Article Text

Statistics from Altmetric.com
1.0 INTRODUCTION
Acute upper gastrointestinal bleeding is the commonest emergency managed by gastroenterologists. It has an incidence ranging from approximately 50 to 150 per 100 000 of the population each year, the incidence being highest in areas of the lowest socioeconomic status. An audit of patients admitted to hospital in the UK published in 1995 reported 11% mortality in patients admitted to hospital because of bleeding and 33% mortality in those who developed gastrointestinal bleeding while hospitalised for other reasons.1 Most deaths occur in elderly patients who have significant comorbidity and the majority are inevitable, despite improvements in medical and surgical expertise. Mortality is reported to be lower in specialist units2,3 and this is probably not related to technical developments but because of adherence to protocols and guidelines. Thus guidelines do have the potential to improve prognosis and in addition may be of value in making the best use of resources by fast tracking low risk patients, thereby optimising duration of hospital stay.
“Medline” and “EMBASE” were searched to identify the evidence used in formulating these guidelines. The term “gastrointestinal hemorrhage” was used to identify general reviews, leading articles, meta-analyses, and randomised clinical trials. Not all of the recommendations have been subjected to clinical trial but represent what, in the view of the British Society of Gastroenterology (BSG) endoscopy committee, defines best clinical practice. Guidelines cannot replace clinical judgment in the management of any specific patient. Best management depends on close cooperation between medical and surgical gastroenterologists and “combined care” is essential in managing the critically ill bleeding patient.
The specific management of acute variceal haemorrhage is a special subject and is not considered in detail.
1.1 Grading of recommendations
Grade A
-
Evidence from large randomised clinical trials
-
Meta-analysis
Grade B
-
High quality study of non-randomised cohorts who did not receive therapy
-
High quality case series
Grade C
-
Opinions from experts based on arguments from physiology, bench research, or first principles
1.2 Definitions
-
Haematemesis is vomiting fresh red blood.
-
Coffee ground vomiting is vomiting of altered black blood.
-
Melaena is the passage of black tarry stools.
-
Haemochezia is the passage of red blood per rectum; this is usually due to bleeding from the lower gastrointestinal tract but occasionally can be due to massive upper gastrointestinal bleeding. In general, patients who present with haematemesis and melaena have more severe bleeding than those who present with melaena alone (grade C).
-
Rebleeding is defined as fresh haematemesis and/or melaena associated with the development of shock (pulse greater than 100 beats/min, systolic pressure less than 100 mm Hg), a fall in CVP greater than 5 mm Hg, or a reduction in haemoglobin concentration greater than 20 g/l over 24 hours. Rebleeding should always be confirmed by endoscopy.
1.3 Causes
A cause for upper gastrointestinal bleeding is found in approximately 80% of cases. The underlying diagnoses are defined in table 1.
2.0 STAFF FACILITIES, PLANNING, AND RECORDS
The evidence base for this section is relatively sparse. What follows is a consensus position reached by the BSG endoscopy committee, informed by the opinion of practising clinicians, and reflects current optimal clinical practice.
2.1 Staff
Patients admitted following a diagnosis of acute upper intestinal bleeding should be the responsibility of the medical or surgical gastroenterologist who collaborates with a consultant in the other discipline. Ideally, specialist gastroenterologists (physicians or surgeons) should admit these patients. When local circumstances do not permit this, referral from the admitting general physician or surgeon to the specialist gastroenterology unit in the hospital is acceptable. Medical and surgical staffing at junior levels should be adequate to allow 24 hour observation and care. Experienced nursing staff should be available for the care of critically severe ill patients at a staff/patient ratio compatible with a high dependency unit.
2.2 Admission arrangements
Patients with upper gastrointestinal bleeding should be admitted or transferred to a safe environment. This is usually an acute general medical ward where the staff have experience of the problem. Severely ill patients are best admitted to a high dependency unit or intensive care unit. Some hospitals admit all patients with upper gastrointestinal to beds designed for the treatment of gastrointestinal bleeding.2,3 Such “bleeding units” are often jointly managed by medical and surgical staff. All units admitting these patients must have round the clock expertise, including emergency endoscopy.
2.3 Blood transfusion
A 24 hour blood transfusion service as part of the National Quality Control Scheme must be available. The laboratory should keep a supply of group O rhesus negative blood for emergency use.
2.4 Endoscopy
Facilities must be available for upper gastrointestinal endoscopy. No clinical trials have shown that diagnostic endoscopy reduces mortality but there is consensus among gastroenterologists that accurately defining the cause of haemorrhage aids management and, as will be discussed later, therapeutic endoscopy improves prognosis in patients who present with severe bleeding. Therefore, the great majority of patients admitted to hospital following a bleed can be safely endoscoped on an early elective list (ideally the morning after admission); a minority of cases need emergency “out of hours” endoscopy and this must be available 24 hours a day, seven days a week. A rota of endoscopists skilled in diagnostic and therapeutic measures is necessary. Endoscopy is best undertaken in a fully equipped endoscopy unit staffed by nurses trained in the care of ill patients and in the maintenance and use of endoscopes and their accessories. In some institutions emergency out of hours endoscopy may be more safely undertaken in an operating theatre environment when anaesthetic cover is available. Equipment must be available for cardiorespiratory monitoring during and after endoscopy. Endoscopy can obviously also be undertaken on the general ward but, although there are no comparisons of this with endoscopy done in a dedicated suite or in an operating theatre, it is our opinion that this is generally not appropriate; patients who have mild to moderate bleeding can be endoscoped next day in the unit while shocked or severely bleeding patients who require out of hours endoscopy need high intensity support which is generally unavailable on the ward.
Minimum standards for routine and emergency endoscopy, applicable to all institutions undertaking these procedures, have been defined.4
2.5 Protocols
An agreed protocol for the management of upper gastrointestinal haemorrhage should be distributed to all medical and nursing staff who care for such patients. This includes medical, geriatric, and surgical wards, the admission unit, laboratories, and pharmacy.
2.6 Records
Details of admission and subsequent events must be clearly documented in patient records. A formal standardised endoscopy report should be issued. Specific items which have prognostic importance (see later) and therapeutic interventions (endoscopic, surgical, and drugs) must be accurately described.
3.0 MANAGEMENT
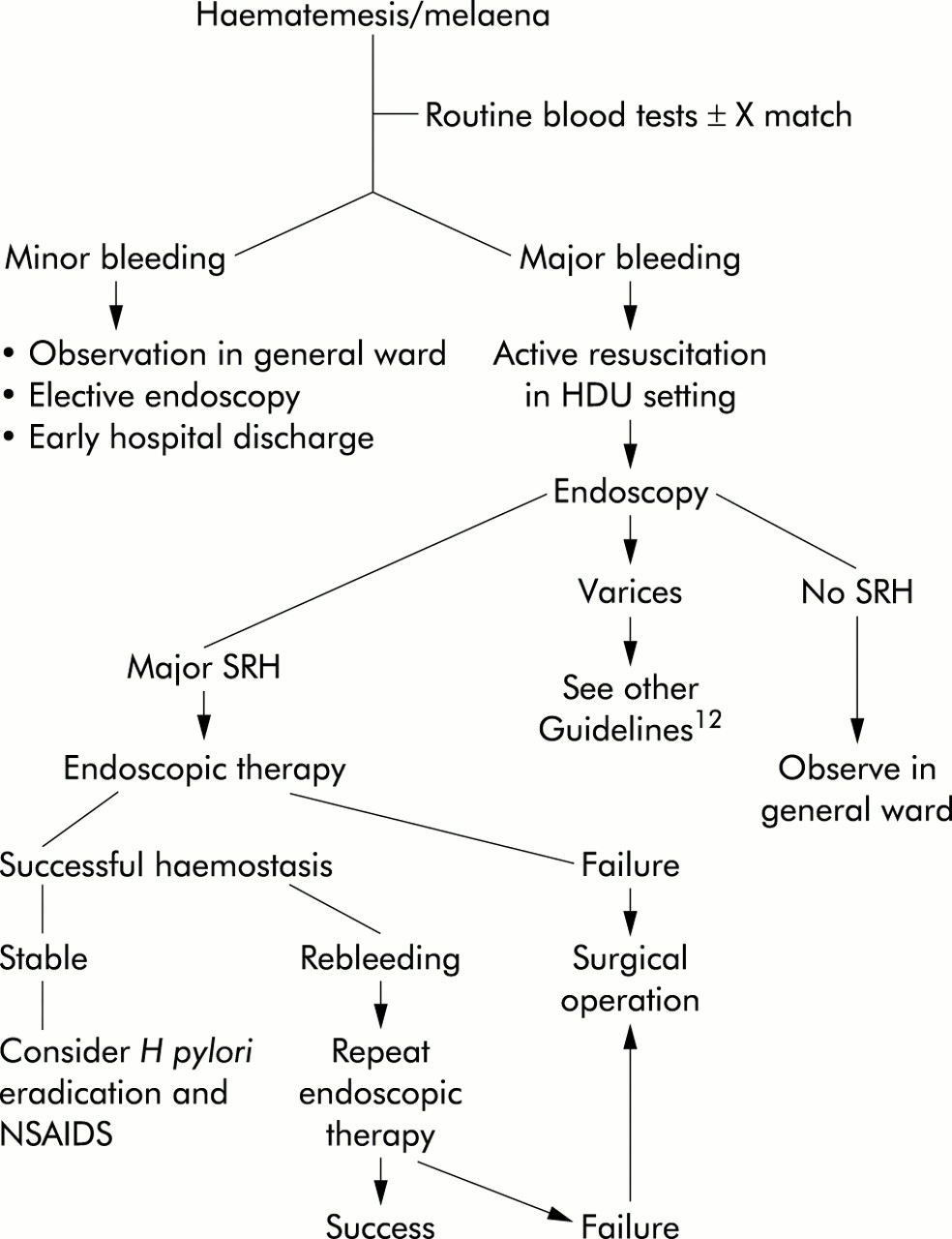
Management of any one patient is dictated by the severity and cause of bleeding and by the presence of other comorbid diseases. For example, a young healthy patient presenting with relatively minor bleeding should be fast tracked towards discharge from hospital while the elderly patient with multiple comorbidity and serious haemorrhage may be best managed in the high dependency unit (grade C). An algorithm summarising management steps is shown in fig 1.

{kind=link}
Algorithm for the management of acute gastrointestinal haemorrhage. HDU, high dependency unit; NDAIDS, non-steroidal anti-inflammatory drugs; SRH, stigmata of recent haemorrhage.
3.1 Assessment of bleeding severity
It is essential to categorise patients at the time of admission into high or low risk of death. Rockall et al defined independent risk factors (table 2) which were subsequently shown to accurately predict death5 (grade A). These comprise:
Increasing age. There is a close relationship between mortality and age. Deaths in patients under the age of 40 years are rare while the risk of death is 30% in patients aged more than 90 years.
Comorbidity. Deaths are almost entirely restricted to patients who have significant general medical diseases. These diseases are decompensated by bleeding, and postoperative complications are more likely to occur in patients who have significant comorbid illness. The number and severity of comorbid illnesses are closely related to mortality in patients hospitalised for gastrointestinal bleeding.6 Patients who have advanced renal or liver disease and those with disseminated cancer fare worst. It is crucial that complicating diseases affecting the heart, respiratory system, and central nervous system are recognised and appropriately managed.
Shock. Defined as a pulse rate of more than 100 beats/min and systolic blood pressure less than 100 mm Hg.
Endoscopic findings. Normal upper gastrointestinal endoscopy, Mallory Weiss tear, or the finding of an ulcer with a clean base are associated with a very low risk of rebleeding and death7,8 (grade A). In contrast, active bleeding from a peptic ulcer in a shocked patient carried an 80% risk of continuing bleeding or of death9 (grade A). A non-bleeding visible vessel is associated with a 50% risk of rebleeding in hospital9,10 (grade A). These risk factors can be scored as shown in table 2. A total score of less than 3 is associated with an excellent prognosis while a score greater than 8 is associated with a high risk of death5,11 (grade A).
Rockall scoring system for risk of rebleeding and death after admission to hospital for acute gastrointestinal bleeding
Patients with liver disease are a special case and guidelines for their management have been published.12 Their prognosis is related to the severity of liver disease rather than to the magnitude of haemorrhage.
3.2 Resuscitation
The first priority in management is to correct fluid losses and restore blood pressure. Thus in all patients intravenous access must be achieved. Comorbidity must be identified and appropriately treated. Routine blood tests (see box) are taken. The severity of bleeding is then estimated. Unfortunately, no current scoring system is applicable at this point because all of these include endoscopic findings, for example the utility of a modified Rockall score (that is, a score lacking endoscopic findings) has not been established. The definition of mild, moderate, or severe risk remains a matter of clinical judgement—in practice the severity of the bleeding episode and of comorbidity, as discussed below, are relatively easy to estimate. Scoring systems are much more relevant to clinical trials than day to day patient management.
Mild or moderate bleed. Pulse and blood pressure are normal and haemoglobin concentration is greater than 100 g/l. Patients have insignificant comorbidity and most will be less than 60 years of age. These patients are admitted to a general medical ward and if stable should be allowed fluids to drink. Pulse and blood pressure are measured hourly and urine volumes are measured. Endoscopy is undertaken on the next available list. If at endoscopy there are no stigmata of recent haemorrhage, varices, or upper gastrointestinal cancer, the prognosis is excellent and the patient is discharged at an early stage from hospital. Subsequent management is largely dictated by the final diagnosis and may include Helicobacter pylori eradication, the use of acid suppressing drugs, and advice concerning non-steroidal anti-inflammatory drug usage. In very low risk young patients who have sustained minor bleeding without haemodynamic compromise, it is perfectly reasonable to discharge the patient from hospital without undertaking endoscopy.
Severe. Such patients are usually aged more than 60 years, have a pulse greater than 100 beats/min, systolic blood pressure less than 100 mm Hg, and haemoglobin concentration less than 100 g/l. Most will have significant general medical diseases. Following initial resuscitation these patients are admitted and are closely monitored. A urinary catheter should be inserted and hourly volumes measured. Pulse and blood pressure are measured constantly using an automated monitor. In patients who have significant cardiac disease measurement of central venous pressure may clarify decisions concerning intravenous fluid replacement (although this has not been subjected to a formal clinical trial).
Blood tests taken urgently at initial presentation
-
Haemoglobin, platelet count, and white blood cell count
-
Urea and electrolytes
-
Liver function tests
-
Cross match
-
Prothrombin time
It is crucial to identify patients who have significant liver disease as these require specific management.12
The patient is fasted until haemodynamically stable and endoscopy is then undertaken.
3.3 Intravenous access and fluid replacement
In patients who are haemodynamically compromised, two large bore venous cannulae are placed in the anticubital fossae. For patients who do not have evidence of liver disease, normal saline should be infused to achieve a fall in pulse rate, rising blood pressure, central venous pressure, and adequate urine output. A clinical guide to the effects of volume depletion is shown in table 3.
Hypovolaemic shock: symptoms, signs, and fluid replacement
In most patients 1–2 litres of saline will correct volume losses. If after this the patient remains shocked, plasma expanders are needed as at least 20% of the blood volume has been lost. Adequately resuscitated patients have a urine output of more than 30 ml/h and a central venous pressure of 5–10 cm H2O.
It is necessary to transfuse blood (as red cell concentrate when):
Bleeding is extreme, as judged by active haematemesis and/or haematemesis with shock (see table 3). O negative blood can be given in extreme circumstances although this is only very rarely necessary as rapid cross matching is possible in standard transfusion laboratories.
When the haemoglobin concentration is less than 100 g/l (although it is perfectly reasonable to avoid blood transfusion at this level in patients who have chronic anaemia, for those who present with acute bleeding this haemoglobin concentration is a reasonable indication for blood transfusion; changes in cardiac output occur at this point and in critically ill ICU patients it is established that mortality is related to the severity of anaemia13).
3.4 Endoscopy
Endoscopy is undertaken either as a semi elective procedure in patients who have had relatively minor bleeding or it is done urgently in patients who have sustained major bleeding. It must be emphasised that endoscopy should only be done when resuscitation has been achieved. Ideally blood pressure and central venous pressure should be stable but in patients who are actively bleeding this is not always possible.
In clinical practice endoscopy is only rarely required “out of hours” but facilities must be available for urgent endoscopy if this is clinically necessary. In most patients endoscopy is best done in the endoscopy unit but an operating feature with full resuscitation equipment and the availability of an anaesthetist may be a better option in many institutes if endoscopy is “out of hours”. In severely bleeding patients, consideration should be given to endoscopy being done with an endotracheal tube in place to prevent pulmonary aspiration. Endoscopy should only be done by experienced endoscopists who are able to undertake therapeutic procedures, including those to achieve haemostasis from ulcers and varices. It is important that assistants who have been adequately trained and who are familiar with endoscopic equipment and their accessories are present.
Endoscopy is useful to define:
The cause of bleeding. Although the older literature suggested that diagnostic endoscopy did not improve prognosis,14 it is clearly important to identify patients who have varices, cancer, and ulcers with major stigmata.
Prognosis. As previously discussed, endoscopic findings are crucial in assessing the risk of further haemorrhage and of death, and steps should be undertaken to clearly identify the bleeding source. In practice, this may involve the use of catheters to wash bleeding points. Adherent blood clot is removed in order to expose an accurate target for endoscopic therapy.
To administer endoscopic therapy.
3.4.1 Endoscopic haemostasis
This is indicated:
In patients who have bled from oesophageal varices. Banding and injection sclerotherapy are described elsewhere.12
To treat ulcers with major stigmata of recent haemorrhage. Patients who have active bleeding whether it be spurting or oozing haemorrhage from the ulcer, a non-bleeding visible vessel, or have adherent blood clot should receive endoscopic therapy15 (grade A). Patients whose endoscopy shows a clean ulcer base, or black or red spots within the ulcer have a low risk of rebleeding and should not be treated endoscopically as their prognosis is excellent when treated conservatively.
A range of endoscopic treatments are available for treating patients who have major stigmata of recent haemorrhage. A meta-analysis of trials showed that endoscopic therapy reduced rebleeding, need for surgical intervention, and mortality15 (grade A). Endoscopic therapies can be classified as those based on injection, application of heat, or mechanical clips.
– (i)Injection. A disposable injection needle is used to inject a 1:10 000 adrenaline solution in normal saline. Injection is undertaken in quadrants around the bleeding point, then into the bleeding vessel using a total of 4–16 ml. This approach will achieve primary haemostasis in up to 95% of patients although bleeding will recur in 15–20% of these16 (grade A). There is little evidence that addition of other agents such as sclerosants (STD, polidoconal, and ethanolamine) reduces the rate of rebleeding and the use of these agents may cause life threatening necrosis of injected areas17–19 (grade A). Injection of absolute alcohol into the bleeding point does not confer advantages over adrenaline and also risks clinical perforation.20 Injection of agents which directly stimulate clot formation such as fibrin glue or thrombin have been shown to be effective21,22 but are not freely available.
– (ii) Application of heat. Thermal haemostasis is achieved using either the heater probe or multipolar coagulation (BICAP). Laser therapy is no longer used. The heater probe is applied at settings of 20–30 joules repeatedly until haemostasis is achieved and a blackened area is formed.23 Haemostasis is achieved by a combination of pressure (tamponade) and heat application and is as effective as adrenaline injection24 (grade A). The heater probe is useful because it includes a powerful water jet which aids removal of overlying blood clot. The efficacy of BICAP is similar to that of the heater probe25 (grade B). The Argon Plasma Coagulator has been shown to be effective in one trial of ulcer bleeding26 and further studies are required to determine its role. One trial showed that for the majority of ulcer bleeding patients, a combination of adrenaline injection plus the heater probe was no better than adrenaline injection alone in achieving permanent haemostasis. However, in a subgroup of patients who had active arterial bleeding, outcome was better in those receiving combination therapy27 (grade B).
– (iii) Mechanical clips. Mechanical clips can be applied to bleeding points and in clinical trials these perform well28 (grade B). Clips are particularly useful for actively bleeding large vessels but may be difficult to apply to awkwardly placed ulcers.
Mallory Weiss tears. These almost always stop bleeding spontaneously but occasional endoscopic therapy is needed to arrest severe haemorrhage. Endoscopic injection using adrenaline or thermal methods are almost always effective29 (grade C).
Vascular malformations, including telangiectasia and gastric antral vascular ectasia. These are probably best treated by application of heat using the Argon Plasma Coagulator or heater probe30 (grade B). Multiple sessions may be required before complete haemostasis is achieved.
Dieulafoy lesion is often difficult both to diagnose and treat. A range of therapeutic endoscopic modalities have been examined but no comparisons have been published. Uncontrolled series report success with band ligation, injection, and thermal methods31(grade C).
3.5 Drug therapy
Three classes of drug therapy have been examined in relation to non-variceal (principally peptic ulcer) bleeding.
Acid suppressing drugs. Their use is based on the observation that the stability of a blood clot is reduced in an acid environment. Thus a pH greater than 6 is necessary for platelet aggregation while clot lysis occurs when the pH falls below 6. There are no convincing data to support the use of H2 receptor antagonists, and these drugs do not reliably or consistently increase gastric pH to 6. In general, the proton pump inhibitor omeprazole has shown benefit in ulcer bleeding patients. A large two centre study in Nottingham in which patients received intravenous boluses of omeprazole or placebo showed lower endoscopic evidence of persistent bleeding in omeprazole treated patients but other end points, including mortality, were similar in both groups.32 A single centre study from Srinagar33 showed that ulcer bleeding patients receiving high dose oral omeprazole therapy rebled less often and required less blood transfusion than patients receiving placebo; endoscopic therapy was not used in this trial. Trials from Scandinavia,34,35 Taiwan,36 and Hong Kong37 have randomised patients to high dose intravenous omeprazole or placebo following primary haemostasis achieved by a range of endoscopic therapies. The most convincing study is that from Lau and colleagues37 who showed in a large study group that the rate of rebleeding, blood transfusion requirement, and duration of hospital stay were all less in omeprazole treated patients. Mortality tended to be less in this group although this did not achieve statistical significance. It seems unlikely that a better study will be available and since there are no data suggesting an adverse effects for omeprazole it is concluded that following successful endoscopic therapy in patients presenting with major ulcer bleeding, high dose omeprazole therapy (80 mg stat followed by an infusion of 8 mg hourly for 72 hours) is recommended (grade B). There are no comparisons of outcome between duodenal, gastric, or stomal ulcer patients receiving omeprazole but in the absence of trial data it seems reasonable to recommend this treatment for all bleeding ulcer patients.
Somatostatin. High dose intravenous somatostatin suppresses acid secretion and reduces sphanchnic blood flow and is therefore theoretically an attractive potential haemostatic agent. A meta-analysis38 showed benefit for treated patients (grade A) but the quality of most of the individual trials is poor and currently there are insufficient data to advocate routine use of this drug.
Antifibrinolytic drugs. A meta-analysis has shown that tranexamic acid therapy, while not reducing ulcer rebleeding, does appear to reduce the need for surgical intervention and tends to reduce mortality in ulcer bleeding patients.39 This meta-analysis was probably disproportionately skewed by inclusion of an extremely large trial in which the mortality in cimetidine treated patients was surprisingly high.40 Further studies of tranexamic acid are necessary before it can be recommended as routine therapy.
4.0 MANAGEMENT FOLLOWING ENDOSCOPY
Patients who have major upper gastrointestinal haemorrhage must be closely monitored following endoscopy with continual observation of pulse, blood pressure, and urine output. Identification of rebleeding or of continuing haemorrhage (defined in section 2.0 above) is essential. Patients who are haemodynamically stable 4–6 hours after endoscopy with or without endoscopy therapy should be allowed to drink and start a light diet; there are no data suggesting that prolonged fasting is necessary in this group of patients.
Repeat endoscopy should be considered in the following circumstances:
if there is clinical evidence of active rebleeding, suggested by the passage of fresh melaena or haematemesis, fall in blood pressure, rise in pulse, or fall in central venous pressure. In some patients (see below) major rebleeding is an indication for surgical intervention without repeating endoscopy, but in most patients it is wise to endoscopically confirm rebleeding (grade C).
if there are concerns regarding optimal initial endoscopic therapy. Accurate injection or thermal therapy is sometimes extremely difficult in actively bleeding patients and suboptimal therapy may be all that is possible. In this group of patients repeat intervention 12–24 hours later is worthy of consideration (grade C). Currently however it is not recommended that routine endoscopy is undertaken in all patients following initial endoscopic treatment.
4.1 Uncontrolled haemorrhage and rebleeding
Active non-variceal gastrointestinal haemorrhage that cannot be stopped by endoscopic intervention needs an urgent surgical operation.
Patients who rebleed after an initial period of clinical stability should undergo repeat endoscopy to confirm further bleeding. If endoscopic stigmata of haemorrhage persist, endoscopic therapy should be attempted on one occasion. One clinical trial has shown that patients whose rebleeding is treated by further endoscopic therapy have at least as good a prognosis as those randomised to urgent surgery without repeat endoscopic therapy41 (grade A). Subsequent management is then very much a matter of clinical judgment and based on local experience and expertise. In some patients endoscopic appearances may suggest that a surgical operation is in the patient’s best interests. For most patients however an expectant policy of continuing observation and decision to perform an operation if rebleeding occurs for a second time is appropriate (grade C). Such decisions are based on the patient’s age and comorbidity, and endoscopic findings. For example, a giant posterior duodenal ulcer with multiple bleeding points is at high risk of further bleeding and semi urgent surgery may be best in this situation. In contrast, a lesser curve gastric ulcer in a younger patient who has little comorbidity would be best managed by an expectant policy in which operation is only done after two rebleeds.
4.2 Surgery: when, by whom, and what operation
A consultant surgeon should be informed about the possible need for surgery and make the decision to operate or delegate the operation to another person. An experienced anaesthetist should be informed, assess the patient’s fitness for operation, and decide whether the anaesthetic should be given by a consultant or delegated to someone else. Timing of an operation should avoid, if possible, the hours of midnight to 7am. Mortality after urgent surgery for bleeding peptic ulcer correlates with the preoperative APACHE 11 score42 (grade A).
There is only one clinical trial of different surgical procedures for bleeding duodenal ulcers.43 The rebleeding rate was lowest in patients having a gastrectomy to include the ulcer either with Billroth I or Billroth II reconstruction compared with those subjected to more conservative operations. However, the bile leak rate following gastrectomy was much higher and the overall mortality in the two randomised groups was the same. Historically, a vagotomy has formed part of the surgical procedure but in the era of powerful antisecretory agents this is unnecessary. The same study suggests that when a bleeding duodenal ulcer is under run, specific ligation of the gastroduodenal and right gastroepiploic arteries reduced the rebleeding rate to a similar level as a gastrectomy43 (grade B).
Gastric ulcers are probably best excised or treated by partial gastrectomy depending on their size and location. There is no clinical trial evidence to support any particular intervention and the decision should be made on an individual basis by an experienced surgeon (grade C). Where there is a suspicion of malignancy then partial gastrectomy is the operation of choice. If a patient with bleeding peptic ulcer is elderly and in poor physical condition, the minimum operation to stop the bleeding should be undertaken, either by local excision or under running of the ulcer (grade C).
4.3 Follow up
Patient who have bled from ulcers should receive standard ulcer healing therapy. In most cases this involves Helicobacter eradication and trials show that rebleeding is then extremely rare44 (grade A). Patients who have ulcers associated with non-steroidal anti-inflammatory drugs or aspirin should stop these drugs and are treated with oral proton pump inhibitors. There are conflicting data concerning H pylori eradication therapy in ulcer bleeding patients who are also taking non-steroidal anti-inflammatory drugs. Many centres advocate eradication therapy (grade C). If a patient needs, with good reason, to continue taking a non-steroidal anti-inflammatory drug after an episode of ulcer associated bleeding, the least damaging agent (ibuprofen)45 should be used with a proton pump inhibitor46 (grade A). Cyclooxgenase 2 specific anti-inflammatory drugs may also be considered.
Patients who have bled from gastric ulcers should undergo repeat endoscopy approximately six weeks after discharge from hospital to confirm ulcer healing and exclusion of malignancy. Proton pump inhibitor therapy should be continued until that point (grade C).
Endoscopic confirmation of duodenal ulcer healing following H pylori eradication is probably not necessary although the subgroup needing to continue non-steroidal anti-inflammatory drugs while receiving ulcer healing therapy probably should be re-endoscoped (grade C).