Article Text

Abstract
Background—The frequency with which non-steroidal anti-inflammatory drugs (NSAIDs) increase small intestinal permeability and cause inflammation is uncertain.
Aims—To examine small intestinal permeability and inflammation in a large number of patients on long term NSAIDs.
Methods—Sixty eight patients receiving six different NSAIDs for over six months underwent combined absorption-permeability tests at three different test dose osmolarities (iso-, hypo-, and hyperosmolar). Two hundred and eighty six patients on 12 different NSAIDs underwent indium-111 white cell faecal excretion studies to assess the prevalence and severity of intestinal inflammation.
Results—The iso- and hyperosmolar tests showed significant malabsorption of 3–0-methyl-d-glucose, d-xylose, andl-rhamnose. Intestinal permeability changes were significantly more pronounced and frequent with the hypo- and hyperosmolar as opposed to the iso-osmolar test. Sequential studies showed that four and nine patients (of 13) developed inflammation after three and six months treatment with NSAIDs, respectively. There was no significant difference (p>0.1) in the prevalence (54–72%) or severity of intestinal inflammation in the 286 patients taking the various NSAIDs apart from those on aspirin and nabumetone, these having no evidence of intestinal inflammation. There was no significant correlation between the inflammatory changes and age, sex, dose of NSAID, length of disease, or NSAID ingestion.
Conclusions—Intestinal permeability test dose composition is an important factor when assessing the effects of NSAIDs on intestinal integrity. All the conventional NSAIDs studied were equally associated with small intestinal inflammation apart from aspirin and nabumetone which seem to spare the small bowel.
- non-steroidal anti-inflammatory drug
- intestinal permeability
- intestinal inflammation
- aspirin
- nabumetone
Statistics from Altmetric.com
Non-steroidal anti-inflammatory drugs (NSAIDs) are the most widely prescribed of the antirheumatic drugs, attesting to their efficacy as analgesic, anti-inflammatory, and antipyretic agents. A major concern with this group of drugs is the frequency and severity of gastrointestinal side effects.1 The precise magnitude of the problem is controversial and depends in part on the study population and/or the methods used to assess the damage.2
Most NSAIDs cause gastric damage in short term volunteer studies, ranging from erythema to ulcers.3 Cross sectional endoscopy studies in patients on long term NSAIDs show gastric erosions in 20–40% and gastric ulcers in 10–25% which have the potential to perforate and bleed.4-7 Small intestinal inflammation on the other hand is associated with blood and protein loss which may contribute to iron deficiency and hypoalbuminaemia.8-10
The gastric damage induced by short term usage of NSAIDs seems to be dose and formulation dependent.3 In the long term, NSAID ingestion is associated with a roughly equal frequency of gastric damage irrespective of drug formulation. However there is a ranking order of NSAIDs when it comes to the serious complications of gastroduodenal bleeding and perforation: azapropazone, indomethacin, and piroxicam usually head the toxicity list while ibuprofen and aspirin seem to be safer,11-13 possibly because of the lower doses used.14
The role of individual NSAIDs in small intestinal damage in man is less well characterised because of the difficulties of documenting and quantitating damage.9 ,15 ,16 Single dose volunteer studies show some difference in the potency of NSAIDs to increase intestinal permeability,17-19 but it is not known whether this applies to long term ingestion. Here various studies have suggested either a high prevalence of increased small intestinal permeability,20 no increased permeability,21infrequent changes only,22 or even colonic rather than small bowel permeability changes.23 One possibility for these discrepancies is that the various permeability test procedures used may differ in respect of their sensitivity. Furthermore it is not known whether the severity of NSAID enteropathy relates to the particular NSAID taken.
This study is in two parts. The first part assesses the prevalence of increased intestinal permeability and the relative sensitivity of three different test doses in patients on long term NSAIDs in order to resolve the controversy relating to the extent of intestinal permeability changes in patients on NSAIDs. The second part concerns a large number of patients with rheumatoid arthritis and osteoarthrosis who underwent indium-111 white cell studies to assess the prevalence and severity of NSAID enteropathy and to establish whether there is a ranking order of toxicities for different NSAIDs in the small intestine.
Patients and methods
INTESTINAL PERMEABILITY
Fourteen healthy Caucasian volunteers acted as controls for these studies (seven males and seven females, mean age 42 years, range 22–63 years). They were not receiving any treatment known to be associated with alterations in gastrointestinal function or gastrointestinal side effects.24
Sixty eight Caucasian patients with definite or classic rheumatoid arthritis (n=54) (American Rheumatism Association criteria) and osteoarthrosis (n=14) taking the same NSAID consistently for over six months were studied (16 males and 52 females, mean age 63 years, range 26–81 years). They were recruited from the rheumatology outpatient clinics at Northwick Park Hospital and King’s College Hospital. Patients were specifically excluded from study if they had significant cardiovascular, pulmonary, liver, or renal disease, or malignancy, or were receiving oral gold, sulphasalazine, or more than one NSAID.25 Patients receiving other drugs or those with other diseases associated with increased intestinal permeability24 were also excluded. All were admitted to a metabolic research ward during these studies.
Sixteen patients were on regular indomethacin (100–150 mg/day), 16 on naproxen (1000–1500 mg/day), 13 on piroxicam (10–20 mg/day), 11 on ibuprofen (1200–2400 mg/day), seven on flurbiprofen (50–300 mg/day), and six on sulindac (300–400 mg/day).
Each patient fasted overnight and took their particular NSAID at 7 00 am. This was followed by the ingestion of a 100 ml test solution at 8 00 am and a further two hour fast after which food and fluid were allowed. Complete five hour urine collections were made into a container containing 1 ml thiomersal (10% wt/vol aqueous) as preservative.
Table 1 shows the composition of the three test solutions used. The use of the four sugars in the iso- and hyperosmolar test solution allows the simultaneous assessment of four absorption-permeation pathways. The osmolarities were decided on the basis that these represent the most common test dose osmolarities used in studies of intestinal absorption-permeability and test dose osmolarity may play an important role in the sensitivity of the procedure.26 ,27 The tests were administered in random sequence, at least two days apart.
Compositions of the three test solutions used for the intestinal permeability studies
Sugar analysis in urine was performed by thin layer chromatography as previously described28 ,29 with scanning densitometry. These procedures are accurate and sensitive, recovery being above 90% and minimum level of reliable quantitation below 0.1 mmol/l. The precision lies between 3 and 8% (coefficient of variation) without replication over the test range of sugar concentration. The urine (5 ml aliquots) containing 51Cr-EDTA was counted in an LKB Wallac 1280 or 1282 (Upjohn-Pharmacia, Helsinki, Finland) along with a 1/500 dilution of the original test solution. Each sample was counted for five minutes which allows the minimum detectable activity of 0.03–0.05% of the administered test dose per litre of urine to be measured.
INTESTINAL INFLAMMATION
Twenty two patients (mean age 38 years, range 20–65 years) with irritable bowel syndrome acted as controls for the 111In white cell studies. Twelve and eight patients with untreated rheumatoid arthritis and osteoarthritis, respectively, acted as disease controls (mean age 56 years, range 23–83 years).
Sequential studies
Thirteen of the patients not on NSAIDs (seven with rheumatoid arthritis and six with osteoarthritis) underwent sequential111In white cell studies before, and three, and six months after starting indomethacin 100–150 mg/day (seven patients) or piroxicam 10–20 mg/day (six patients) and no other drugs, in order to assess the temporal relation between NSAID ingestion and the development of intestinal inflammation.
Cross sectional studies
The cross sectional study involved 286 patients (57 males and 229 females, mean age 62 years, range 18–86 years) with rheumatoid arthritis (n=253) and osteoarthrosis (n=33), taking the same NSAID consistently for over three months. These were recruited from the rheumatology outpatient clinics at Northwick Park Hospital and King’s College Hospital. All but 31 investigations were carried out as inpatients in a metabolic research ward. Exclusion criteria were the same as for the intestinal permeability studies.
The patients were on conventional NSAIDs: indomethacin 100–150 mg/day (n=52), naproxen 1000–1500 mg/day (n=58), piroxicam 10–20 mg/day (n=28), ibuprofen 1200–2400 mg/day (n=29), flurbiprofen 100–200 mg/day (n=16), ketoprofen 600–1200 mg/day (n=14), diclofenac 75–150 mg/day (n=38), and aspirin (n=7); or pro-NSAIDs: sulindac 300–400 mg/day (n=9), etodolac 400–600 mg/day (n=11), fenbufen 600–900 mg/day (n=11), or nabumetone 2 g/day (n=13).
Cell labelling
Neutrophils were isolated by sedimentation and centrifugation and labelled with 111In (30–300 μCi (1–11 MBq)) using tropolone as an ionophore as previously described15 and injected intravenously. The estimated radiation dose received during these studies was 0.7–6.5 millisieverts (effective dose equivalent). The higher dose of 111In was used if abdominal scintigraphy was performed and the lower dose if the study was confined to stool collections.
Individual stools were collected over a four day period after injection of the labelled cells and counted in a high resolution bulk sample counter along with standards for 20–60 seconds to allow measurement of 0.1–0.01% (low and high dose, respectively) of the injected dose with a counting accuracy of ±4%.
STATISTICS
The SYSTAT statistic package (for the Macintosh) was used for calculations. Spearman’s correlation coefficient was used to assess correlations. The paired Student’s t test was used for sequential studies, one way analysis of variance (ANOVA) for assessing differences between groups, or χ2 test as appropriate.
Results
INTESTINAL ABSORPTIVE CAPACITY AND INTESTINAL PERMEABILITY
Iso-osmolar test solution
Table 2 shows the five hour urinary excre- tion of 3–0-methyl-d-glucose, d-xylose, andl-rhamnose and the differential urinary excretion of lactulose:l-rhamnose. Patients on NSAIDs excreted significantly less (p<0.05) monosaccharides than controls; two to seven patients (33–43%) in each group had levels below the control lower limits (below −2SD).
Intestinal absorptive capacity and intestinal permeability assessed at three different test dose osmolarities
The excretion of lactulose did not differ significantly from control levels, but intestinal permeability as assessed by the differential urinary excretion of lactulose:l-rhamnose was significantly (p<0.05) increased with an average twofold increase from control levels. Three to five patients (24–50%) in each group had values above the control range. There were no significant differences (p>0.2) in the frequency or severity of the permeability changes in patients receiving the different NSAIDs.
Hyperosmolar solution
Control excretion values for monosaccharides and intestinal permeability did not differ significantly from the iso-osmolar test dose (table 2). Monosaccharide excretion was significantly (p<0.05) decreased in patients on NSAIDs compared with controls and the same patients had values outside the lower limit as with the iso-osmolar test.
The differential urinary excretion of lactulose:l-rhamnose was significantly (p<0.05) increased in each group of patients on NSAIDs. In each group, 50–81% of patients had values above the control range which was significantly (p<0.02) greater than that following the iso-osmolar test.
There were no significant differences in absorptive capacity or the differential urinary excretion of lactulose:l-rhamnose between patients on different NSAIDs.
Hypo-osmolar test
The urinary excretion of l-rhamnose did not differ significantly from control levels in any of the patient groups on NSAIDs (table 2). The differential excretion of51Cr-EDTA:l-rhamnose was significantly increased in each group of patients on NSAIDs. The discrimination between controls and patients on NSAIDs (50–90% of patients in each group) was comparable with that obtained with the hyperosmolar test and significantly (p<0.01) greater than with the iso-osmolar test dose. There were however no significant differences (p>0.3) in the frequency or severity of the permeability changes in subjects on different NSAIDs as assessed by the differential urinary excretion of51Cr-EDTA:l-rhamnose.
111In WHITE CELL STUDIES
The mean (SD) normal four day faecal excretion of111In white cells was 0.46 (0.23)% (range 0.05–0.98%) of the injected dose. The absolute upper limit (0.98%) was used to define normal-abnormal excretion of 111In white cells.
Patients with untreated rheumatoid or osteoarthritis had mean111In excretion values (0.59 (0.31)%, range 0.09–1.21%) which did not differ significantly (p>0.6) from normal controls.
Sequential studies
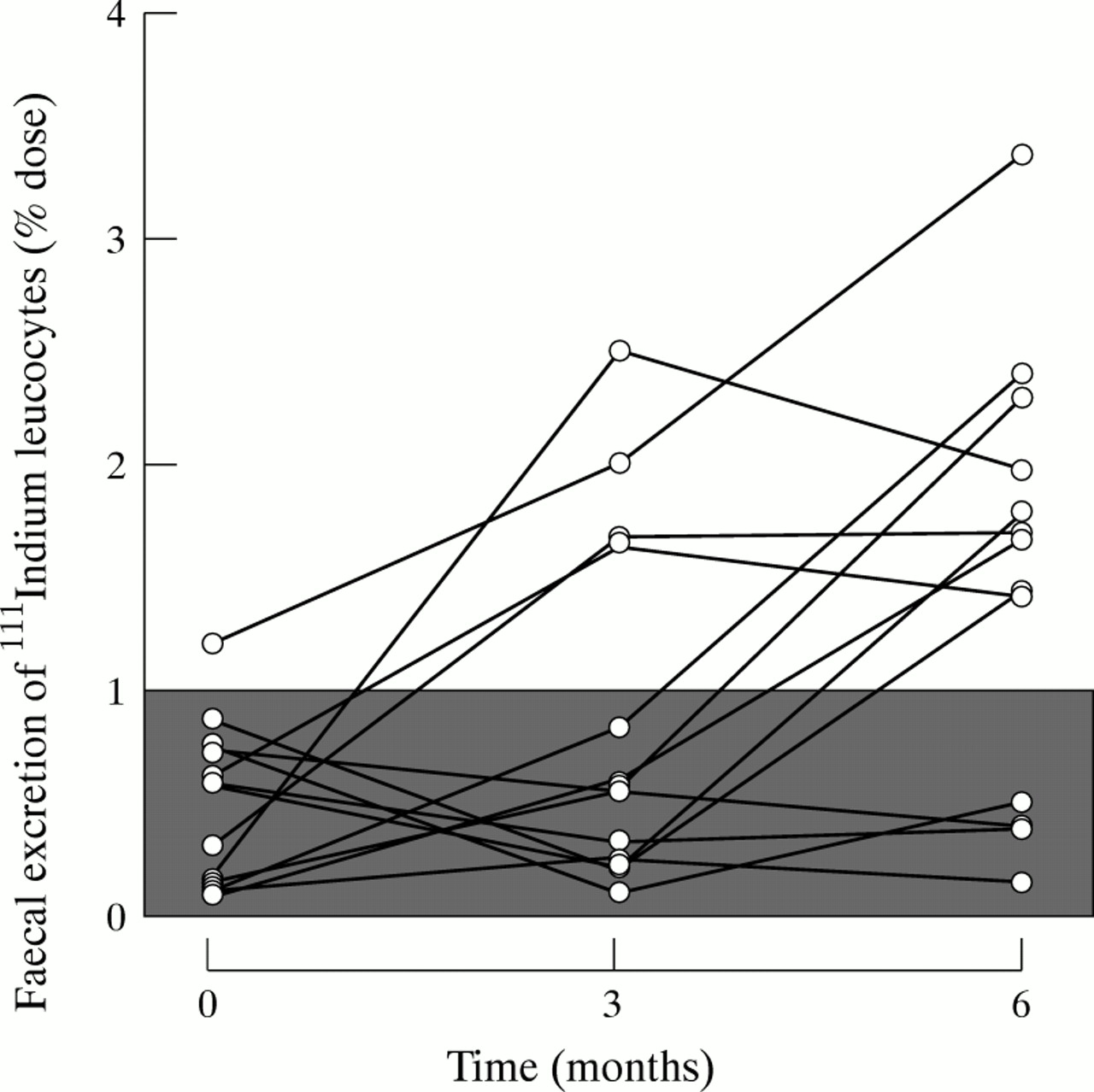
Figure 1 shows the sequential changes in the faecal excretion of111In in subjects taking indomethacin or piroxicam. By three months on the drugs four patients were clearly abnormal and at six months nine of 13 had intestinal inflammation.

{kind=link}
Sequential changes in the four day faecal excretion of111In white cells in response to indomethacin or piroxicam ingestion. The shaded area represents the normal range of excretion of the labelled cells.
Cross sectional studies
Table 3 shows that the mean four day faecal excretion of111In white cells was significantly (p<0.05) increased in patients taking different NSAIDs except in those on aspirin and nabumetone who did not differ significantly from controls (one of seven on aspirin and two of 13 patients on nabumetone had intestinal inflammation as assessed by the faecal excretion of 111In white cells).
Intestinal inflammation in patients on long term NSAIDs
There was no significant difference (p>0.1) in the prevalence of intestinal inflammation in patients taking the various NSAIDs (apart from aspirin and nabumetone), the proportion of patients with abnormal results being 54–72%. Within each group of patients on NSAIDs there was no significant correlation (r ranged from −0.11 to 0.17, p>0.1) between the faecal excretion of 111In and age, sex, dose of NSAID, length of disease, or NSAID ingestion.
Discussion
The present study shows that long term NSAID ingestion is associated with mild malabsorption and that the different formulations of intestinal absorption/permeability tests vary in their sensitivity to detect the effects of NSAIDs on the small intestine. Sequential studies of patients receiving NSAIDs show that ingestion of the drugs leads to intestinal inflammation. The prevalence and intensity of the inflammation associated with different NSAIDs, apart from nabumetone and aspirin, is comparable.
Intestinal permeability is thought to be a prerequisite for the development of NSAID enteropathy.24 ,30 ,31 However, there is a wide discrepancy in the reported prevalence of permeability changes in patients on NSAID treatment, ranging from 80% to nil.21 ,23 The reason for these discrepancies is not clear.24 ,32 The present study shows a notable difference in the sensitivity of the different test procedures which depends on test dose composition. Such differences in sensitivity may explain the failure of some studies to show significant effects of NSAIDs on small intestinal permeability,21 ,23 ,26 especially as iso-osmolar test solutions were used. Others used a hyperosmolar test solution,22 achieved by addition of lactose and sucrose, intestinal hydrolysis of which introduces a variable which has considerable indirect effects on absorption and permeability estimations.32-35 The way in which different dose osmolarities affect the sensitivity of absorption/permeability the tests is complex,36-38 but it is suggested that the hypo- (14 mmol/l) and hyperosmolar (1500 mmol/l) solutions exert a physiological stress on the intestinal mucosa. A damaged or diseased intestinal mucosa may be more susceptible to such effects.26 ,36-38
NSAIDs do not cause malabsorption when given short term,18 ,19 but malabsorption of d-xylose has been documented in patients on long term NSAID treatment.39 Here we show that the absorption of 3–0-methyl-d-glucose and l-rhamnose is also affected, but the malabsorption is relatively mild,40 ,41and certainly insufficiently severe to cause malnutrition by itself.
The sequential study shows a 12–24 week time interval between commencement of NSAID treatment and the development of intestinal inflammation. This contrasts with the demonstration of intestinal inflammation within two weeks of NSAID ingestion when the faecal calprotectin concentration is used as a marker of intestinal inflammation.42 The reason for these differences is uncertain. One possibility is that the 111In white cell technique may underestimate somewhat the severity of intestinal inflammation as in active arthritis there is often increased synovial, liver, and splenic sequestration of the cells which would reduce the number available for migration to the intestine.
The cross sectional study showed no significant differences (apart from aspirin and nabumetone) in the frequency or severity of intestinal inflammation in patients on conventional NSAIDs or pro-NSAIDs. This is in contrast to the different toxicity of NSAIDs according to serious gastroduodenal outcomes (perforation and massive bleeding).11 ,12 The reasons for these apparent differences are likely to be methodological as well as biological.8 ,16 In respect of the gastroduodenal mucosa, short term endoscopy studies give different NSAID toxicity rankings from the serious outcome studies.3 ,11 ,12 At the same time cross sectional endoscopy studies do not shown a significant difference in the prevalence of gastroduodenal ulcers in patients on different NSAIDs43-46 which is in general agreement with what we have found in the small intestine. A potential problem with the above long term studies is the variability in the daily dose of NSAIDs which might obscure a dose effect relation if one existed. Nevertheless it seems likely that the particular factors which determine the development of gastroduodenal ulceration and small intestinal inflammation in patients on long term NSAID treatment differ from those that account for the short term gastroduodenal lesions and the predisposition of ulcers to bleed and perforate in the longer term.
In our study two NSAIDs were associated with less small intestinal inflammation than the others, namely aspirin and nabumetone. Interestingly the same drugs do not increase small intestinal permeability in man19 or cause small intestinal inflammation in the experimental rat even at very large doses.47-49 The possible reasons for the lack of small intestinal inflammation associated with these drugs may relate to their site of absorption and lack of excretion in bile. Aspirin, an acidic NSAID, is mostly absorbed through the gastroduodenal mucosa,50 ,51 while nabumetone is non-acidic and therefore not trapped within enterocytes during drug absorption. Aspirin and 6-methoxy-2-naphthylacetic acid, the active metabolite of nabumetone, are the two NSAIDs that are not excreted in bile in significant amounts.47 ,52 ,53 Hence the small intestinal mucosa may not be exposed to significant quantities of these drugs so that the “topical” phase of damage is largely avoided.31 ,49 At this conjecture it is relevant that cyclooxygenase-1 knockout mice, that produce virtually no intestinal prostaglandins, do not develop gastrointestinal lesions spontaneously,54 re-emphasising that simple inhibition of cyclooxygenase is insufficient by itself to account for all of the gastrointestinal damage of NSAIDs.48 ,55 ,56
In summary, these studies show that intestinal permeability test dose composition and osmolarity are important factors when assessing the possible effects of NSAIDs on intestinal integrity. Long term ingestion of all the conventional NSAIDs studied was equally associated with small intestinal inflammatory changes apart from aspirin and nabumetone, both of which seem to spare the small bowel.
Acknowledgments
GS was supported by the Helga Jonsdottir and Sigurlidi Kristjansson Memorial Fund, Iceland, and JT by an NHS Executive R&D grant.