Article Text

Abstract
Background:Helicobacter pylori infection induces progressive inflammatory changes in the gastric mucosa that may lead to gastric cancer. Understanding long term effects resulting from the cure of this infection is needed to design cancer prevention strategies.
Methods: A cohort of 795 adults with preneoplastic gastric lesions was randomised to receive anti-H pylori treatment and/or antioxidants. At the end of six years of intervention, those who did not receive anti-H pylori treatment were offered it. Gastric biopsies were obtained at baseline, and at 3, 6, and 12 years. A histopathology score was utilised to document changes in gastric lesions. Non-linear mixed models were used to estimate the cumulative effect of H pylori clearance on histopathology scores adjusted for follow up time, interventions, and confounders.
Results: Ninety seven per cent of subjects were H pylori positive at baseline, and 53% were positive at 12 years. Subjects accumulated 1703 person years free of infection. A multivariate model showed a significant regression in histopathology score as a function of the square of H pylori negative time. Subjects who were H pylori negative had 14.8% more regression and 13.7% less progression than patients who were positive at 12 years (p = 0.001). The rate of healing of gastric lesions occurred more rapidly as years free of infection accumulated, and was more pronounced in less advanced lesions.
Conclusions: Preneoplastic gastric lesions regress at a rate equal to the square of time in patients rendered free of H pylori infection. Our findings suggest that patients with preneoplastic gastric lesions should be treated and cured of their H pylori infection.
- GC, gastric cancer
- IM, intestinal metaplasia or metaplastic multifocal atrophic gastritis
- MAG, non-metaplastic multifocal atrophic gastritis
- PMN, polymorphonuclears
- SMN, stromal mononuclears
- gastric atrophy
- dysplasia
- metaplasia
- Helicobacter pylori
- randomised trial
Statistics from Altmetric.com
- GC, gastric cancer
- IM, intestinal metaplasia or metaplastic multifocal atrophic gastritis
- MAG, non-metaplastic multifocal atrophic gastritis
- PMN, polymorphonuclears
- SMN, stromal mononuclears
Helicobacter pylori infection has been categorised as a class I carcinogen.1 Some randomised short term studies2–4 and one five year study from China5 have reported no change in the degree of intestinal metaplasia (IM) and atrophy after successful eradication. Some randomised controlled studies of H pylori treatment effect have been published. In our randomised trial in Colombia,6 there was significantly more regression of preneoplastic lesions among those who had cleared the infection after six years of follow up. Wong and colleagues7 reported that after five years of follow up, H pylori eradication significantly slowed the progression of precancerous lesions such as atrophy and IM. Sung and colleagues8 reported that after five years of follow up H pylori eradication had significantly reduced progression of IM and induced regression of gastric atrophy.
Uncontrolled H pylori treatment trials report that in studies of more than two years of follow up there is improvement of atrophy but not IM.9,10 Other reports11 have shown an improvement in atrophy and IM. Not surprisingly, studies of less than two years of follow up showed inconsistent results.12–16
A 2002 review17 of 51 selected reports from 1066 relevant articles concluded that there was general agreement concerning reversal of acute and chronic inflammation. Most studies showed improvement in atrophy after H pylori eradication but improvement of IM was not conclusive.
Studies on the long term natural history of chronic gastritis associated with H pylori18,19 have shown that non-atrophic gastritis progressed to glandular atrophy and IM over a period of 12 years. This finding supports the most accepted model of gastric carcinogenesis.20Helicobacter pylori gastritis represents the initial step in a process which in high risk populations may lead to multifocal atrophy and IM, gradually expanding from the antrum to the body.21 It has been estimated that the relative risk of gastric cancer (GC) is 18.1 and 4.6 among subjects with antral or body atrophy, respectively.22 A recent large study23 reported that after 7.5 years of follow up the cumulative GC incidence was significantly higher in H pylori positive subjects. The aim of this study was to evaluate the long term effects of H pylori eradication on histology over a period of 12 years.
METHODS
Study subjects, treatment, and follow up
Details of subject characteristics and results of the six year follow up of this trial were reported previously.6 Briefly, volunteers from a high risk GC area in Colombia were screened in 1991, and those with a histological diagnosis of preneoplastic lesions were randomly assigned to receive for two weeks anti-H pylori therapy (amoxicillin, metronidazole, and bismuth subsalicylate) and/or supplementation for six years with beta-carotene (30 mg once daily) and/or ascorbic acid (1 g twice a day) in a threeway factorial design. Subjects assigned to the anti-H pylori treatment arm who tested positive for H pylori at 36 months were retreated for 14 days (amoxicillin, clarithromycin, and either omeprazole or lansoprazole). After six years of follow up, the trial was unblinded. Anti-H pylori therapy was offered to those not treated, as recommended by the Data and Safety Monitoring Committee. Subjects were then followed for another six years.
Histopathology
Endoscopies were performed at baseline, and at 3, 6, and 12 years. At the time of each endoscopy, four biopsies were obtained: antrum adjacent to incisura angularis, antrum greater curvature (5 cm above the pylorus), antrum anterior wall, and corpus anterior wall. They were formalin fixed and paraffin embedded. Sections were stained with haematoxylin-eosin for regular histology, with Alcian blue-periodic acid Schiff24 to detect IM, and with the modified Steiner technique25 to detect H pylori.
To determine intraobserver variation in histology assessment over the 12 year study period, the same pathologist (JCB) who evaluated the biopsy specimens collected at baseline, 36, and 72 months was asked to blindly re-evaluate the global diagnosis of 20% (n = 127) of the samples randomly selected from 72 months of follow up. Interobserver variability was assessed by asking the second pathologist (MBP) to evaluate the same set of biopsies. Intra- and interobserver variations were evaluated and acceptable results were obtained (kappa values: 0.79 and 0.62, respectively). Biopsies at 12 years were examined independently by the above mentioned two pathologists unaware of treatment assignation and the results of preliminary histopathological evaluations. In case of disagreement, the relevant biopsies were re-examined simultaneously in a multihead microscope with a third expert pathologist (PC) until agreement was reached.
Multifocal atrophic gastritis, defined as loss of appropriate glands and subdivided as non-metaplastic or metaplastic following established criteria, was graded as indefinite, mild, moderate, or marked atrophy.26 Metaplastic multifocal atrophic gastritis (IM) was defined as replacement of the gastric epithelium by intestinal-type epithelium. It was further subclassified as complete (small intestinal-type), defined by the presence of absorptive enterocytes with brush border alternating with goblet cells, or incomplete (colonic-type), defined by the presence of columnar cells with foamy cytoplasm, lacking brush border.27 Dysplasia, defined by atypical cytological and architectural derangement, was graded as indefinite for dysplasia, low grade, and high grade.28 Chronic inflammation, activity, and density of H pylori colonisation were graded as mild, moderate, and marked, according to the updated Sydney system.29
Informed written consent was obtained from all participants. The Institutional Review Board of Louisiana State University Health Sciences Center and the Committees on Ethics of Universidad del Valle and Hospital Departamental de Nariño in Colombia approved the original protocol of this study.
Statistical analysis
Global diagnosis
Gastric lesions were classified using an increasing ordinal scale: 1 = normal, 2 = non-atrophic gastritis, 3 = non-metaplastic multifocal atrophic gastritis (MAG), 4 = IM, 5 = dysplasia (DYS), and 6 = GC. The most advanced lesion seen in each set of biopsies from every patient at each visit was considered as the global diagnosis.
Histopathology score
For analysis of the results, a score was developed giving numerical values to the subdivision of the global diagnosis. The score reflects extensive previous experience, which recognised the heterogeneity of each global diagnosis, as well as the previously reached expert’s consensus.26 Subdivisions recognise their prognostic value (table 1). Thus the greater the extent of gastric atrophy, the greater the cancer risk.30 The incomplete-type of IM carries a higher risk than the complete type.27 Histological grades of dysplasia are correlated with GC risk.28 The MAG score (3) was modified using a continuous scale: indefinite for atrophy (0.25), mild (0.50), moderate (0.75), and severe (1.0). The IM score (4) was modified according to type and extension. IM type was classified into four categories in an ordinal scale: complete-type (0.1), mixed predominant complete-type (0.2), mixed predominant incomplete-type (0.3), and incomplete-type (0.4). The average extension of the IM (number of biopsies with IM/total number of biopsies) was grouped by tertiles. Each tertile was given a value: 0.2, 0.4, or 0.6, respectively. In order to obtain a total score of IM, values for type and extension were added to the original score for IM (4). The dysplasia score (5) was modified using a continuous scale: indefinite (0.25), low grade (0.50), and high grade (0.75). For MAG, IM type, and dysplasia, the most advanced grade seen (maximum value) among different biopsies was taken. This augmented histopathology score, not the global diagnosis, was used for statistical analyses.
Description of the histopathology score values according to the histopathological diagnosis
Inflammatory parameters
Average values of polymorphonuclears (PMN) and stromal mononuclears (SMN) were estimated from the total number of biopsies in each endoscopy procedure, separately in the body and antrum. Transitional mucosa was considered antral.
Mixed linear and non-linear models
The statistical analysis utilised all instances of intervention (antioxidant supplement and anti-H pylori treatment at baseline, retreatment among those who failed therapy, and anti-H pylori treatment at six years) and all four sets of biopsies. Specifically, the analysis used the histopathology score from each patient through time, so that an individualised function of a curve’s shape over time could be ascertained. Short and long term, instantaneous, and/or cumulative effects of interventions over the histopathology score have to be determined for each patient and groups of patients. In the case of H pylori clearance, the time that the patients are not exposed to the bacteria needs to be considered so that the suitable differentiation is made between those who have cleared the bacteria for nine years, six years, a short period, intermittently, or cumulative periods thereof. Further adjustment was made for baseline variables (age, sex, weight, and height) and time dependent variables that may impact outcome, such as anti-H pylori treatment.
The statistical procedure was accomplished through the use of mixed linear and non-linear models. The scores for each patient are assumed to be correlated to subsequent scores over time. The patient is the unit of analysis, and the baseline score of each one is assumed to be different from each other. This histopathology score analysis is much more sensitive to changes over time than the progression-no change-regression categorical construct.
Fixed factors are divided into potential confounders (age, sex, weight, and height) and treatment allocation at baseline (antioxidant or anti-H pylori). Random effects are those that vary through time, such as H pylori clearance status, chronological time in years, and anti-H pylori treatment. The coefficients produced by the mixed model analysis have a natural interpretation as they correspond to change from baseline scores. They correspond to progression (positive coefficients) or regression (negative coefficients) of the histopathological lesions, and can be easily transformed into per cent change per year or per cent cumulative difference at six or 12 years. Stratified models by global baseline diagnosis were also considered.
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS version 11.0).
RESULTS
A total of 795 patients were included in this analysis. Of those, 679 came to the three year biopsy, 629 to the six year biopsy, and 609 to the 12 year biopsy. A total of 638 patients were biopsied on three or more occasions.
Table 2 shows baseline characteristics and their change through time. There were no differences in age, sex, height, or weight distributions at baseline according to the randomised assignment groups.
General characteristics of the participants during follow up
H pylori infection clearance and reinfection/recrudescence rate
Among patients that received anti-H pylori therapy at baseline (n = 394), eradication rates at 3, 6, and 12 years were 51% (171/336), 75% (239/320), and 51% (153/300), respectively. The clearance rate at 12 years among patients that did not receive anti-H pylori therapy at baseline but were offered and received it at the six year mark was 47% (84/180). The spontaneous clearance rate was 2.9% per year, and was calculated among subjects who did not receive anti-H pylori treatment and were positive at baseline, but became negative and were followed for six or 12 years.
The reinfection/recrudescence rate was 5.4% per year, and was calculated among subjects that were treated at baseline, not treated at six years, and their Helicobacter status was negative at six years, but positive at 12 years.
There was a strong and significant effect of age on spontaneous clearance and reinfection/recrudescence rates. Subjects younger than 50 years at baseline had smaller spontaneous clearance rates (1.6% per year) than patients over 50 years old (2.6% per year), while the former had larger reinfection/recrudescence rates (6.2% per year) than the latter (4.6% per year).
Histopathology score
The average histopathology score at baseline was 3.77 (95% confidence interval (CI) 3.68–3.86), so that an average subject had moderate to severe MAG. Those who cleared the infection had declining scores as a function of the square of time. At six years the score for those subjects was 0.13 less than baseline (95% CI 0.11–0.15) while at 12 years the score was 0.59 less than baseline (95% CI 0.51–0.67). Subjects never treated who remained infected had an increase in score of 0.18 at 12 years. Treated patients (at any point) who were still infected at 12 years (treatment failure) had a decrease in score of 0.19.
Analysis of the effects of baseline treatment allocation on histopathology score to 12 years showed that there was a significant effect of baseline anti-H pylori therapy (0.28 less than baseline, 95% CI 0.18–0.38) but no significant effect of antioxidants. Subjects treated with both antioxidant supplements and anti-H pylori therapy did not have additional benefit. Eliminating the non-significant variables, factors that predicted histopathology score through all 12 years of follow up were the square of time, H pylori status, and age. The effect of time could be measured among subjects who never received anti-H pylori therapy and were H pylori positive throughout the 12 year period.
Subjects who were H pylori negative at 12 years had 14.8% more regression and 13.7% less progression than subjects who were H pylori positive at 12 years (p = 0.001). The difference was less striking among subjects who were randomised to receive anti-H pylori treatment as those had 5.2% more regression and 2.1% less progression than subjects that did not receive anti-H pylori treatment at baseline (p = 0.364). Among those who received anti-H pylori treatment for the first time on completion of the intervention at six years, the effect was smaller and non-significant. At 12 years there was a non-significant effect of having received antioxidant supplementation for the first six years. Changes in the average histopathology score depending on their infection status at six and 12 years, but independent of treatment received, are shown in fig 1.

Histopathology score over time and Helicobacter pylori infection clearance.
A model that considered the fact that some subjects were treated at baseline and others at six years found that time dependent anti-H pylori treatment was significant (p = 0.0002) adjusted for age and clearance. This residual effect of treatment was not related to the fact that subjects cleared the bacteria.
Inflammatory changes
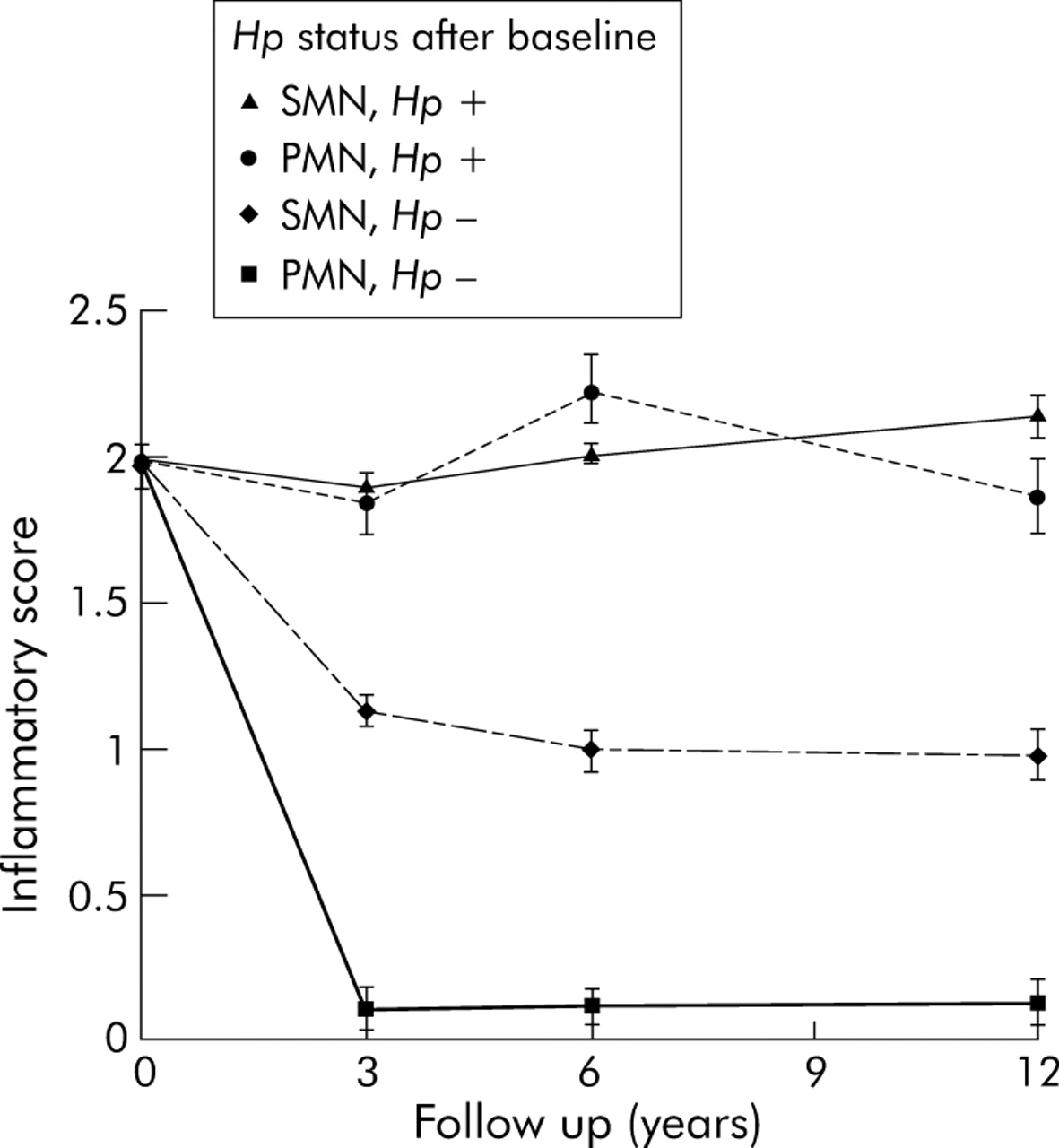
Eradication of H pylori reduced activity (PMN) in the antrum and corpus mucosa. A typical H pylori positive patient had at baseline an average PMN score in the antrum of 2.08 (0.11). If the subject received therapy and cleared the infection, his/her score was reduced at year 3 to 0.09 (0.06) (p<0.0001). This effect was maintained until 12 years (fig 2).

{kind=link}
{kind=link}
Acute and chronic inflammation score in the antrum over time according to Helicobacter pylori (Hp) status. PMN, polymorphonuclears; SMN, stromal mononuclears.
Regarding chronic inflammation (SMN), subjects that cleared the infection at year 3 had a significant decline in the antrum average score from 1.99 (0.13) (moderate) to 1.12 (0.26) (mild), with a continued less steep but significant decline to 0.97 (0.21) until year 12. Subjects that remained positive had a slow linear but significant (p = 0.008) increase in score over time (to 2.14 (0.2) at year 12) (fig 2). Subjects with MAG had the steepest declines if they cleared the bacteria, and also the sharpest increases if they did not. There was an interesting ladder effect with less advanced lesions behaving in step with more advanced lesions. This interaction between time, diagnosis, and clearance was statistically significant (p = 0.01). These changes were similar, but less marked, in the corpus, with slower declines but no differential effect by diagnosis*.
Gastric cancer incidence
There were nine new GC cases during the 12 years of follow up: five in the H pylori treatment group (four had dysplasia and one had IM at baseline) and four in the non-treated group (one had dysplasia and three had IM at baseline).
DISCUSSION
Our randomised placebo controlled study in a high risk GC area of Colombia documents a strong and significant effect of clearing H pylori infection towards the healing of gastric precancerous lesions after a follow up of 12 years. This effect is cumulative and compounded through time, so the longer the patient is free of the infection the faster and more thoroughly the healing occurs. For instance, a subject with moderate to severe MAG that cleared the infection and stayed negative for 12 years had mild or no atrophy. On the other hand, a patient that did not receive anti-H pylori therapy and remained positive during all 12 years had a slightly worse histopathology score. Moreover, 66% (46/70) of all subjects with MAG at baseline who were H pylori negative at the 12 year biopsy reverted to no atrophy, compared with 14% (9/66) among subjects that were positive (some of these subjects may have cleared the bacteria and become positive again). Additionally, 20% (70/182) of subjects with IM at baseline who were H pylori negative at 12 years had no atrophy or IM at that point, contrasted with 5% (9/183) among those who were H pylori positive.
The effect of clearing the bacteria on histopathology scores during a span of six years is only 10% of the effect that can be observed after 12 continuous years of healing, instead of the expected 50%. This disparity is explained by the typical S shape of exponential curves. The healing effect increases as a function of the square of time. The longer the patient is free of the bacteria the faster the gastric lesions heal. This finding indicates that the dynamics of the healing process after suppressing the carcinogenic agent parallel in reverse the carcinogenic effects of a given agent. Doll and Peto,31 in their study of the British doctors, reported that smoking increases lung cancer risk exponentially as a function of exposure time: K×(number of cigarettes/day)2×(exposure time)4.5.
The only significant baseline covariate which predicted the histopathology score through all 12 years of follow up was age, with older subjects having more advanced lesions and therefore higher histopathology scores than younger subjects at baseline. Older subjects none the less were more likely to clear the infection than younger subjects (p = 0.001), and when they did, they had a lower reinfection/recrudescence rate than younger subjects. This is probably related to the well known fact that the metaplastic mucosa is not a favourable niche for H pylori colonisation.32 Moreover, older H pylori positive subjects had a higher spontaneous clearance rate than younger subjects. Despite these advantages, older subjects were slower to heal than younger subjects, mainly because they started with more advanced lesions. This finding is consistent with the report from Wong et al that anti-H pylori treatment in subjects without precancerous lesions (no atrophy or IM) at baseline apparently succeeded in preventing cancer development.23
When all anti-H pylori treatments are considered, there is a significant reduction in histopathology score independent of clearance and age. This residual effect of anti-H pylori treatment in patients who did not clear the infection may be caused by clearing the bacteria over a short period of time, diminishing the bacterial burden, or to selective survival of less virulent genotypes of the bacteria after “unsuccessful” treatment, as reported previously in our subjects.33 Lesser mucosal damage is to be expected with less pathogenic strains.34 Although an antioxidant effect was observed at six years, it disappeared during the six years of no supplementation, and no residual effect was observed.
There seems to be a cause-effect relationship in the chain that involves first successful anti-H pylori treatments which in turn produce H pylori clearance and then promote healing of gastric lesions. Subjects who cleared the bacteria had the most consistent effect. Among treated subjects the effect was confounded by the fact that some treated subjects did not clear the bacteria. Independent of any treatment, subjects who were consistently H pylori positive had a non-significant small worsening in histopathology score through the 12 year follow up. Subjects that cleared soon after treatment and accumulated at least nine years of time without infection had the largest healing effect, equivalent to a patient with initially moderate MAG and then having no atrophy.
In this 12 year study, we confirmed previous observations regarding regression of atrophy and IM after successful eradication of H pylori. More importantly, the quadratic nature of the temporal relationship between disappearance of infection and healing of the mucosa explains previous negative findings for IM where the follow up was less than three years. These findings also indicate that regression of IM may be a long term process, taking many years after eradication of H pylori. We found no significant changes in dysplasia but there was a trend towards more regression and less progression among patients that remained consistently negative for infection. It is expected that a longer follow up with an adequate sample size may answer the question of the effect of H pylori clearance on dysplasia.
In accordance with previous studies we found that acute inflammation disappeared soon after H pylori treatment. Chronic inflammation responded at a slower pace but was still present, significantly lower, by 12 years.
Because gastric preneoplastic lesions have a multifocal presentation, one of the limitations of this study was the possibility of sampling error. Other limitations include difficulty in establishing the precise timing of reinfection/recrudescence and the fact that the study population had a very high H pylori baseline prevalence. Additionally, there was a lack of information about the use of antibiotics prescribed out of the trial. It could have influenced “spontaneous” H pylori clearance in subjects who did not receive anti-H pylori therapy.
This study has shown that the observed antioxidant effect was transient and disappeared after six more years of follow up while the anti-H pylori treatment effect persisted for as long as patients remained free of H pylori. Subjects with atrophic gastritis can indeed recover completely after a 12 year period without infection, and subjects with IM have a high probability of doing the same, although more time is presumably needed to heal completely. In conclusion, our study indicates that GC chemoprevention via eradication of H pylori infection is a viable option, but the greatest beneficial effects might not be evident in the first 3–6 years of observation. Finally, our findings suggest that patients with preneoplastic gastric lesions should be treated and cured of their H pylori infection.
Acknowledgments
We acknowledge our staff members at LSUHSC: Alberto Delgado, Violeta Sanchez, and Raquel Nin for processing of the biopsies. We thank the Hospital Departamental de Nariño Directors, past and present, and our field staff in Colombia: Tito Collazos and Stella Garcia, in Cali; Cristina Campo, Yolanda Mora and Alicia Rosero in Pasto. We also acknowledge the expert clinical contribution of our endoscopists Drs Luis Realpe and Guillermo Zarama.
This study was supported by a grant from the National Cancer Institute (PO1CA028842), by a grant from the Health Excellence Fund of the Board of Regents of the State of Louisiana (HEF 2000-05-03), and by a grant from the Instituto Colombiano para el Desarrollo de las Ciencias y Tecnología “Francisco José de Caldas” (1106-04-13075).
REFERENCES
Footnotes
-
Published online first 28 June 2005
-
Conflict of interest: None declared.
Linked Articles
- Digest
- Letter
- JournalScan
- Letter