the model discriminating HC and PSC shows that only 4 of the 10 taxa incorporated in the model contribute significantly to the outcome in our dataset: Veillonella (p<0.01), Clostridiales (p<0.001), Lachnospiraceae (p<0.01) and Coprococcus (p<0.01). Using these four taxa only, the mean AUC of 1000 repetitions splitting the data into training and evaluation set is 0.8137 for the differentiation between HC and PSC.
These results show that the findings of Kummen et al with regard to microbiota as diagnostic markers can, in parts, be replicated in an independent geographical cohort and using a different variable region of the 16S rRNA gene. The differentiation between PSC and HC using a subset of taxa previously identified yielded fairly good results, but the discrimination between UC and PSC using the same taxa was not convincing. Furthermore, discrimination between any of these groups using the abundance of the genus Veillonella only did not perform better than random. Further studies are needed to confirm these results in independent cohorts and to improve the accuracy for the discrimination between PSC (with or without associated colitis) and UC.
Footnotes
MCR and F-AH contributed equally.
AF and CS jointly supervised.
Contributors AF and CS designed the study. CS, RZ and WL provided patient data and material. MCR, F-AH and AF analysed the data. AF, CS, MCR and F-AH wrote the manuscript. All authors have read and approved the final version.
Funding This work was supported by the Deutsche Forschungsgemeinschaft (DFG), KFO306 and Cluster of Excellence ‘Inflammation at Interfaces’, the biobank popgen (the popgen 2.0 network is financed by the German Ministry of Education and Research (grant 01EY1103)) and the German Federal Ministry of Education and Research (BMBF) within the framework of the e:Med research and funding program (SysInflame grant 01ZX1306A).
Competing interests None declared.
Ethics approval Ethics committees of University of Kiel and University of Hamburg.
Provenance and peer review Not commissioned; internally peer reviewed.