Article Text

Statistics from Altmetric.com
Editor—The aetiology of inflammatory bowel disease (IBD) is complex and shows clear evidence of familial clustering,1-3 and genetic linkage studies suggest a number of susceptibility genes.4-12 Changes in mucin expression are a feature of IBD.13-17 In ulcerative colitis there is a depletion of mucus, while the reverse is true for Crohn’s disease.18 Since the gene that encodes a major component of gel forming mucin of the large intestine,MUC2, located on 11p15.5, shows a high level of genetically determined polymorphism in length,19-21 it has been considered as a potential risk factor in IBD.22We have previously shown that the allele lengths range in size between approximately 45 and 200 repeats as judged by cutting genomic DNA samples with the restriction enzymeHinfI.19 This corresponds to apomucin sizes ranging from Mr 400-760 000. It is our hypothesis that these differences have a functional significance by changing the properties of the mucins in terms of the amount of apomucin backbone available for glycosylation or altering the spacing between the cysteine rich domains which are involved in cross linking or both. Here we report the work of two groups which was aimed at testing the hypothesis that short alleles predispose to ulcerative colitis.
DNA was prepared from peripheral blood and digested withHinfI. Agarose electrophoresis was used to separate the HinfI fragments which were then transferred by passive blotting onto nylon membrane, and the membranes probed using the tandem repeat cDNA Smuc41 as probe.23Allele lengths were determined by comparison with molecular weight standards and samples containing alleles of known length. All the procedures were standard though the details differed in the two laboratories. Optimised conditions are described in Vinallet al 24 and a typical gel is shown in fig 1.

Photograph showing the MUC2 VNTR polymorphism detected using HinfI digested DNA in seven representative samples from the survey. The molecular weight markers (M) shown are the Raoul markers from Appligene.
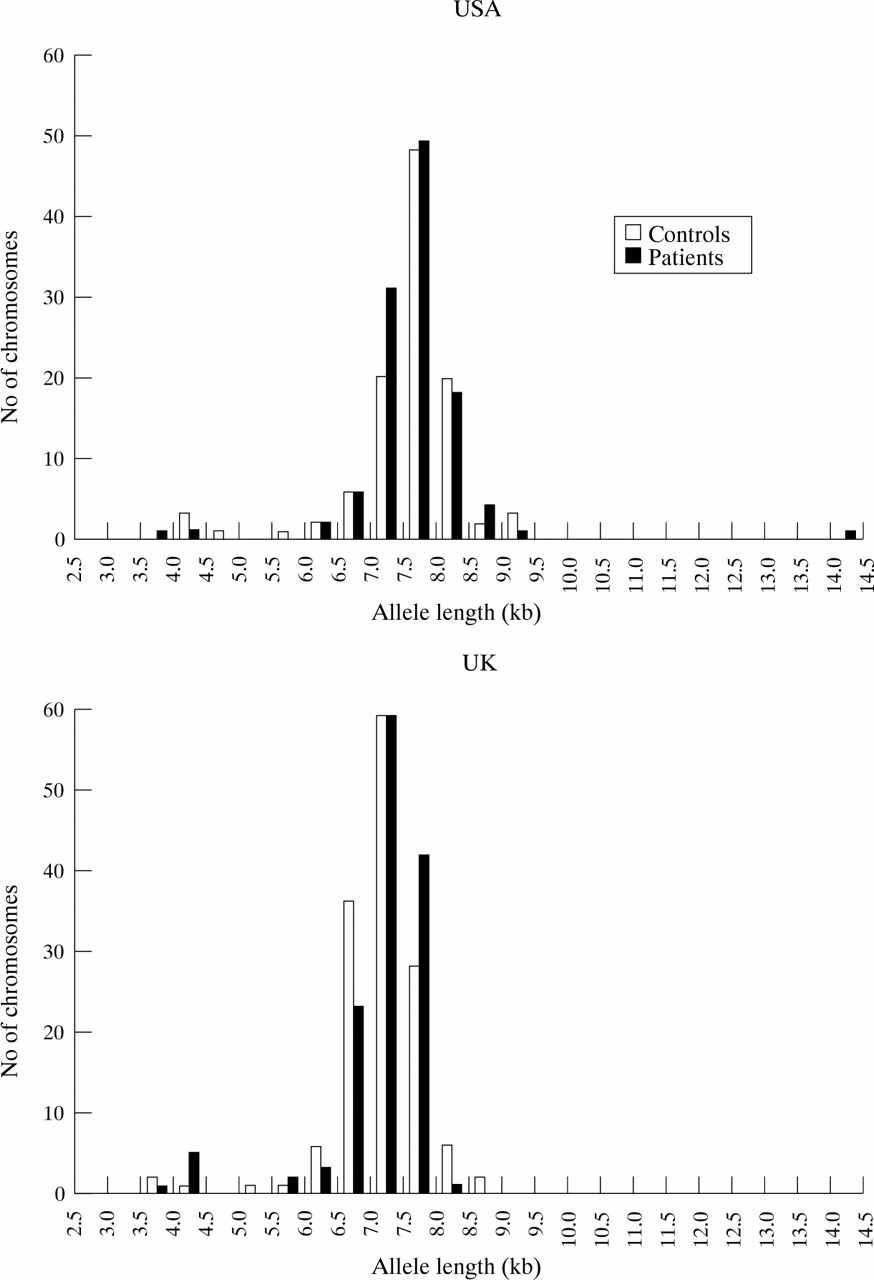
We examined a total of 125 genetically unrelated patients with inflammatory bowel disease (68 UK, 57 USA). As controls we tested a similar number of spouses and healthy volunteers. All subjects were of European origin although the American survey contained people from both southern and northern Europe and a large number of Jewish people. The data from the two laboratories were kept separate and the results are shown in fig 2. As can be seen, there is a very similar distribution of allele lengths in both studies. The slight right shift in the American population as compared with the UK population probably reflects subtle differences in the electrophoretic conditions used in each study. In both studies the short MUC2 alleles are very rare in patients as well as controls (6/136 UK patients and 3/142 UK controls, 2/114 USA patients and 4/106 USA controls), and there is no significant difference in the numbers of “small” alleles (smaller than 5.0 kb) and “large” alleles (greater than 5.0 kb) between patients and controls (Fisher’s exact test, UK data p=0.29, USA p=0.31). We also analysed the samples separately after exclusion of the Jewish subjects because of the suggestion of different genetic risk in Jewish and non-Jewish groups,25 26 but there was no difference in distribution (not shown). One subject in the USA group had one unusually large allele. The significance of this rare allele is not known though an allele approaching this in size (12 kb) is found in one of the CEPH families. Careful scrutiny of the large allele distribution shows slight but statistically non-significant difference in distribution in the patients and controls (Mann-Whitney U test, UK data set p=0.11, USA data set p=0.36) which is in the opposite direction in both groups.

{kind=link}
{kind=link}
Histogram showing the distribution of allele length in patients with ulcerative colitis and healthy controls. Sizes of the HinfI fragments were determined by comparison of their mobility with that of controls of known size. Subjects showing a single band were assumed to be homozygous for two alleles of the same size. The distributions were similar when Jewish people were excluded. All of the UK samples were taken from people of northern European extraction. The patients comprised 30 females and 38 males and their mean ages were 53 and 43 respectively and included six who were Jewish. Forty eight of the UK cohort had extensive colitis, 12 left sided colitis, and eight distal colitis. The UK controls comprised 33 females and 38 males, mean ages 37 and 44 (one Jewish). The USA samples were all from people of European extraction. The patients comprised 31 females and 26 males, mean ages 40 and 39 respectively (25 Jewish). Fifty six of the USA cohort were classified as suffering from ulcerative colitis and one from proctitis. The USA controls comprised 24 females and 29 males with mean ages of 42 and 41 (13 Jewish). All subjects were unrelated to each other and 28% of the UK cohort and 40% of the USA cohort had a known family history of inflammatory bowel disease.
This negative evidence seems to rule out the idea that shortMUC2 allele length predisposes to ulcerative colitis, but does not exclude the possibility that other variations in the MUC2 gene, such as “within repeat” sequence differences, or the final fully glycosylatedMUC2 mucin may play a role. Furthermore, in view of the recent results of Cho et al 12 it may be worth studyingMUC2 in Crohn’s disease since some evidence has been obtained for linkage of Crohn’s disease rather than ulcerative colitis to 11p.
Acknowledgments
LV was supported by the British Lung Foundation, MM was supported by the Sir Halley Stewart Trust, and JCWL was supported by the National Association for Colitis and Crohn’s Disease and by the Crohn’s Disease in Childhood Research Association.